Sepsis Shock Case Study part 2
History of Current Problem:
Jack Holmes a 72-year-old Caucasian male brought to the ED by ambulance from a skilled nursing facility (SNF). According to report from the paramedic, when t
...
Sepsis Shock Case Study part 2
History of Current Problem:
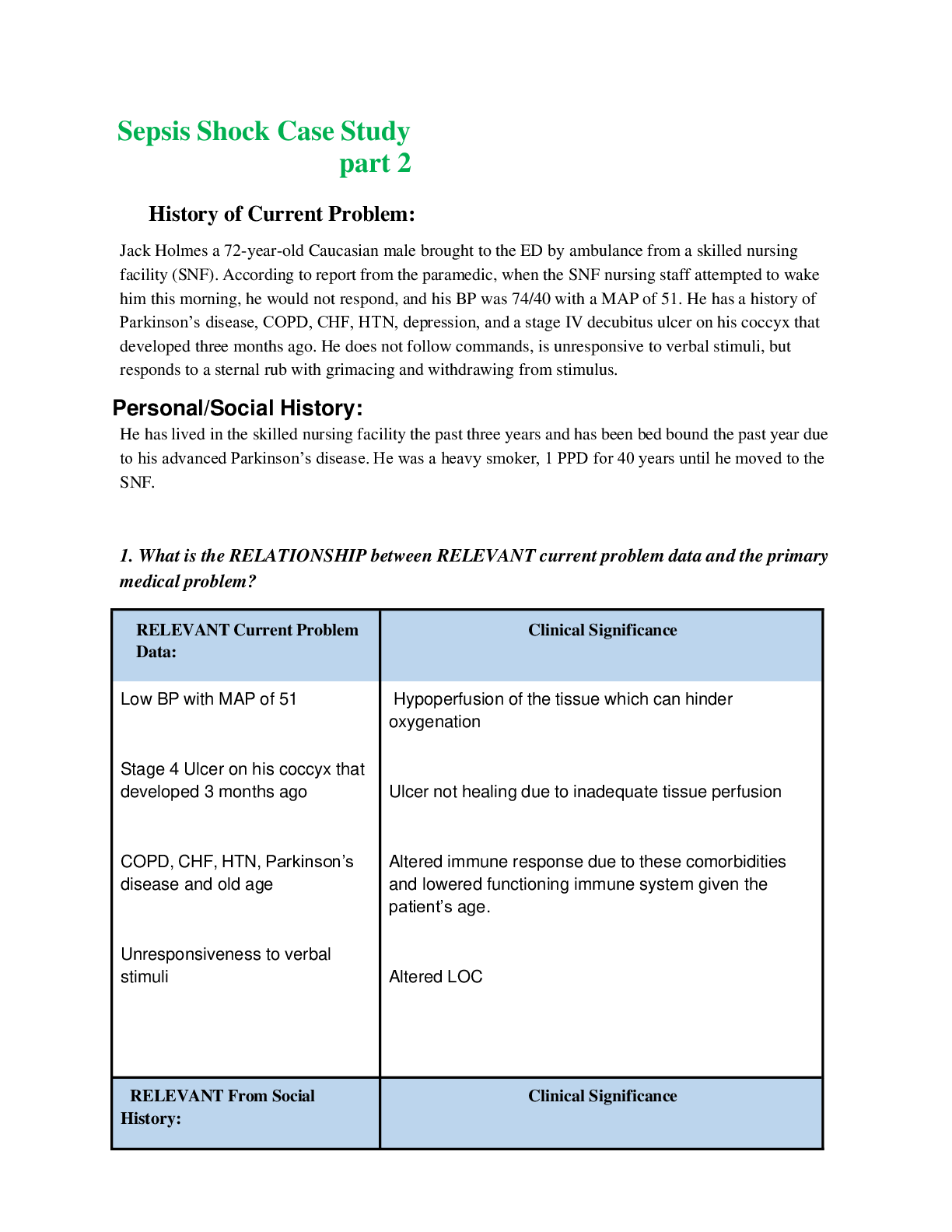
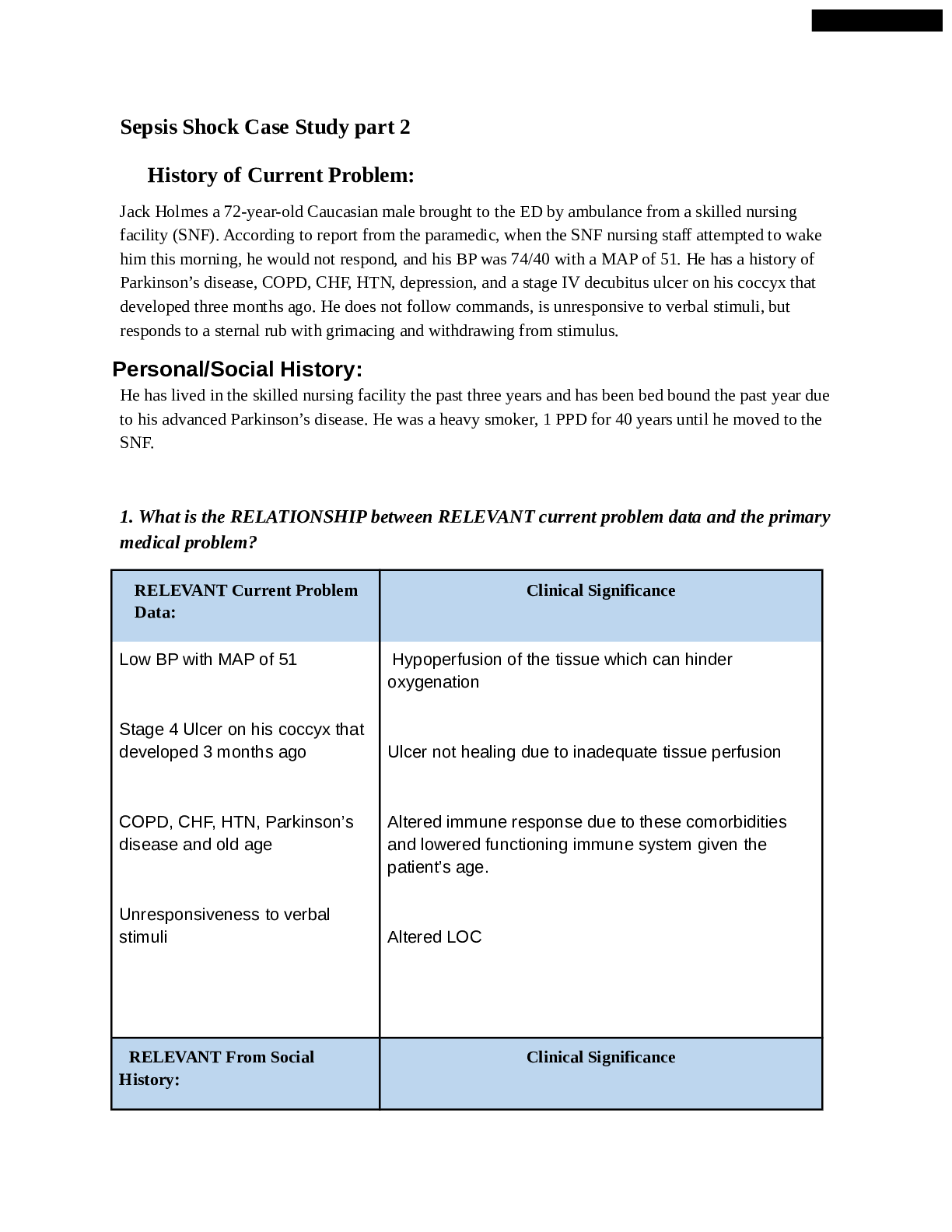
Jack Holmes a 72-year-old Caucasian male brought to the ED by ambulance from a skilled nursing facility (SNF). According to report from the paramedic, when the SNF nursing staff attempted to wake him this morning, he would not respond, and his BP was 74/40 with a MAP of 51. He has a history of Parkinson’s disease, COPD, CHF, HTN, depression, and a stage IV decubitus ulcer on his coccyx that developed three months ago. He does not follow commands, is unresponsive to verbal stimuli, but responds to a sternal rub with grimacing and withdrawing from stimulus.
Personal/Social History:
He has lived in the skilled nursing facility the past three years and has been bed bound the past year due to his advanced Parkinson’s disease. He was a heavy smoker, 1 PPD for 40 years until he moved to the SNF.
1. What is the RELATIONSHIP between RELEVANT current problem data and the primary medical problem?
RELEVANT Current Problem Data: Clinical Significance
Low BP with MAP of 51
Stage 4 Ulcer on his coccyx that developed 3 months ago
COPD, CHF, HTN, Parkinson’s disease and old age
Unresponsiveness to verbal stimuli Hypoperfusion of the tissue which can hinder oxygenation
Ulcer not healing due to inadequate tissue perfusion
Altered immune response due to these comorbidities and lowered functioning immune system given the patient’s age.
