Elsevier NCLEX Endocrine 2023
$ 14

TEST BANK FOR Buttaro: Primary Care: A Collaborative Practice/ Interprofessional Collaborative Practice 6TH EDITION.TOP NOTCH
$ 10

CNA Final Exam/Practice Test
$ 10

NURS C787-NUTRITION STUDY GUIDE-complete
$ 14
NCP ON DIABETES MELLITUS
$ 10

MGT3102 W1A1.docx
$ 10
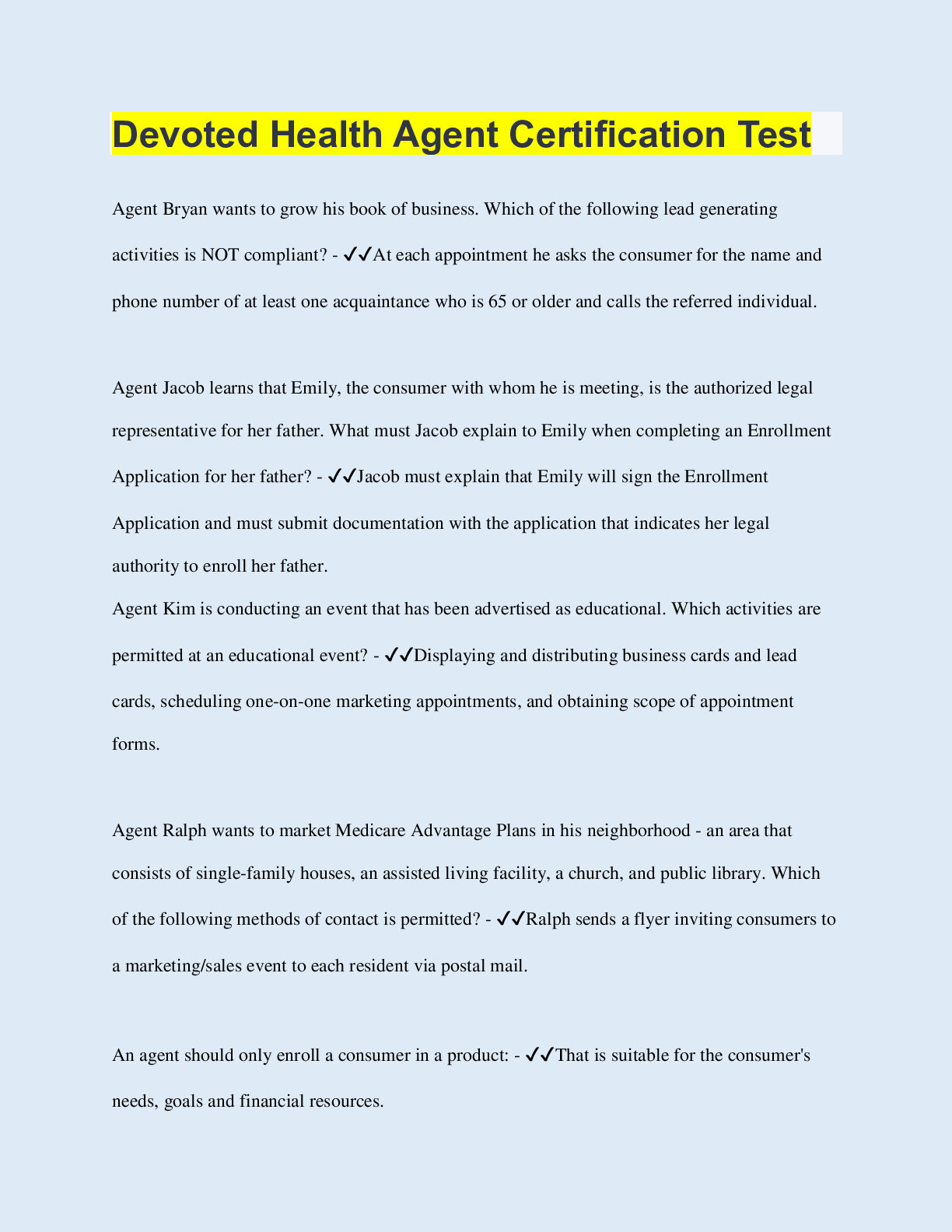
Devoted Health Agent Certification Test
$ 8.5
WK3AssgnLoveD ..docx
$ 10
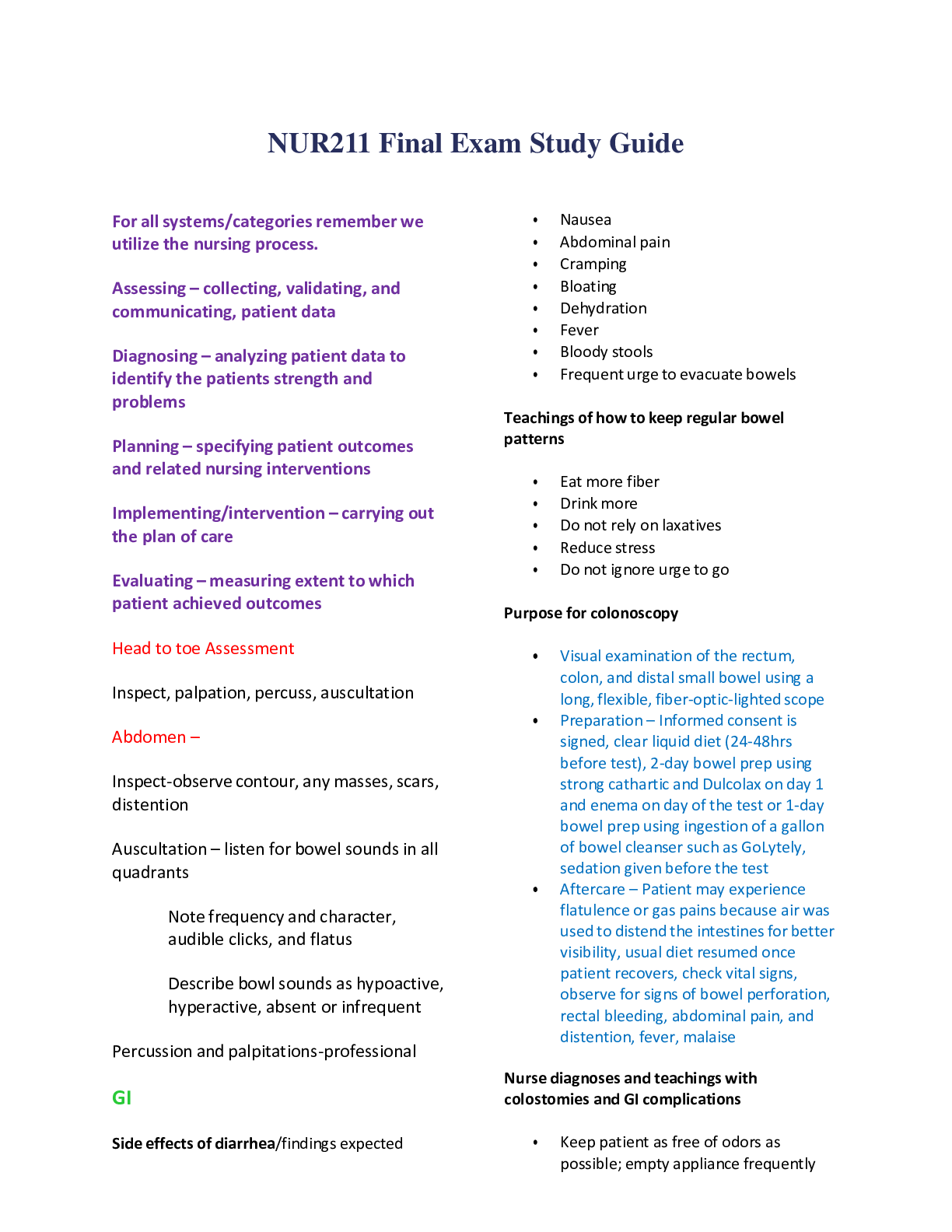
NUR211 Final Exam Study Guide
$ 10

Task 5 Math Systems.docx Task 5 Finite Mathematics Task 5: Math Systems A. Explain why
