NURS 6560 Final Exam Study Guide (Complete Guide for Exam Preparation)
Document Content and Description Below
NURS 6560 Final Exam Study Guide (Complete Guide for Exam Preparation)
NURS 6560 Final Exam Study Guide Liver Biliary Tract, Pancreas, Spleen Resection of the liver and regeneration and follow up labs pp 546-548 Types
...
[Show More]
Last updated: 3 years ago
Preview 1 out of 53 pages
Instant download


Buy this Document to get the Full Access Instantly
Provided by Students Who Aced it
We Verify Document Content to Gurantee Accuracy
Reviews( 0 )
Document information
Connected school, study & course
About the document
Uploaded On
Dec 06, 2020
Number of pages
53
Written in
All

Additional information
This document has been written for:
Uploaded
Dec 06, 2020
Downloads
0
Views
97
Document Keyword Tags
Recommended For You
Get more on EXAM »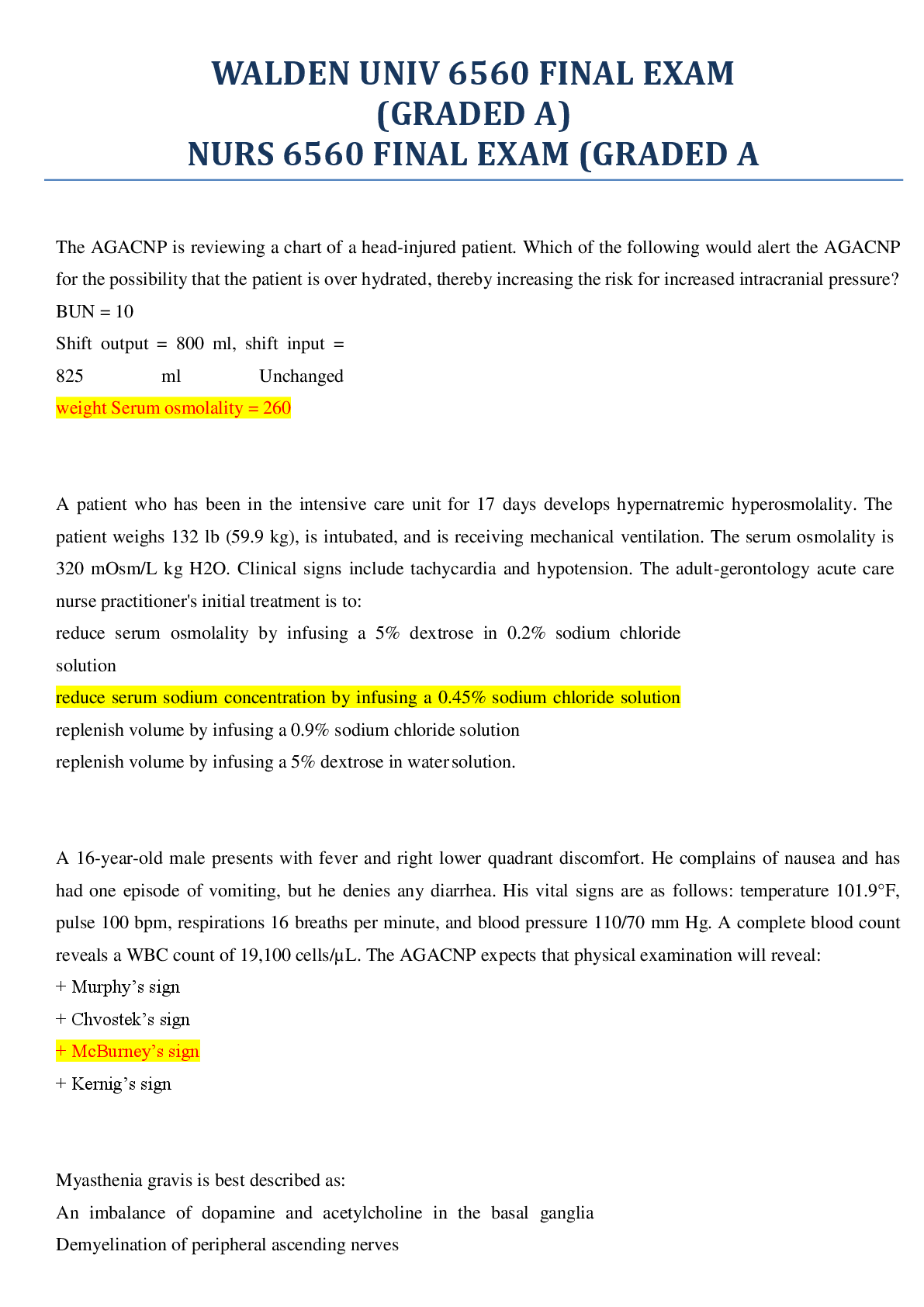
$15
27 Pages
NURS 6560 Advanced Practice Care of Adults in Acute Care Setti...
$9
26 Pages
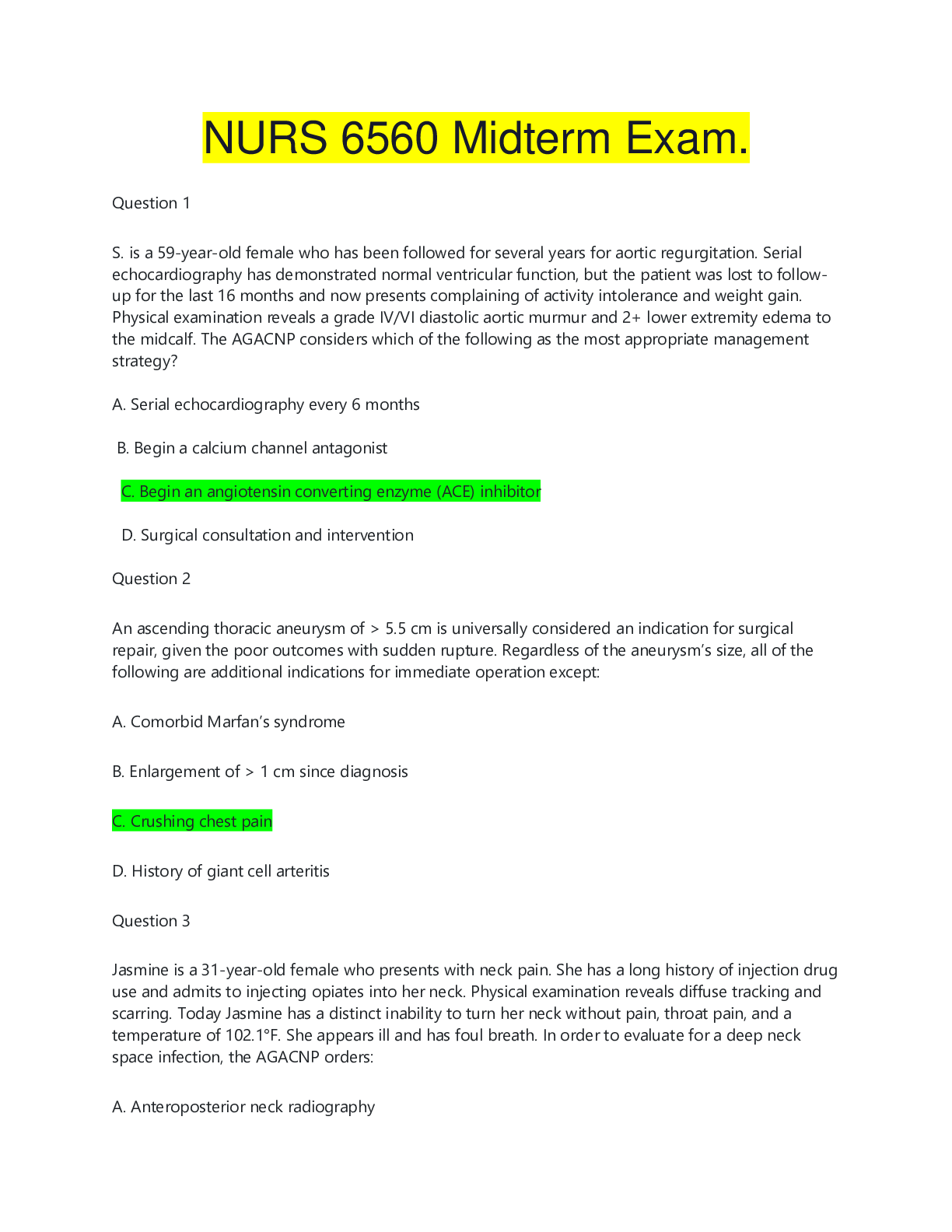
NURS 6560 Midtem Exam. 100 Questions and Answers | NURS 6560...

$12
7 Pages
NURS6560 / NURS 6560: Advanced Practice Care of Adults in Acut...