Altered LOC
RELEVANT From Social History: Clinical Significance
Skilled Nursing Facility
Bed bound due to his parkinson’s
Depression More exposure to pathogens or iatrogenic illness at the facility
Poor skin integrity, atrophy of muscle, renal calculi, DVT, isolation
Isolation, no interest or motivation in performing ADLs, unable to self advocate, withdrawing from peers
Patient Care Begins
Current VS P-Q-R_S-T Pain Assessment
T: 103.4 F/39.7 C (oral) Provoking /palliative Not responsive verbally, withdraws to pain, no other indicators of pain
P: 135 (irregular) Quality
R: 32 (regular) Region/radiation
BP: 76/39 MAP: 51 Severity
O2 Sat: 91% 2 liters n/c Timing
2. What VS data are RELEVANT and must be interpreted as clinically significant by the nurse?
RELEVANT VS Data Clinical Significance
Temperature is high There is an active infection in the body, this can also cause higher metabolism which can lead to fatigue
Respiration is high Compensating for low BP inorder to adequately oxygenate the tissues
BP is low
This is an indication of septic shock
O2 Sat is low (91%)
Could be normal for a patient with COPD who is a heavy former smoker with a history of 1 PPD for 40 years.
Current Assessment
General appearance Pale and warm to touch. Appears tense.
Respirations Tachypneic and working hard to breathe, intercostal and suprasternal retractions present. Breath sounds diminished and light crackles in lower lobes bilat. Nail beds have noticeable clubbing, barrel chest present.
Cardiac Pale, 1+ pitting edema lower extremities, systolic murmur with an irregular rhythm, radial pulses weak and thready, cap refill 3 seconds
Neuro Does not open eyes to sound or pain, withdraws to pain, incomprehensible sounds to painful stimuli, does not follow commands but does not resist when moved on a stretcher. PERRL
GI Distended abdomen, firm/nontender, bowel sounds hypoactive in all quadrants
GU Foley catheter placed to monitor urine output. 50 mL tea-colored urine with no
sediment, and no odor present
Skin Stage IV decubitus to coccyx 1 cm x 0.5 cm x 0.5 cm depth, wound bed with visual bone noted at the base with large areas of necrosis on both sides of the sacrum bone. When dressing was removed, a large amount of yellow/green purulent drainage on dressing with a foul odor. Mucus membranes dry and pale.
3. What Jack’s Glasgow Coma Scale score?
Eye opening 1
Verbal Response 2
Motor Response 4
Total 7
4. What assessment data are RELEVANT and must be interpreted as clinically significant by the nurse?
RELEVANT assessment Data Clinical Significance
Tachypneic and working hard to breathe, intercostal and suprasternal retractions present.
Breath sounds diminished and light crackles in lower lobes bilat.
Nail beds have noticeable clubbing, barrel chest present.
Pale, 1+ pitting edema lower extremities,
Low blood pressure and low level of oxygen can lead to tachypnea inorder to compensate for poor oxygenation.
It could indicate that the lungs aren’t functioning properly due to presence of fluids in the lungs as a result of CHF.
Chronic hypo-oxygenation of the tissues can lead to clubbing, COPD can lead to barrel chest.
Pitting edema due to his CHF, sluggish cap refill due to low BP
systolic murmur with an irregular rhythm, radial pulses weak and thready, cap refill 3 seconds
Does not open eyes to sound or pain, withdraws to pain, incomprehensible sounds to painful stimuli, does not follow commands but does not resist when moved on a stretcher.
Distended abdomen, firm/nontender, bowel sounds hypoactive in all quadrants
50 mL tea-colored urine with no sediment, and no odor present
Stage IV decubitus to coccyx 1 cm x 0.5 cm x 0.5 cm depth, wound bed with visual bone noted at the base with large areas of necrosis on both sides of the sacrum bone.
When dressing was removed, a large amount of yellow/green purulent drainage on dressing with a foul odor.
Mucus membranes dry and pale
Altered level of consciousness because the brain is not being adequately perfused due to shock
Distended abdomen indicates patient has ascites; firm bowel, hypo-active sounds indicate peritonitis. This reinforces patient’s diagnosis of septic shock.
This indicates patients liver and kidneys and not working properly. Tea colored urine is also a sign of pyelonephritis and failing liver. This could be a sign that the patient is starting to develop multi organ dysfunction syndrome.