$ 10

WK2AssigPUBH4030.pdf (1)
$ 10
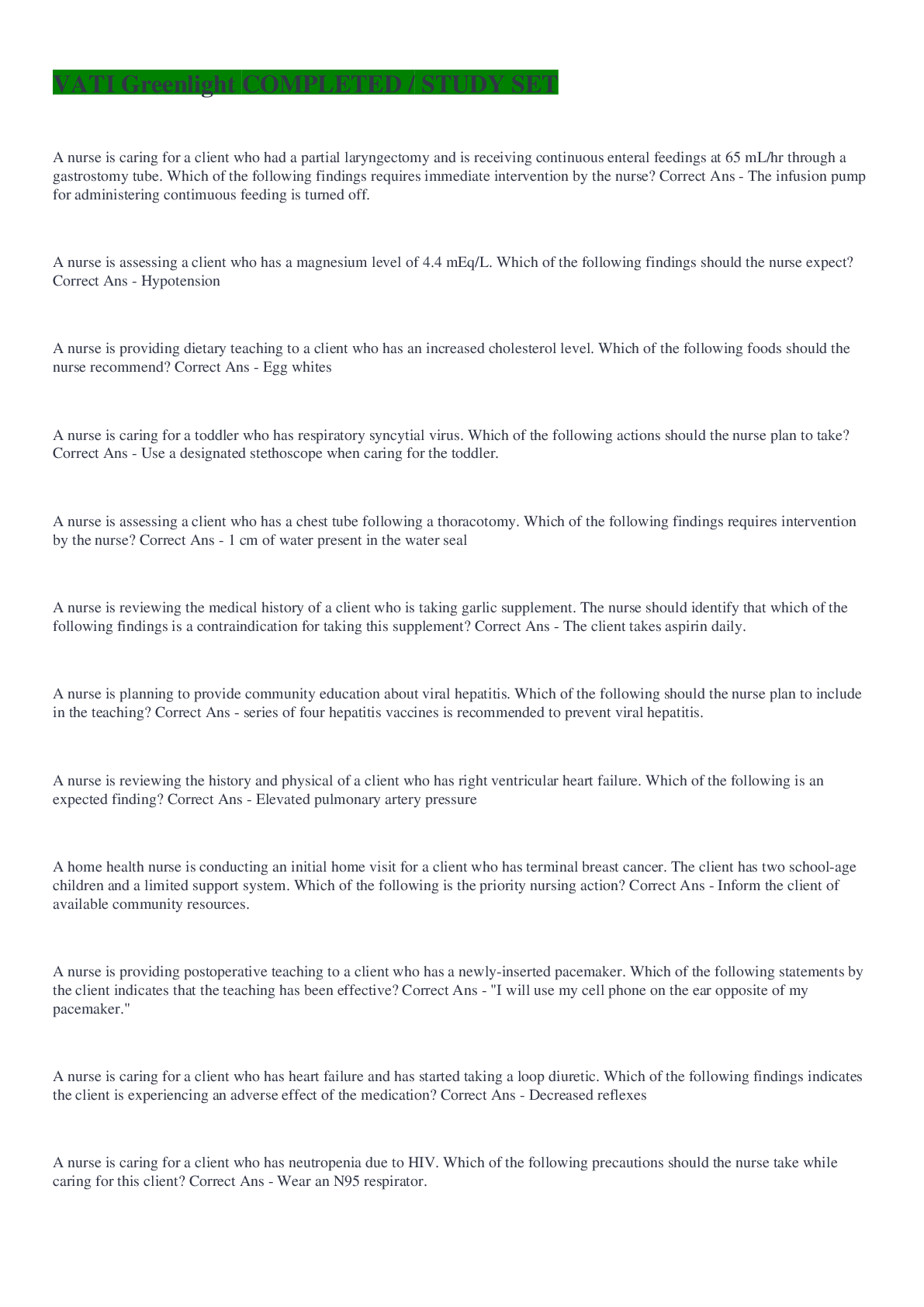
VATI Greenlight COMPLETED / STUDY SET
$ 26.5
eBook The Mekong River Basin (Volume 3) 1st Edition By Hong Quan Nguyen, Heiko Apel, Quang Bao Le, Minh Tu Nguyen, Venkataramana Sridhar
$ 30