$14.5
17 Pages
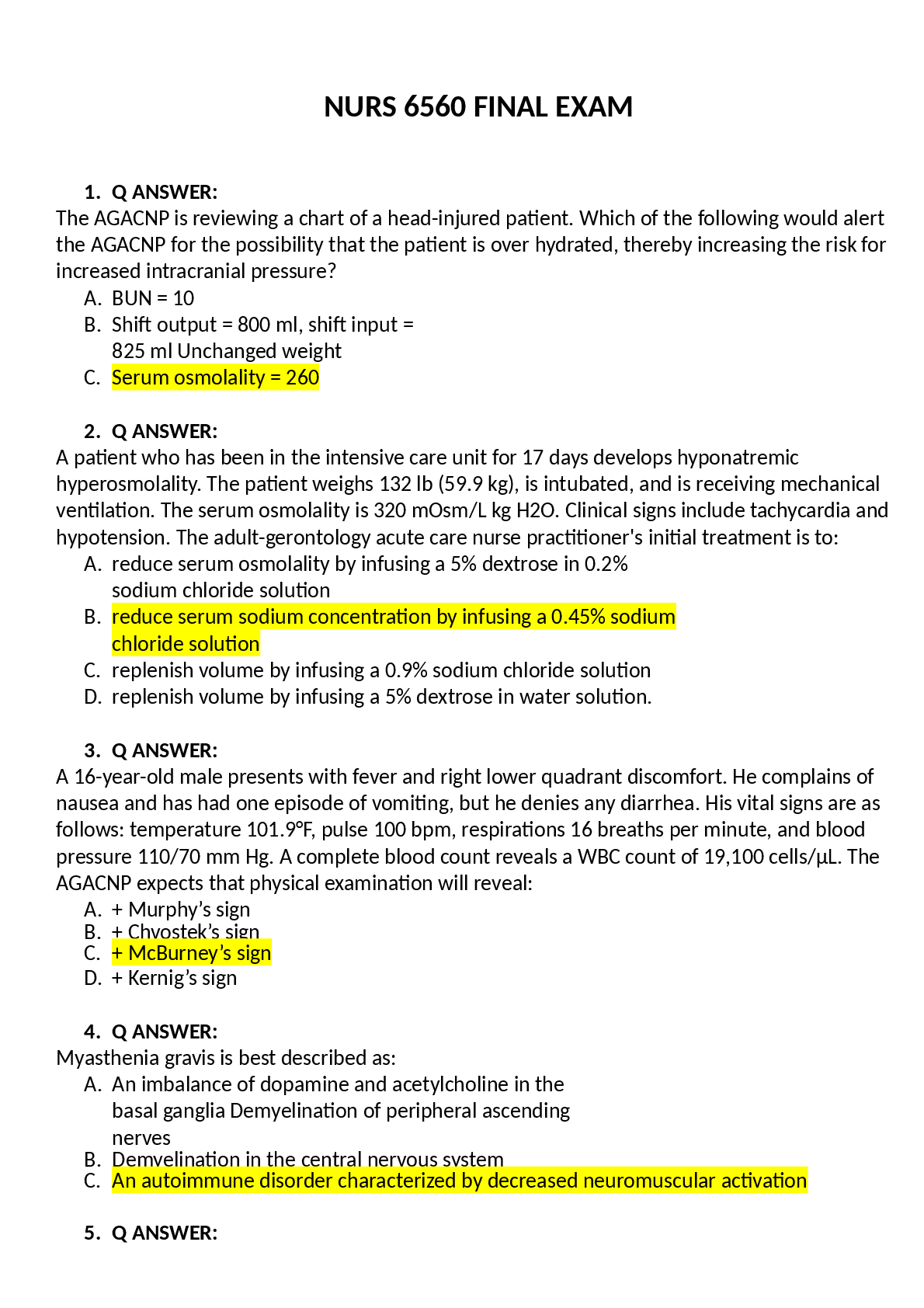
NURS 6560 FINAL EXAM, Latest (2022/2023) complete Questions &...
$19
24 Pages
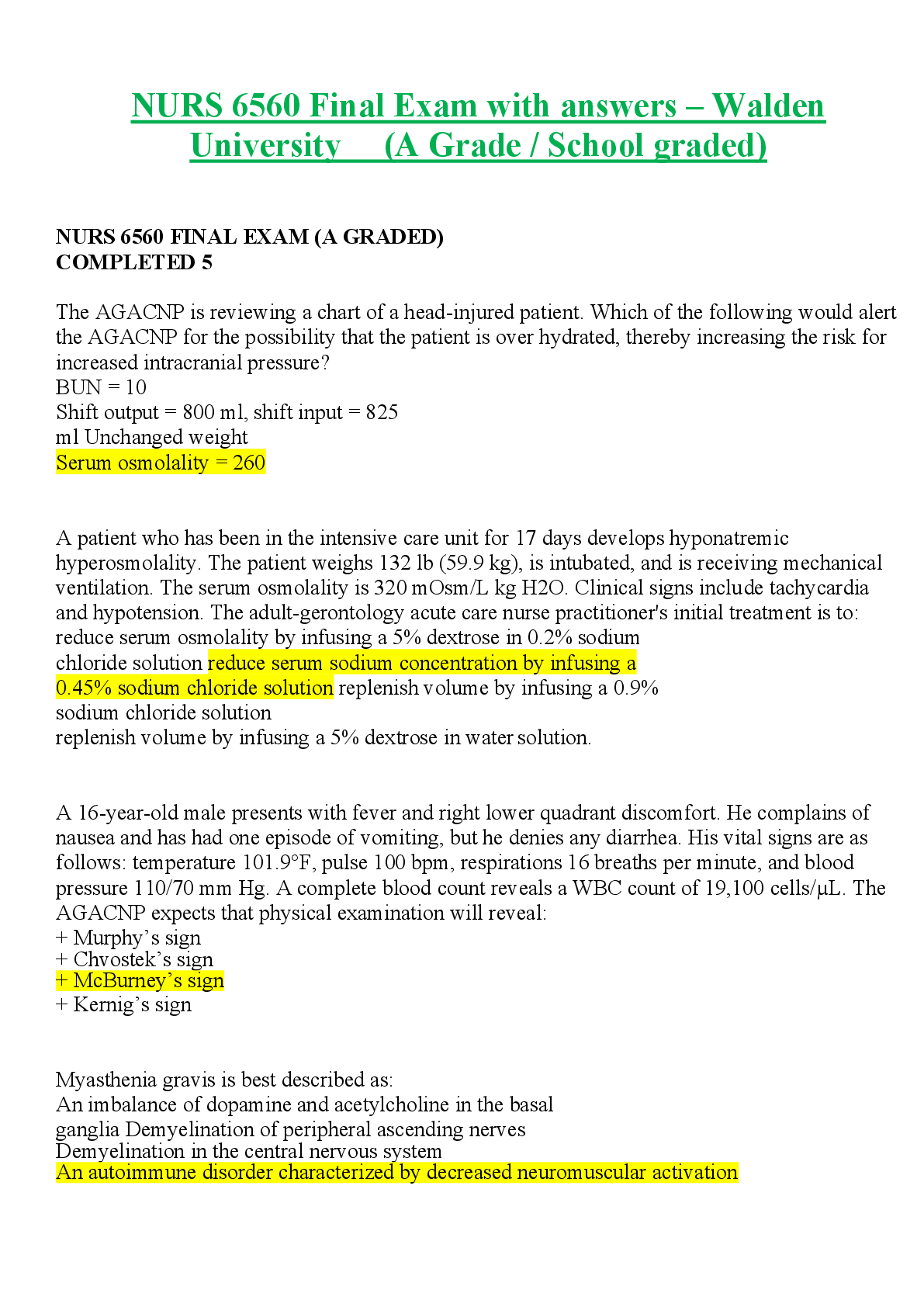
NURS 6560 Final Exam with answers – Walden University (A Grad...
 MY21.png)
$6.5
6 Pages
NURS6560 / NURS 6560 Final Exam Study Guide (Updated) : Advan...
$25
17 Pages
NURS 6560 Exit Exam (Test Bank solution) | NURS6560 exit exam...

$15
17 Pages
TEST BANK NURS 6560 Exit Exam | NURS6560 exit exam (2020/2021)
$18
136 Pages
TEST BANK; NURS 6560 Final, MIDTERM & FINAL JUNE Exam / NURS-...

$11
63 Pages
NURS6560 / NURS 6560 Midterm Exam Study Guide : Advanced Prac...

$8.5
4 Pages
NURS 6560 - Week4 iHuman; Primary Diagnosis: Acute Bacterial e...
$25
16 Pages
WEEK 8 I-HUMAN CASE FOR A 72 YEARS OLD PATIENT CC: UNUSUAL MO...

$15
278 Pages
TEST BANK for Saunders Comprehensive Review for the NCLEX-RN®...
More related documents below