Ulcer is not healing or progressively getting worse due to lack of oxygen to the tissues.
Purulent drainage indicates active infection.
Patient is dehydrated.
5. Interpret the rhythm
Regular or (irregular)? P wave yes or (no) PR QRS wide or (narrow)
Interpretation Clinical Significance
This is an a-fib because the rate is irregular, there is no p wave and the QRS is narrow. This can lead to clot formation which can cause stroke or PE. A- fib also leads to low cardiac output and low BP.
Lab/diagnostic Results:
6. What diagnostic results are RELEVANT and must be recognized as clinically significant to the nurse?
Radiology Report: Chest x-ray
Relevant Results Clinical Significance
Cardiac silhouette slightly enlarged. No infiltrates present. This is an indication of CHF, which can lead to low CO and low BP. Enlarged heart also requires extra myocardial oxygenation.
WBC: Hgb: Platelet Neutroph il Bands
Current: 18.5 13.1 250 85.2 3
Most Recent: 12.4 13.2 175 64 0
7. Address the results of the CBC- address each lab result
Relevant Results Clinical Significance Trend (Improve worsening stable)
WBC Active infection Bleeding or anemia
Thrombocytosis due to anemia or iron deficiency in his diet
Active infection Active infection Worsening
Hgb
Worsening
Platelet
Worsening
Neutrophils
Worsening
Bands
Worsening
Na: Potassiu m: Glucose Creatinin e Lactate PT/INR GFR
Current
: 147 5.2 172 1.6 7.4 1.6 45
Most Recent: 138 4.4 98 0.88 n/a 0.9 >65
8. Address the results of the BMP –address each result
Relevant Results Clinical Significance Trend (Improve worsening stable)
Sodium Hypernatremia can cause changes in LOC, seizures, cerebral edema Worsening
Potassium:
Hyperkalemia can lead to arrhythmia, respiratory distress, urine abnormalities all of the symptoms which are being presented by the client
Worsening
Glucose
Creatinine
Elevated glucose could be due to increased level of stress in the body.
Elevated creatinine level indicates renal hypoperfusion and dehydration
Worsening
Worsening
Lactate
Elevated lactic acid level indicates poor oxygenation of the tissues.
Worsening
PT/INR
GFR
Elevated PT/INR indicates poor liver function as it is not producing clotting factors, this can lead to increased risk of bleeding
Reduced GFR indicates hypoperfusion of the kidneys and poor kidney function, which is concerning because blood is not being filtered which will lead to waste build up in the
blood Worsening
Worsening
Albumin: T Bili: Alk Phos ALT AST
Current: 2.9 5.1 285 134 175
Most Recent: 3.1 0.9 48 17 12
9. Address the results of the liver panel
Relevant Results Clinical Significance Trend (Improve worsening stable)
Albumin
T. Bili
Alk Phos Hypoalbumin can be due to malnutrition. Due to lack of proper nutrients, the patient's wound is not healing.
An increase in T. Bili level may indicate that the liver damage or disease. Which could mean that the liver is not clearing bilirubin properly.
An elevated ALk Phos means that the liver is not functioning properly. Worsening
Worsening
Worsening
ALT
An increase in ALT can be due to damage or inflamed liver
Worsening
AST
An elevated level could indicate damage to liver and other organs
worsening
UA with Micro
Color
: Clarit y: Sp.
Gr. Prote in Nitrit e LE T RB
Cs WB
Cs Bacter ia Epitheli al
Curre nt: Tea Clear 1.0
50 NEG NEG NE G <5 <5 NEG None
Most Recen t: Yello w Clear 1.0
25 NEG NEG NE G <5 <5 NEG None
10. Address the results of the UA
Relevant Results Clinical Significance Trend (Improve worsening stable)
Tea colored urine and sp gravity 1.050, This indicates dehydration, acute kidney injury, or liver injury, which is causing it to produce high level of bilirubin Worsening
11. Lactate 7.4 Normal value 0.5-1 Critical value >2 Clinical significance
As hypoxemia progresses, cellular metabolism becomes anaerobic, which increases lactic acid levels. Excess lactic acid limits ATP production and cell function cannot be maintained. This impairment results in sodium accumulation and loss of potassium. Cellular edema occurs and further decreases cardiac output, while increasing capillary permeability. As a result, electrolytes and fluid enters cells causing damage and eventually cell death. Elevated levels of lactate are associated with sepsis and severe inflammatory response syndrome.
Based on your understanding of Lactate as it relates to shock identify 2 Nursing priorities and 2 interventions.
