CADC – Documentation
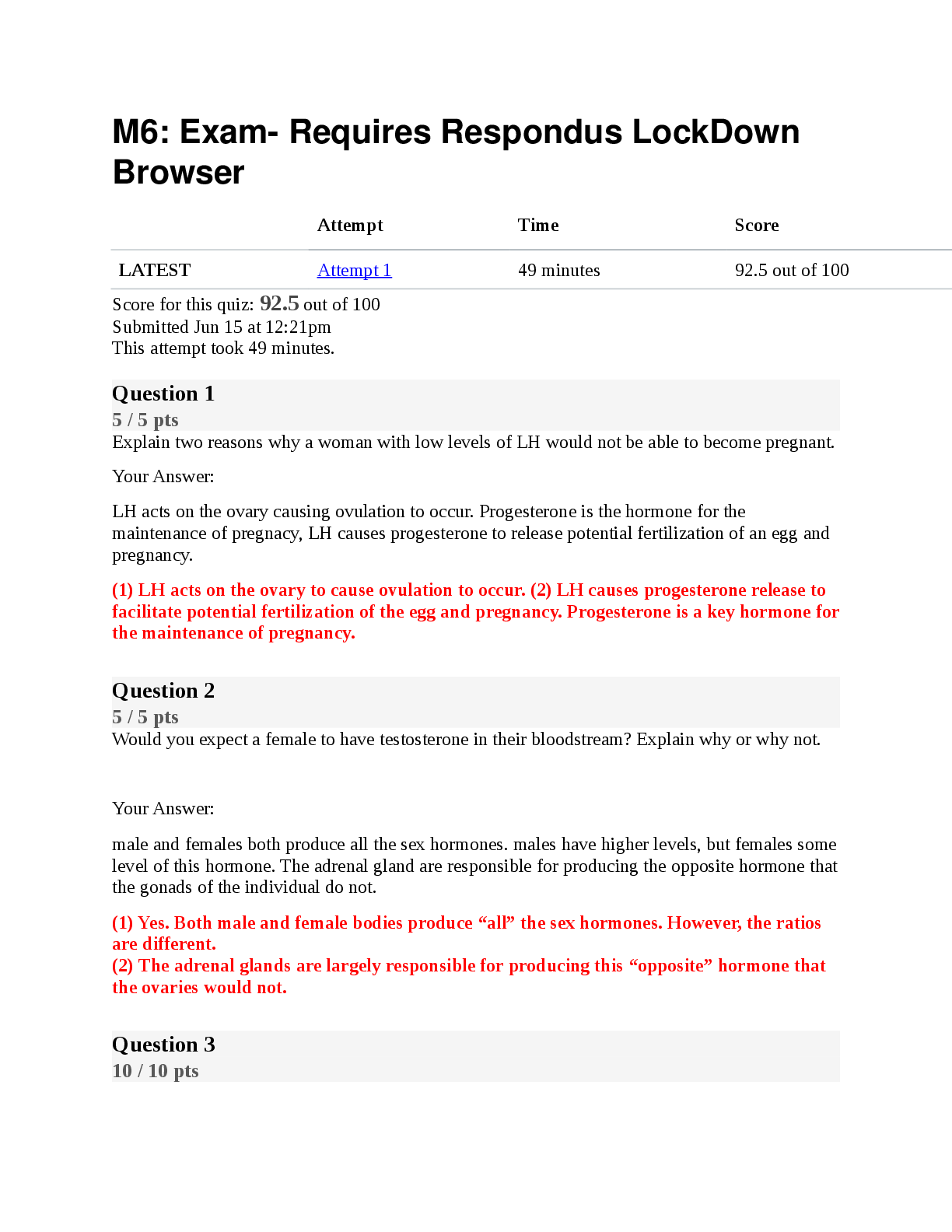
Roles of documentation ✔✔1. clinical tool
2. continuity of care
3. legal document
4. accountability
5. quality assurance
Documentation as a clinical tool ✔✔chronologically details the condition
...
CADC – Documentation
Roles of documentation ✔✔1. clinical tool
2. continuity of care
3. legal document
4. accountability
5. quality assurance
Documentation as a clinical tool ✔✔chronologically details the condition of the client receiving
services, why the services were needed, services provided who delivered the services, and
outcomes achieved.
- used in supervision
- most important skill in assuring continuity of care
Documentation as means to ensure continuity of care ✔✔ensures continuity of care, regardless of
counselor availability, changes in counselor or service provider or subsequent readmission for
services.
