*NURSING > QUESTIONS & ANSWERS > Remediation Fundamentals Proctored Exam With Latest Solutions UPDATED (All)
Remediation Fundamentals Proctored Exam With Latest Solutions UPDATED
Document Content and Description Below
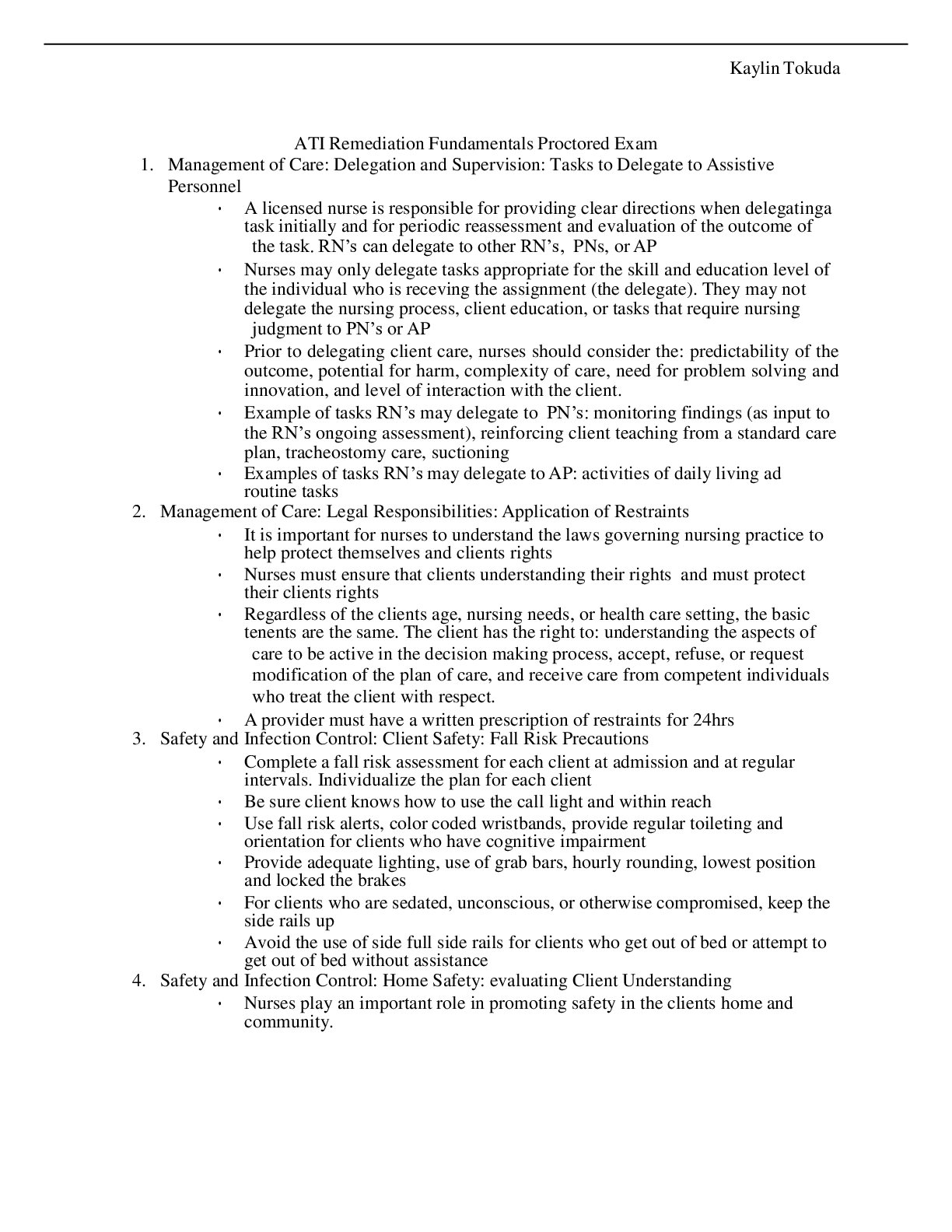
1. Management of Care: Delegation and Supervision: Tasks to Delegate to Assistive Personnel • A licensed nurse is responsible for providing clear directions when delegating a task initially and for ... periodic reassessment and evaluation of the outcome of the task. RN’s can delegate to other RN’s, PNs, or AP • Nurses may only delegate tasks appropriate for the skill and education level of the individual who is receving the assignment (the delegate). They may not delegate the nursing process, client education, or tasks that require nursing judgment to PN’s or AP • Prior to delegating client care, nurses should consider the: predictability of the outcome, potential for harm, complexity of care, need for problem solving and innovation, and level of interaction with the client. • Example of tasks RN’s may delegate to PN’s: monitoring findings (as input to the RN’s ongoing assessment), reinforcing client teaching from a standard care plan, tracheostomy care, suctioning • Examples of tasks RN’s may delegate to AP: activities of daily living ad routine tasks 2. Management of Care: Legal Responsibilities: Application of Restraints • It is important for nurses to understand the laws governing nursing practice to help protect themselves and clients rights • Nurses must ensure that clients understanding their rights and must protect their clients rights • Regardless of the clients age, nursing needs, or health care setting, the basic tenents are the same. The client has the right to: understanding the aspects of care to be active in the decision making process, accept, refuse, or request modification of the plan of care, and receive care from competent individuals who treat the client with respect. • A provider must have a written prescription of restraints for 24hrs 3. Safety and Infection Control: Client Safety: Fall Risk Precautions • Complete a fall risk assessment for each client at admission and at regular intervals. Individualize the plan for each client • Be sure client knows how to use the call light and within reach • Use fall risk alerts, color coded wristbands, provide regular toileting and orientation for clients who have cognitive impairment • Provide adequate lighting, use of grab bars, hourly rounding, lowest position and locked the brakes • For clients who are sedated, unconscious, or otherwise compromised, keep the side rails up • Avoid the use of side full side rails for clients who get out of bed or attempt to get out of bed without assistance 4. Safety and Infection Control: Home Safety: evaluating Client Understanding • Nurses play an important role in promoting safety in the clients home and community. • To initiate a plan of care, the nurse must identify risk factors using a risk assessment tool and complete a nursing history, physical examination, and home hazard appraisal • Nurses must look at risk factors for client injury such as age and developmental status, mobility and balance, knowledge about safety hazards, communication skills • For example: remove items that can cause clients to trip, place electrical cords or extension cords against the wall behind furniture, monitor gait and balance, grab bars, lighting is adequate • Keep emergency numbers near phone, have family exit plan for fires that is reviewed and practiced regularly. Review with cleitns on all ages that in the event of a fire the clients clothing or skin is on fire, the mnemonic “stop drop and roll” should be used to extinguish the fire 5. Home safety: teaching an older adult client about home safety: • When the client demonstrates fators that increases the risk for injury (regardless of age) a home hazard evaluation should be conducted by a nurse, PT, and OT. The client is made aware of the enviormental factors that can pose a risk to safety and suggestion modifications to be made • Remove items where the client can fall (loose rugs, throw rugs) • Ensure lighting is adequate inside and outside the home • Place a shower chair in the shower and provide a bedside commode • Nonskit mat in the shower 6. Psychosocial Integrity: Preschoolers (3-6 years) analyzing response to stressors • Physical development occurs at a more gradual rate than cognitive and psychosocial development, they evolve from the characteristically unstead wide stance and protruding abdomen of toddlers to the more graceful, posturally