NR 601 Final exam review Weeks 5-8 content
Document Content and Description Below
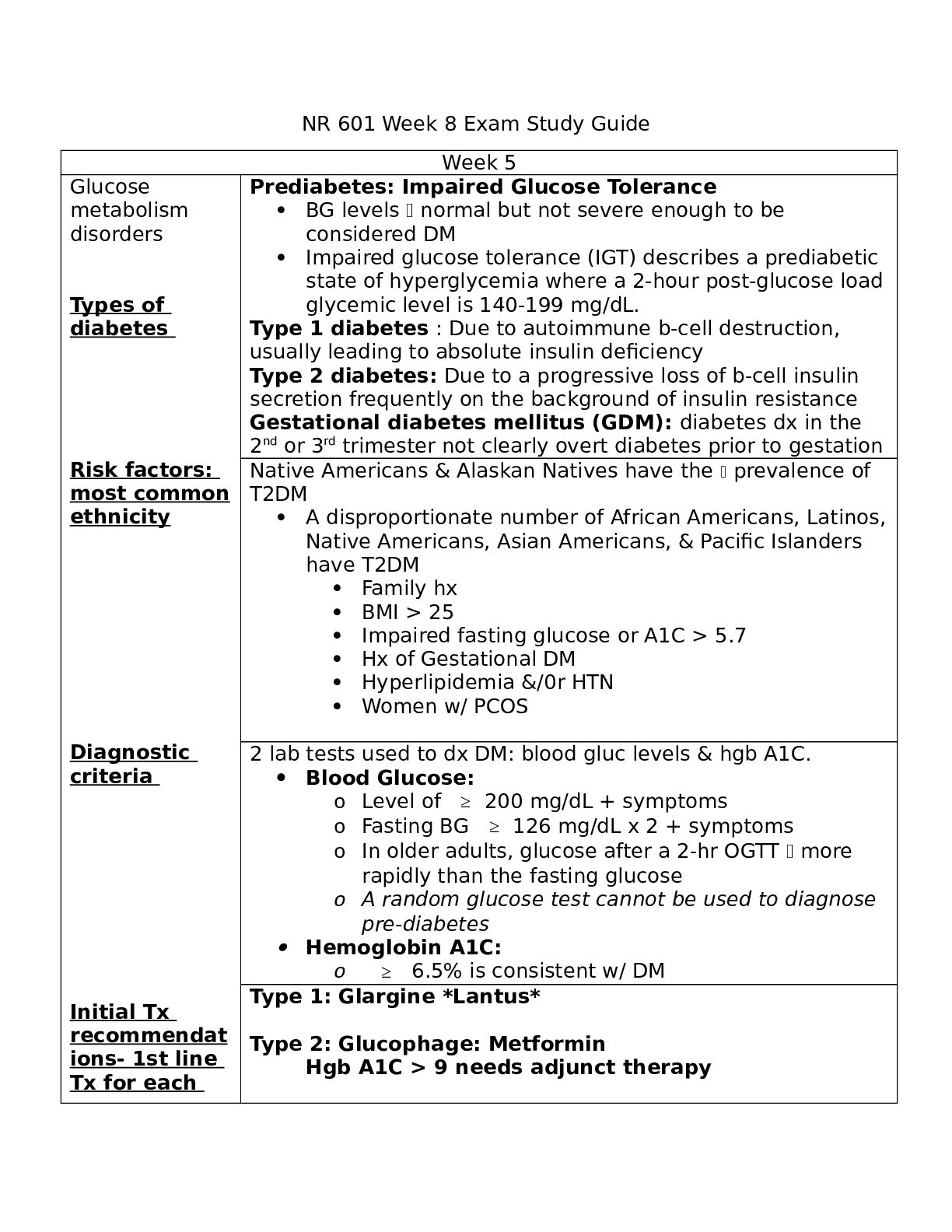
Glucose metabolism disorders
Types of diabetes (prediabetes, type 1 and type 2)
Islet cell-specific antibodies may be identified in 70-80% of people with prediabetes & those newly dx with DM1 and
hyperglycemia ty
...
[Show More]
Last updated: 3 years ago
Preview 1 out of 5 pages
Instant download
Buy this Document to get the Full Access Instantly
Provided by Students Who Aced it
We Verify Document Content to Gurantee Accuracy
Reviews( 0 )
Document information
Connected school, study & course
About the document
Uploaded On
Sep 03, 2021
Number of pages
5
Written in
All

Additional information
This document has been written for:
Uploaded
Sep 03, 2021
Downloads
0
Views
80
Document Keyword Tags
Recommended For You
Get more on EXAM »
$12.5
36 Pages
NR 601 Midterm Exam - Chamberlain College of Nursing Questi...
 GRADE A SOLUTION.png)
$14.5
22 Pages
NR 601 MIDTERM EXAM 1 QUESTIONS WITH (LATEST) GRADE A+ SOLUTIO...

$10
57 Pages
NR 601 Week 3 Psychiatric Disorders and Screening Discussion
![Preview of eBook [PDF] Barash, Cullen, and Stoelting's Clinical Anesthesia 9th Edition By Bruce F. Cu](https://browseimages.nyc3.digitaloceanspaces.com/paper-images/2024/Aug/29/8DF2QRTq2024-08-29-10-3966d0259b7c4b5.png)
$26
345 Pages
eBook [PDF] Barash, Cullen, and Stoelting's Clinical Anesthesi...
![Preview of eBook [PDF] Fundamentals of Nursing 3rd Edition By Joanne Tollefson, Sue C. DeLaune, Patri](https://browseimages.nyc3.digitaloceanspaces.com/paper-images/2024/Aug/26/U6SQ8mmq2024-08-26-01-4766cc5d40d7385.png)
$29
551 Pages
eBook [PDF] Fundamentals of Nursing 3rd Edition By Joanne Toll...
![Preview of eBook [PDF] Burns' Pediatric Primary Care 7th Edition BY Dawn Lee Garzon Maaks,, Nancy Bar](https://browseimages.nyc3.digitaloceanspaces.com/paper-images/2024/Aug/26/WR2rowXX2024-08-26-02-0966cc625bea839.png)
$29
1067 Pages
eBook [PDF] Burns' Pediatric Primary Care 7th Edition BY Dawn...

$16
137 Pages
Test Bank for Burns' Pediatric Primary Care 7th Edition by Daw...
$15
135 Pages
Burns Pediatric Primary Care 7th Edition All Chapters Complete...
More related documents below



.png)