- EASES the TRANSITION PROCESS ensuring pertinent info is available to receiving
counselor/program
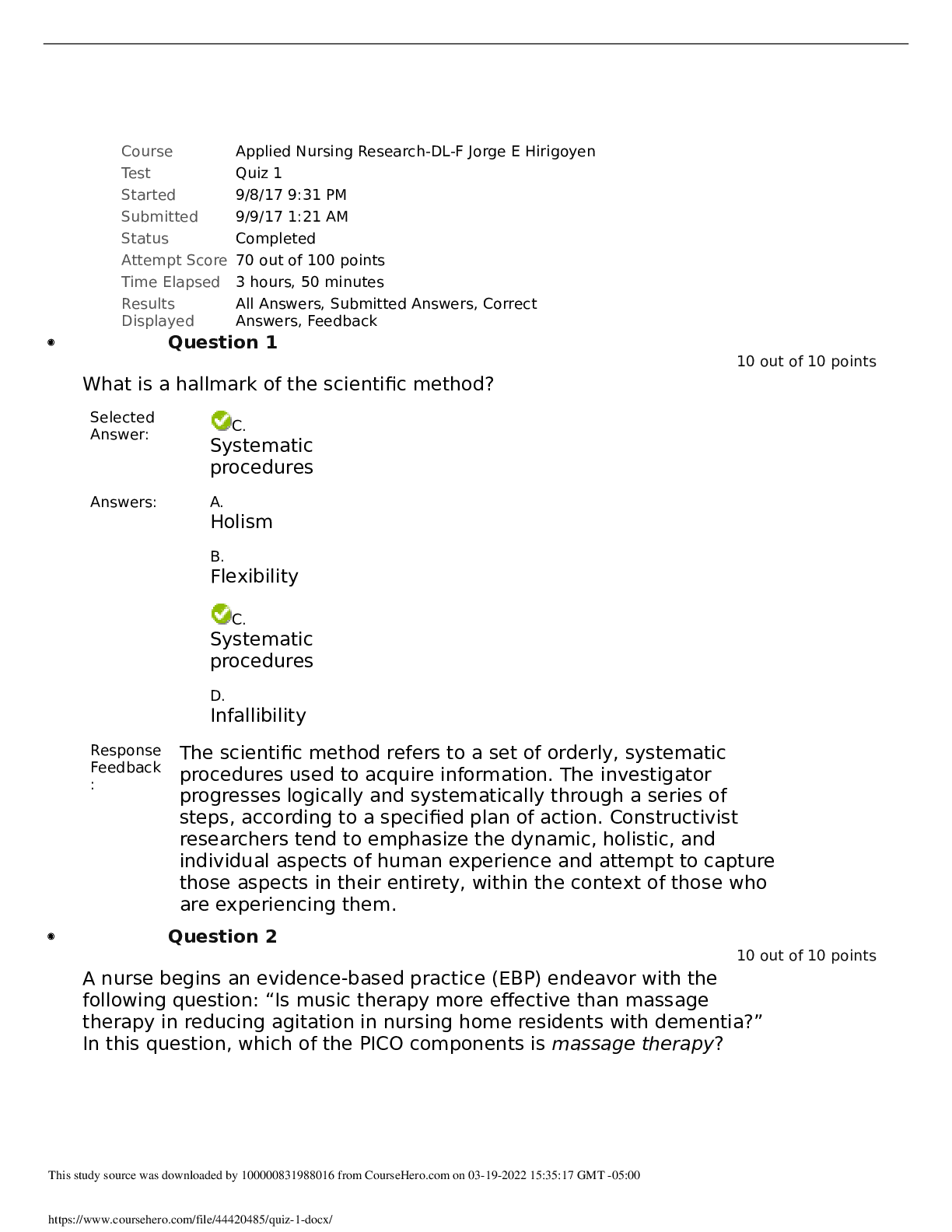
Documentation as a legal document ✔✔records both counselor and client input, including what
did/did not work.
- portions of clt record may be requested by courts if clt is legally involved or in cases where the
clt brings legal proceedings against a counselor/program
Documentation as accountability ✔✔recording information that is used for billing purposes,
financial audits or reviews to ensure compliance with various standards.
- document time, date, duration & type of insurance
Documentation for quality assurance ✔✔the clt record provides documentation for quality
assurance reviews including utilization review, peer review, and clinical supervision.
- processes assess if the type, intensity, duration of services are appropriate for client's condition
and if documents meet regulatory and agency expectations.
In IL, how long are treatment records retained? ✔✔5 years after discharge, excluding the
accounting of disclosures protected by HIPPA which must be retained for 6 years.