.png)
NURS 6501N Final Exam 3
$ 7
ICT2622 SEM 2 ASSIGNMENT 2 2023
$ 19
Untamed by Glennon Doyle
$ 4.5
MedSurg Notes for Edapt
$ 30
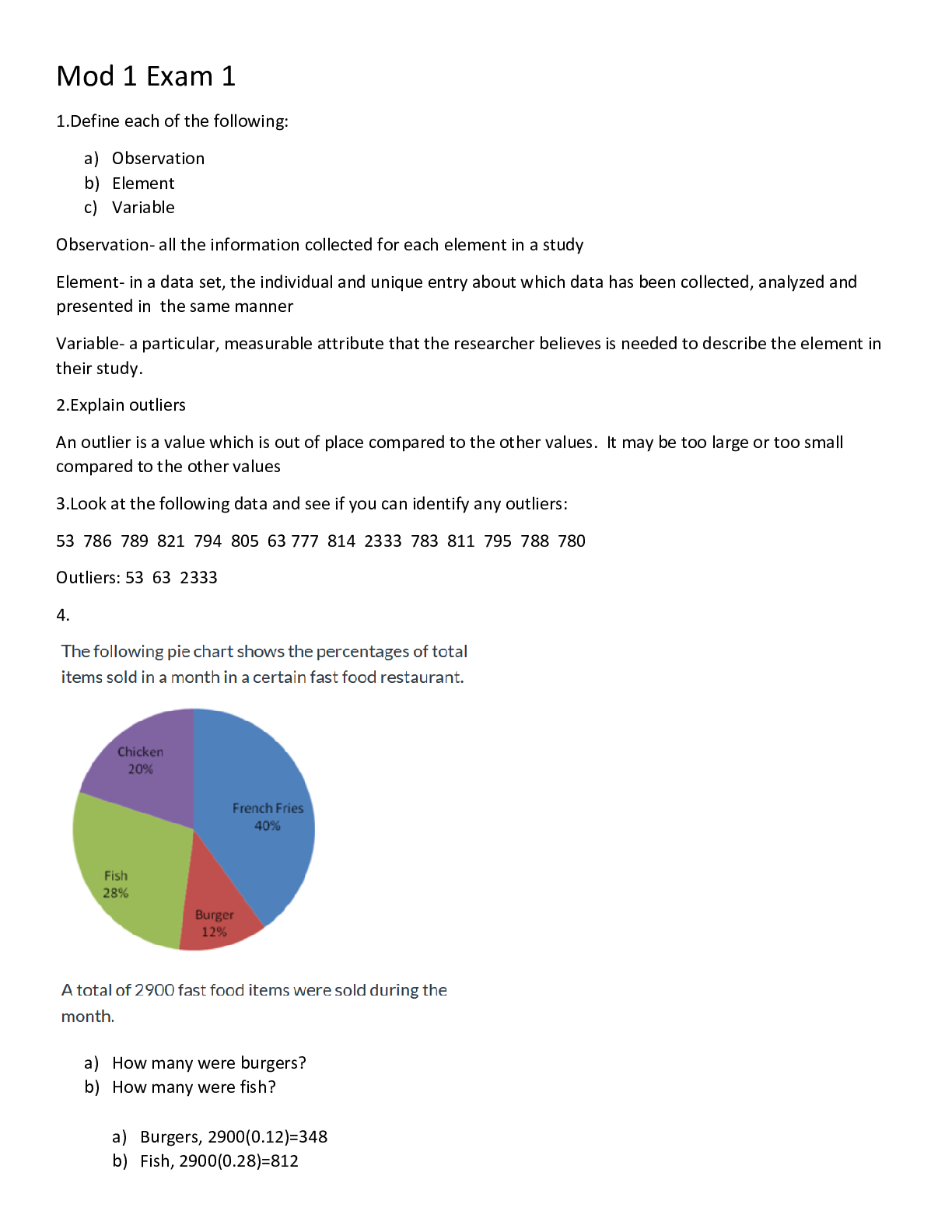
MATH 110 All Exams Pack Complete Solution 2022
$ 10

NURS 6541 MIDTERM EXAM
$ 9

Practice Exam - Version A.
