2020/2021 latest NURSING 306wk6 OB practice Qs.p
Document Content and Description Below
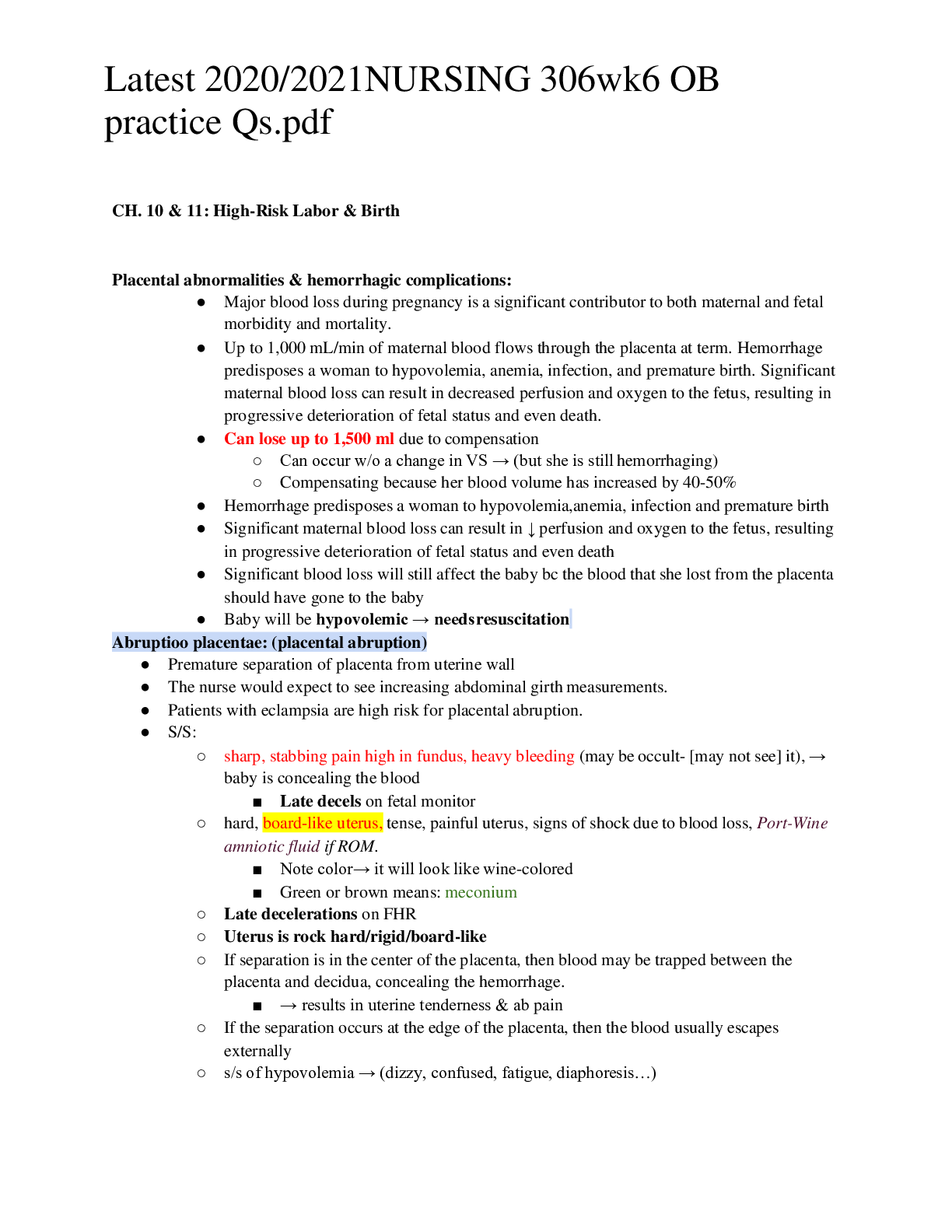
● Risks:
○ Prolonged PPROM r/t ↑ risk of chorioamnionitis, placental abruption & cord prolapse
● Predisposing fx:
○ ↑parity (had a lot of babies), adv. maternal age(>35 y.o),
○ short umbilical cord (baby starts to co
...
[Show More]
Last updated: 3 years ago
Preview 1 out of 37 pages
Instant download
Buy this Document to get the Full Access Instantly
Provided by Students Who Aced it
We Verify Document Content to Gurantee Accuracy
Reviews( 0 )
Document information
Connected school, study & course
About the document
Uploaded On
Feb 12, 2021
Number of pages
37
Written in
All

Additional information
This document has been written for:
Uploaded
Feb 12, 2021
Downloads
0
Views
102
Document Keyword Tags
Recommended For You
Get more on EXAM »

$16
496 Pages
TEST BANK for Essentials of Psychiatric Mental Health Nursing:...





$15
51 Pages