In IL, How long are medical records detained? ✔✔7 years
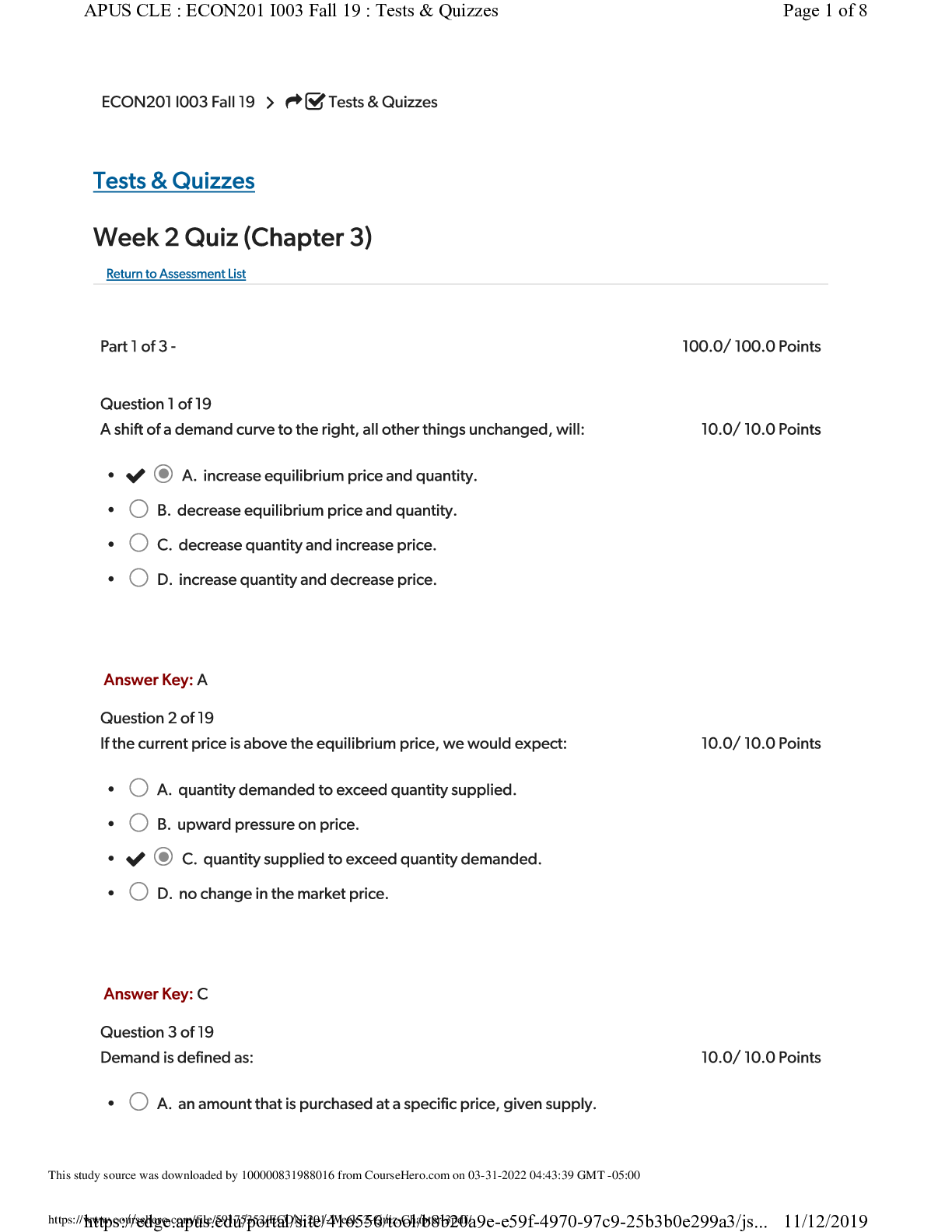
Screening ✔✔Occurs at INITIAL CONTACT, purpose is to gather enough preliminary
information about the clt to evaluate their need for services, eligibility for services, and appropriate
level of care/service placement.
- Focuses on CURRENT INFO regarding the PRESENTING PRBLM and the PRBLM ACUITY
that resulted in the clt seeking or being referred to treatment
Elements of screening documentation ✔✔1. Referral source
2. Presenting problems/problem acuity
3. Background information (vocational, legal, family, living environment)
4. Emotional/mental status (degree of danger to self/others, ability to participant in tx)
5. Client strengths and preferences
6. Recommendation for assessment or other referral
Comprehensive assessment ✔✔biopsychosocial assessment is the foundation which the clt record
is built and entails data gathering, analysis, and identification of problems/strengths which provide
the basis for treatment.
- multiple sources of information used in the development of biopsychosocial assessment such as
client self report, info from parents/spouses/family/probation officers/teachers/pcp and results of
medical/psychological tests.
Based on counselor's observations and experience, a clinical summary is formulated.
[Show More]
.png)
.png)





![Preview of [SOLVED] EDCO 740 / EDCO740 Quiz 1 (LATES 2021/2022 Graded A)](https://scholarfriends.com/storage/EDCO_740_Quiz_1.png)