$ 9
.png)
EMT Lab Practical Review 2022
$ 8
CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD
$ 13
Fall 2021 Final Exam Version A.
$ 8
ATI Questions Chapter 3 Neurologic Diagnostic Procedures
$ 11
.png)
Maths A Level Statistics Questions and Answers Rated A+
$ 9.5
BIOM2011 Cardiac function final 2019
$ 13
EPPP Practice test 1 2022
$ 13
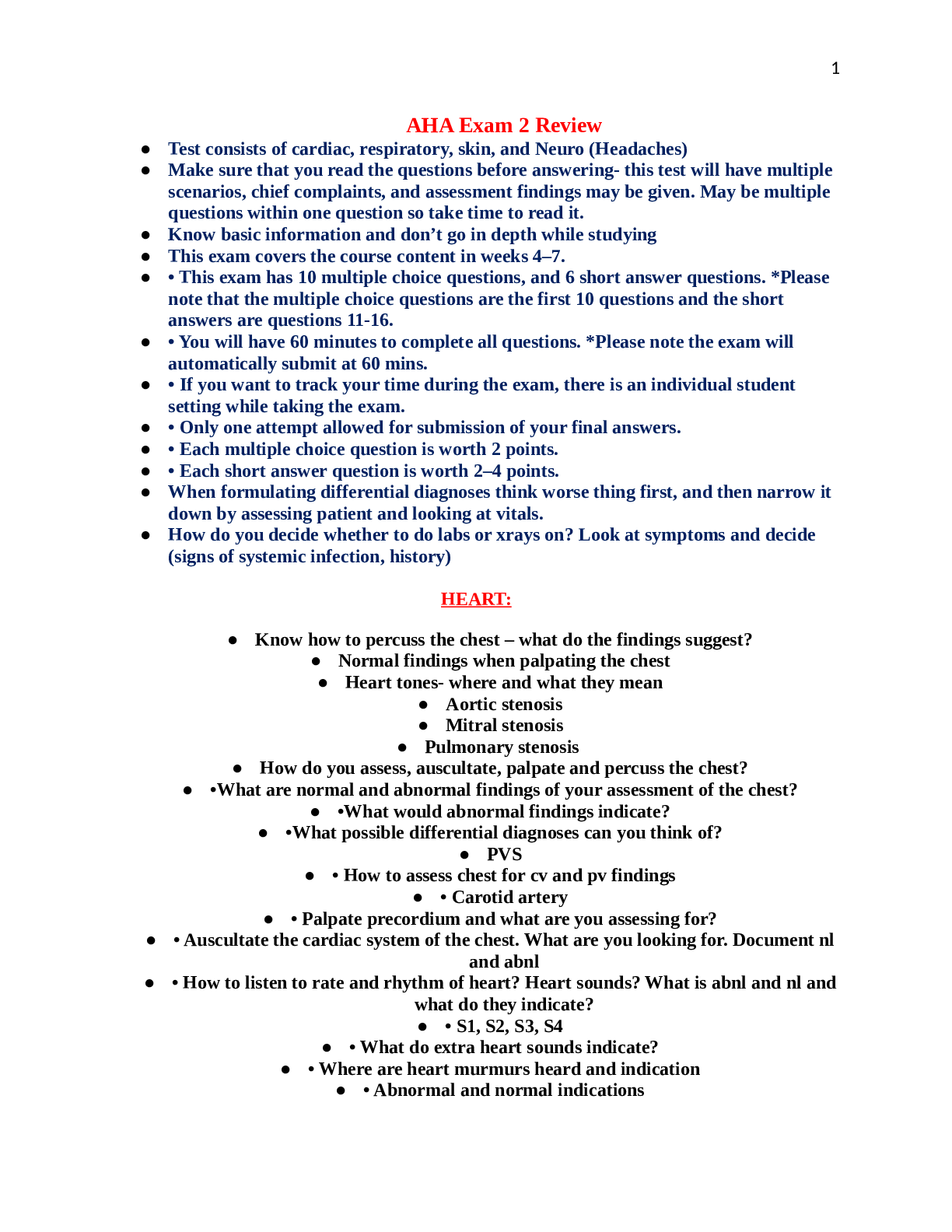
AHA Exam 2 Master Study Guide 2023
$ 11
.png)
Math_Practice_Quiz 4_Final-1.