erect and strudy physicality of this age group • Preschoolers in continue in the good bad orientation of the toddler years but begin to understand behavior in terms of what is socially acceptable. They also take on new experiences • They may feel good about themseleves for mastering skills such as dressing and feeding. • During stress, insecurity or illness, they tend to regress to previous immature behavior or develop habits such as nose picking, bed wetting, or thumb sucking 7. Psychosocial Integrity: Grief, loss, palliative care: identifying anticipatory grief • Anticipatory loss: experienced before the loss happens • This grief implies the “letting go” of an object or person before the loss, as in a terminal illness • Individuals have the opportunity to start the grieving process before the actual loss • Identity expected grieving behaviors, such as crying somatic manifestations, and anxiety • Therapeutic communication related to the clients stage of grief 8. Basic Care and Comfort: fluid imbalances hyperosmolar imbalance • Fluid volume deficit- dehydration is the loss of water from the body without the loss of electrolytes. This hemoconcentration results in the increases in hct, serum electrolytes, and urine specific gravity • Compensatory mechanisms include sympathetic nervous system responses of increases thirst, ADH release, and aldosterone release • Older adults have an increased risk for dehydration • Causes of dehydration: hyperventilation, prolonged fever, DKA, and eneternal feeding without sufficient water intake 9. Basic care and comfort: nasogastric intubation and enteral feedings: unexpected findings • Nasogastric intubation is the insertion of NG tube to manage GI dysfunction and provide enteral nutrition via NG. • Excoriation of nares and stomach is a complication of NG tubes. Apply water soluble lubricant to the nares, assess the color of the drainage, report dark coffe ground or blood immediately, and consider switching the tube to other naris • Discomfort is another complication. Rinse the mouth with water for dryness, throat lozenages can help and provide oral care • Occulusion of the NG tube leading to distention is another complication. Irrigate the tube to unclog blockages. Use tap water with enteral feedings, have the client change positions in case the tip of the tube is against the stomach wall • Complications of enteral feedings: gastric residual exceeds 250 mL for each of two consecutive assessments. Withhold the feeding and notify HCP, keep client in semi folwers, recheck residual in 1hr 10. Basic care and comfort: personal hygiene: grief loss, and palliative care: providing postmortem care • Nurses are responsible for following federal and state laws regarding requests for organ and tissue donation obtaining permission for autopsy • After postmortem care is completed, the clients family becomes the nurses primary focus • Ask the family whether they would like to visit with the body, honoring any decisions • Provide care with respect and compassion while attending to the desires of the clients and family per their culture, religion, and social practices • Clarify where the clients personal belongings should go: with the body or to a designated person • Prepare the body for viewing (privacy, remove all tubes and personal belongings, cleanses and align the body supine with a pillow under the head, arms with palms of hands down outside the sheet and blanket, dentures in place, and eyes closed, apply fresh linens, remove excess supplies, dim the lights and minimize noise 11. Reduction of Risk potential: intravenous therapy: recognizing phlebitis • Edema; throbbing, burning, or pain at the site; increased skin temp, eryhtemia, red line up the arm with a palpable band at the vein site, slowed rate of infusion • Treat promptly discontinue the infusion and remove the catheter • Elevate the extremity, apply warm compress three to four times/day. Restart the infusion in a different vejn proximal to the site • How to prevent: rotate sites at least every 72 hrs or sooner, avoid the lower extremities, hand hygiene, and [Show More]
Last updated: 3 years ago
Preview 1 out of 4 pages
Buy this document to get the full access instantly
Instant Download Access after purchase
Buy NowInstant download
We Accept:

Reviews( 0 )
$10.00
Can't find what you want? Try our AI powered Search
Document information
Connected school, study & course
About the document
Uploaded On
Nov 13, 2021
Number of pages
4
Written in
All

Additional information
This document has been written for:
Uploaded
Nov 13, 2021
Downloads
0
Views
160






.png)