NUR 265 Nursing Concepts Test # 3/Adv Med Srg #3 STUDY GUIDE
Document Content and Description Below
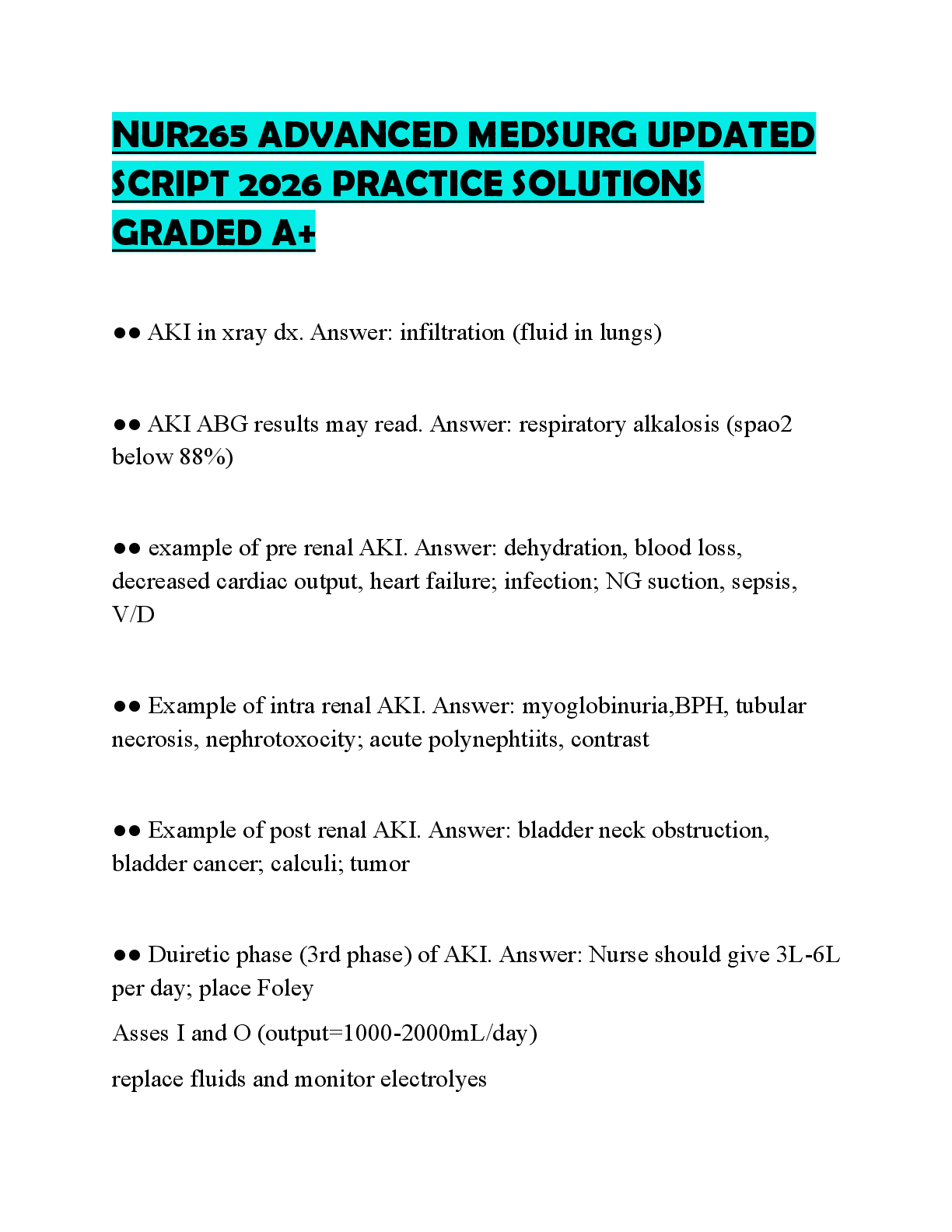
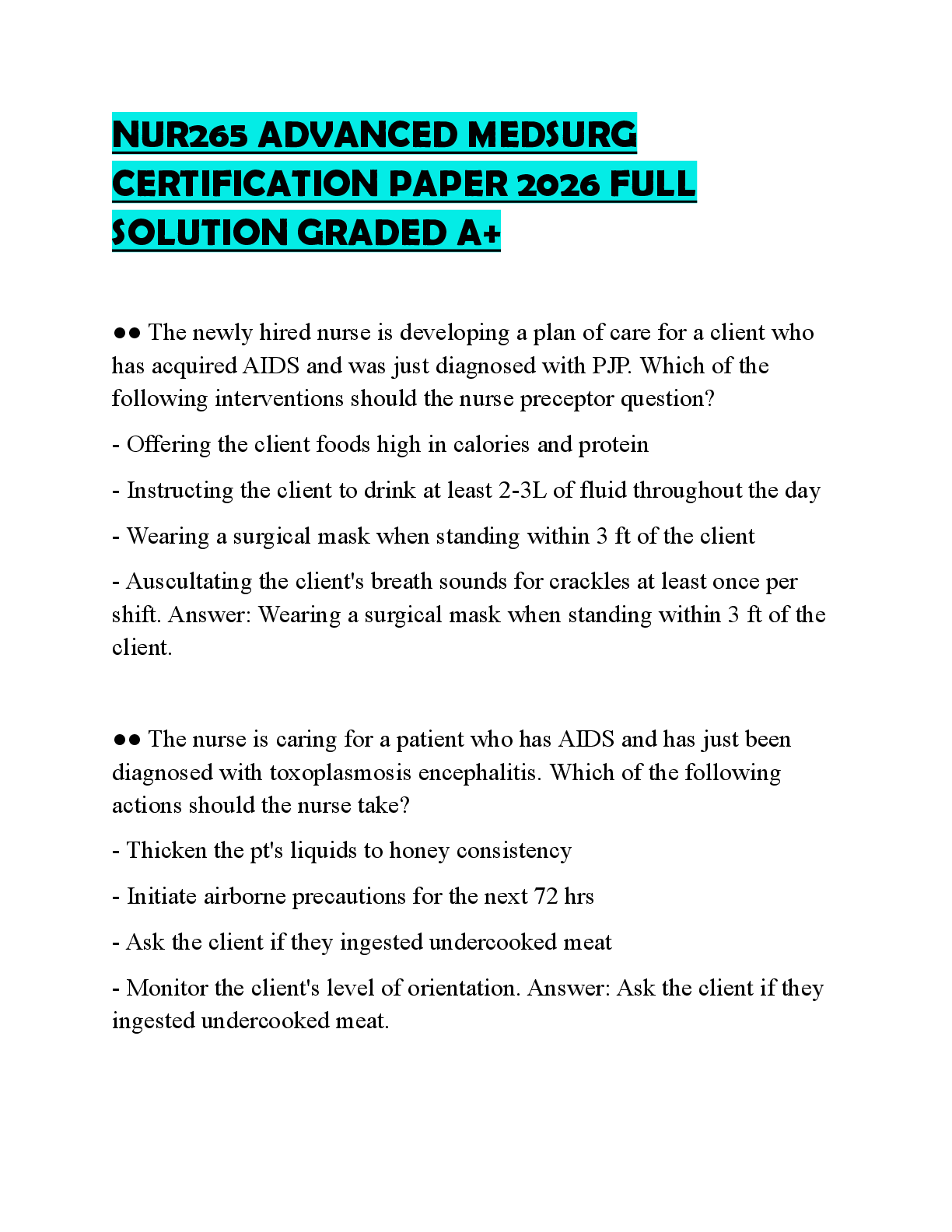
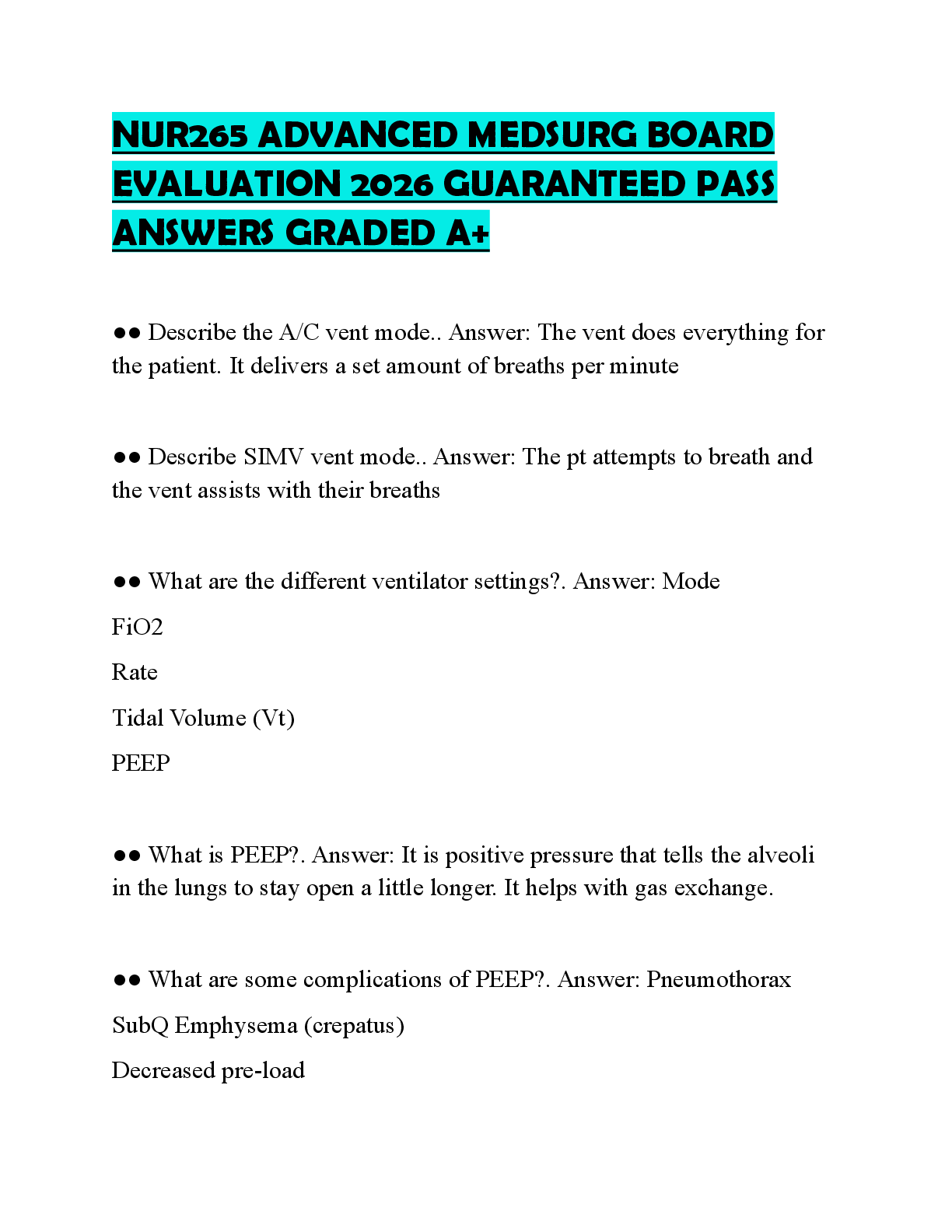
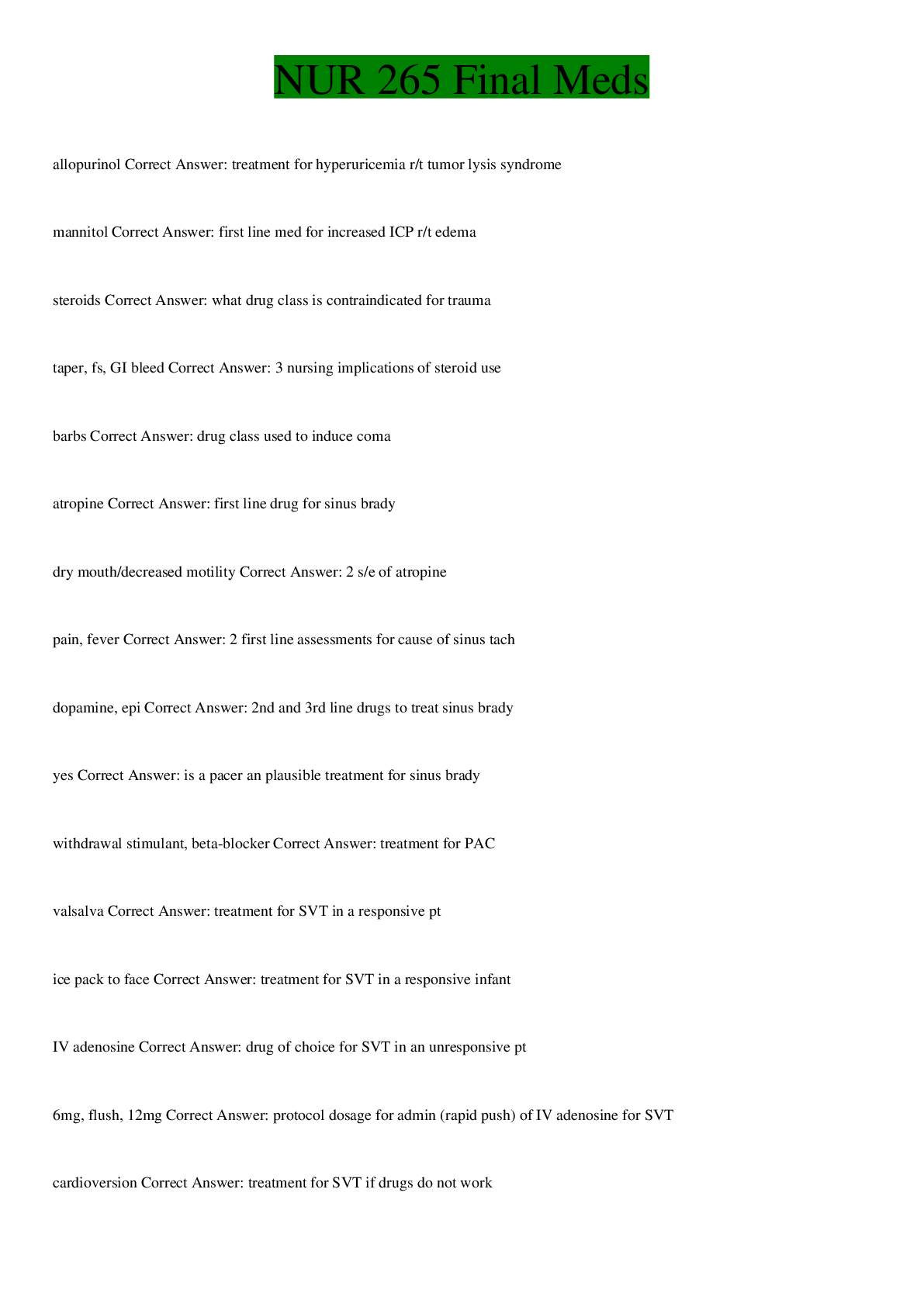
NUR 265 Nursing Concepts Test # 3 Care of Critically Ill Patients with Neurologic Problems / Chapter 47 (25 questions) Traumatic Brain Injury 1. Contrecoup injury Coup is an impact to the frontal lobe; countrecoup is t
...
[Show More]
Last updated: 3 years ago
Preview 1 out of 9 pages
Instant download
 (2).png)
Buy this Document to get the Full Access Instantly
Provided by Students Who Aced it
We Verify Document Content to Gurantee Accuracy
Reviews( 0 )
Document information
Connected school, study & course
About the document
Uploaded On
Jan 21, 2022
Number of pages
9
Written in
All

Additional information
This document has been written for:
Uploaded
Jan 21, 2022
Downloads
0
Views
99
Document Keyword Tags
Recommended For You
Get more on EXAM »

$15.5
43 Pages
Nur 265 Exam 1 Actual Questions And Answers || Latest Version...