$ 10
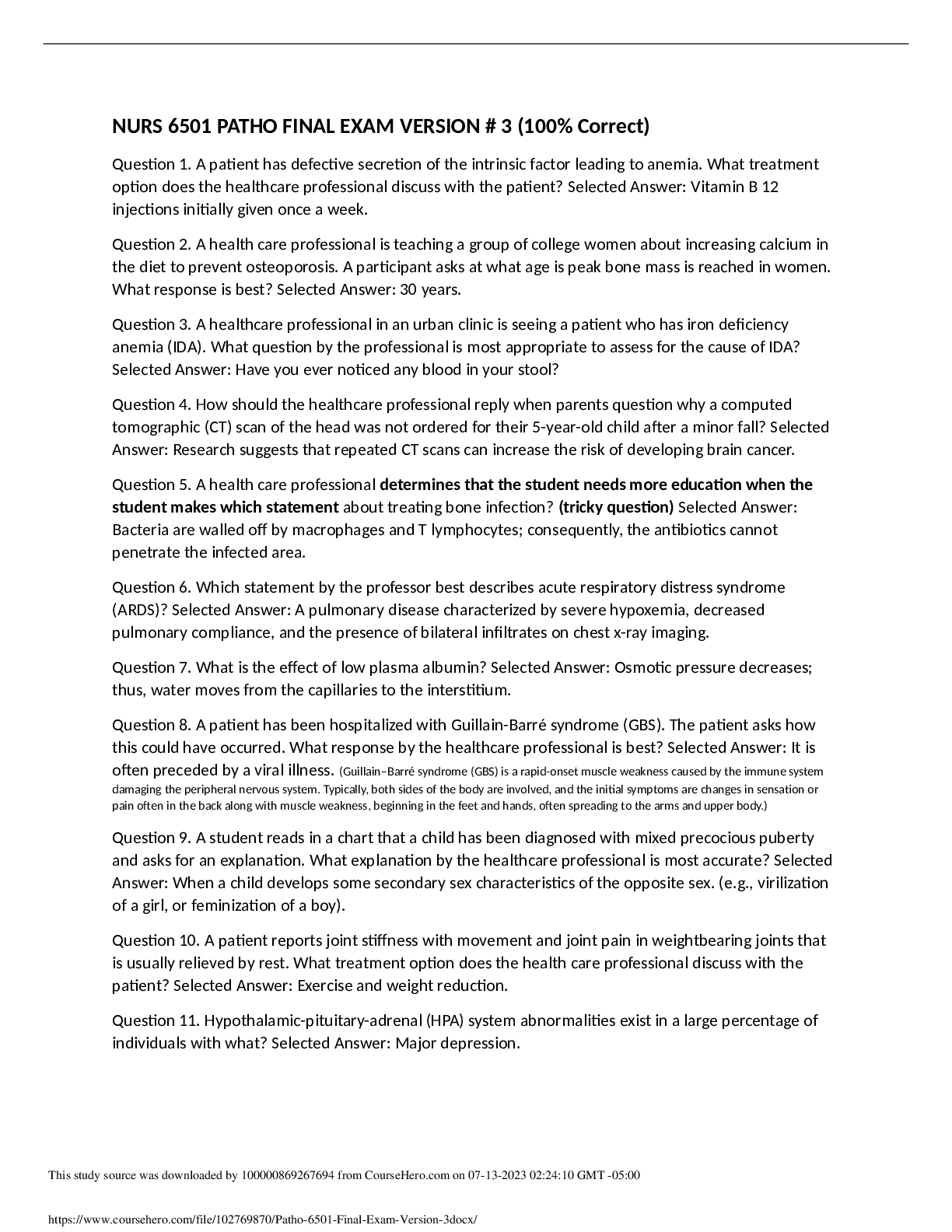
Patho 6501 Final Exam Version #3
$ 10
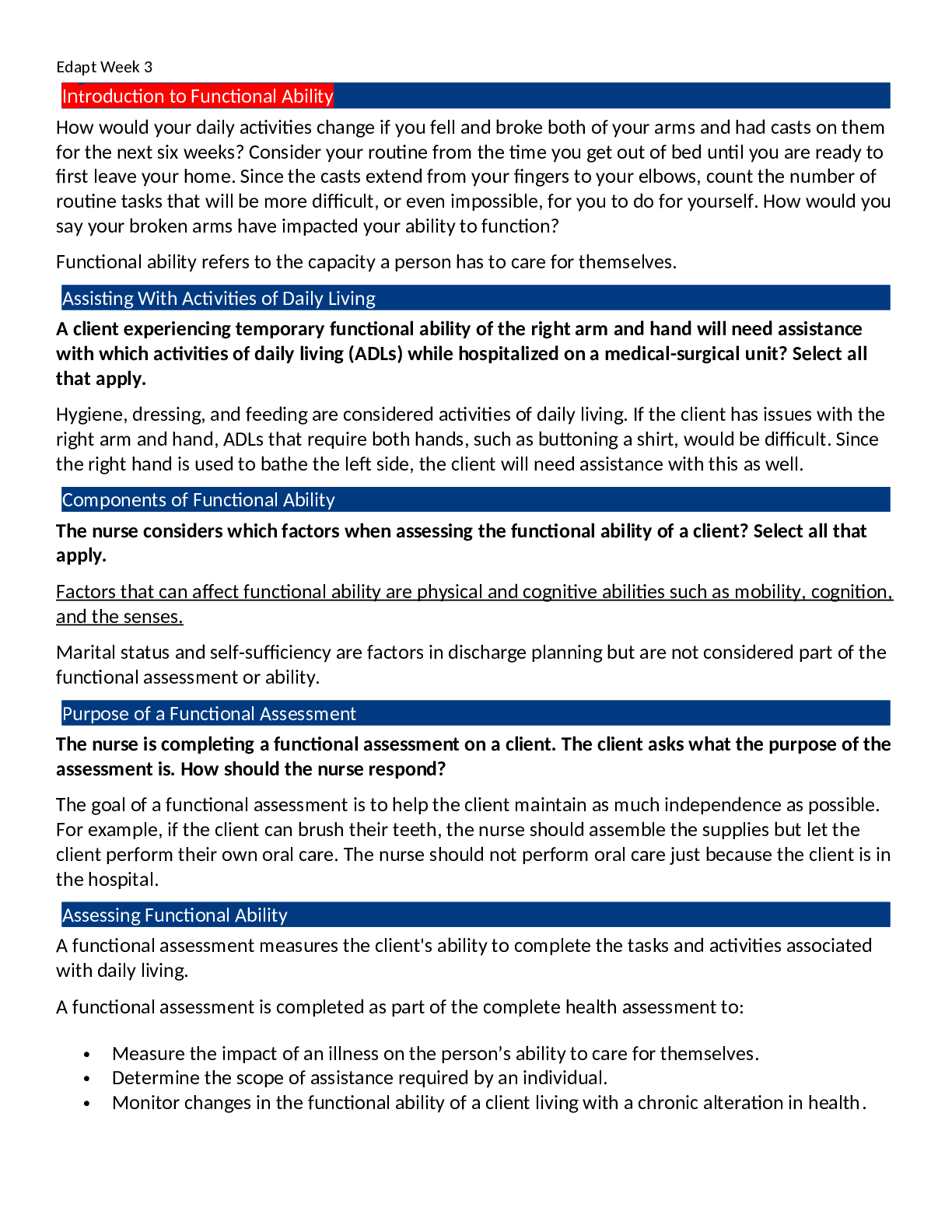
Edapt Week 3 Introduction to Functional Ability
$ 16
BUS 421 final exam 2022




.png)