$12.5
25 Pages
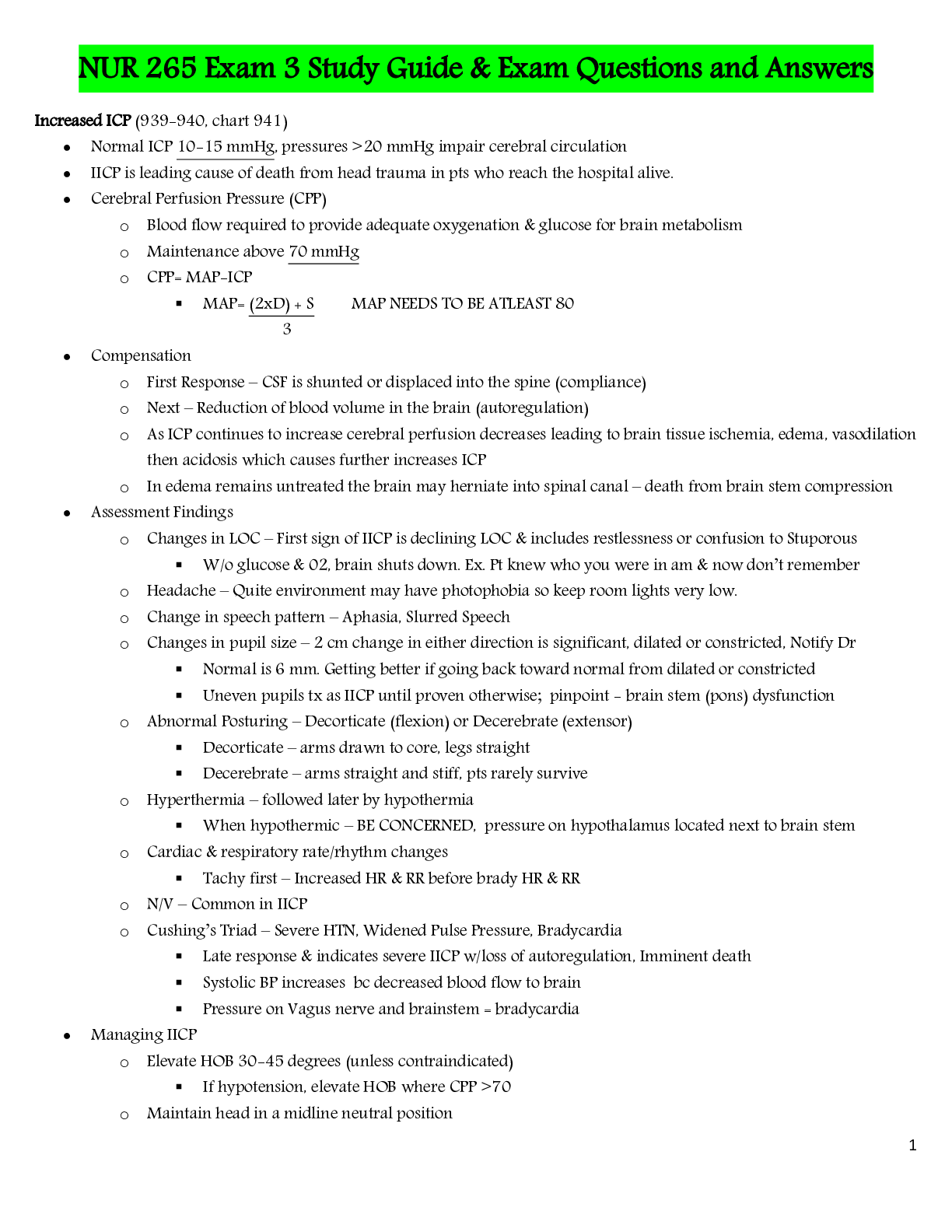
NUR 265 Exam 3 Study Guide & Exam Questions and Answers
$12
11 Pages
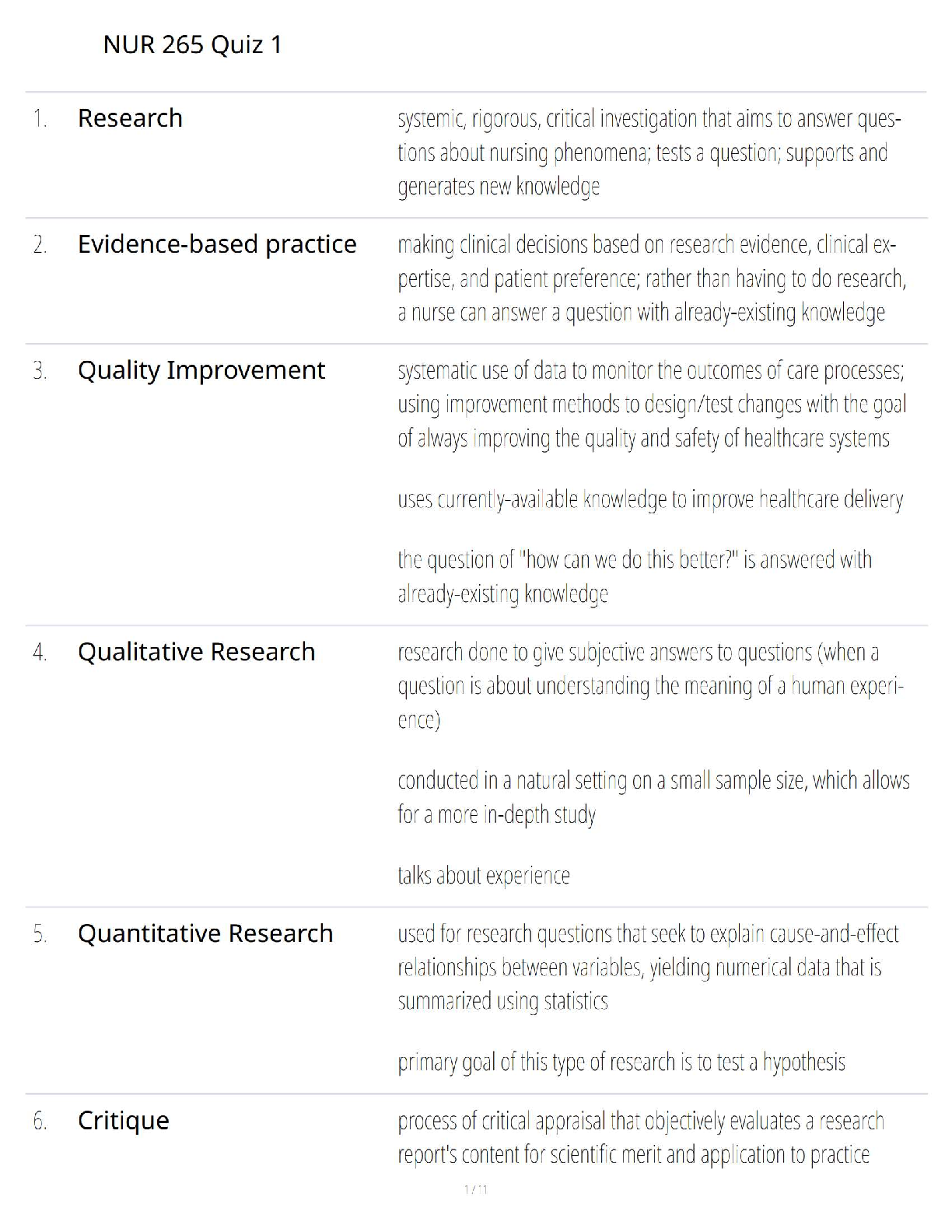
NUR 265 Quiz 1 Study Guide: Score 100% with Correct Answers –...

$12
16 Pages
NUR 265 Exam 2 Study Guide-with 100% verified questions and a...
More related documents below