1. Impaired tissue oxygenation- Increase perfusion to organs
a. Intubation and ventilatory support to increase oxygenation and remove carbon dioxide. This also reduces the work of breathing, which helps prevent exacerbation of lactic acid production → lactate. .
b. Norepinephrine is a vasopressor that constrict blood vessel to keep MAP elevated. MAP >65 promotes kidney perfusion.
c. Prone and lateral positioning will help increase oxygen delivery.
2. Deficient Fluid Volume- Increase fluid and electrolyte accumulation within the body to prevent cellular edema and cell death and promote oxygenation.
a. Administer fluid bolus (0.9% NS) to help increase blood pressure, which results in improved perfusion.
b. Administer Vasopressin, which can lead to the prevention of fluid loss leading to an increase fluid in vessel and MAP.
12. What is the PROBLEM ?
The patient is in Septic shock. According to the lab values, it looks like the patient is starting to develop multi organ dysfunction syndrome.
13. Present the Pathophysiology of the problem and address -SIRS or MODS (does he have them or not and what supports that determination
Septic shock results from severe infection within the blood due to endotoxins causing vasodilation and a drastic fall in blood pressure. Perfusion of tissues decreases and vital organs cease to receive adequate oxygenation and functioning is altered. Septic shock is a medical emergency. The patient’s particular cause of sepsis could be related to the infected and necrosed wound from the ulcer in the coccyx. Additionally, the patient has several comorbidities, such as; CHF, COPD, HTN and parkinsons that place him at an increased risk for developing infections and being immunocompromised.
Since the patient has multiple signs that define SIRS, it is realistic to say that he has it.
For example, the patient’s fever is above 38C (39.7C), he is tachycardic (135 bpm), and tachypneic (32 bpm). At least three signs out of the four are present and fit the criteria for SIRS. Following the Sequential (sepsis-related) Organ Failure Assessment, The patient’s condition is indicating MODS due to MAP of less than 65, renal dysfunction as evidenced by elevated BUN and creatinine and UOP results. Additionally, bilirubin is elevated at 5.1, indicating hepatic impairment. The patient’s GCS score of 7 signifies CNS alteration and a comatose state. As mentioned previously, the patient is in respiratory distress as well as cardiovascular impairment as shown by an irregular and dangerous heart rhythm known as afib.
14. Looking at your orders for Jack – what is the purpose or rationale for each one?
Care Providers orders Rationale
Two large bore (18 g) IVs This allows the patient to receive medication and fluid rapidly.
Fluid bolus 0.9% NS 30 mL/kg (2250 mL) This is administered to improve fluid level of septic patients which will raise their blood pressure.
Raising blood pressure will help perfuse the tissues.
Blood cultures x2 This test is carried out to determine if there is a bacterial infection within the blood.
Performing 2 culture ensures the presence of infection in the bloodstream.
Urine culture This test is done to determine the pathogen that is causing the infection and the right antibiotic to treat the infection
Wound culture This test is carried out to determine the cause of sepsis and the type of antibiotic to use
Vancomycin 2 g IV after cultures collected This is a broad spectrum antibiotic that is used to treat infection until the main cause of the infection is determined
Clindamycin 600 mg IV every 6 hours
This is an antibiotic that is used to treat patient with infection
If MAP remains <65 after 2250 mL of 0.9% NS…start Norepinephrine 1-12 mcg/min to maintain MAP >65 An elevated MAP <65 initiate kidney perfusion. Norepinephrine is a vasopressor that constrict blood vessel to keep MAP elevated.
If MAP remains <65 after norepinephrine at 1 mcg/kg/min… start
Vasopressin 0.04 units/minute to maintain MAP >65 Vasopressin is considered an antidiuretic which can lead to the prevention of fluid loss leading to an increase fluid in vessel and MAP
Continuous cardiac monitor This detects changes in heart rhythm, rate and conduction
VS every 5-15” This is used to determine changes within a patient with sepsis
Acetaminophen 1000 mg PR every 6 hours PRN for fever >101 This is used to reduce fever which will then reduce body’s metabolic rate
15. Identify 3 Nursing Priorities (first part of nursing diagnosis- These should be active problems)
1. Impaired Gas Exchange
2. Ineffective tissue perfusion
3. Deficient fluid volume
4. Imbalanced nutrition less than body requirements
16. What will you do to address Jack’s psychosocial / emotional needs
As Jack’s nurse it is important to ensure his family is present for support during this time and that end of life decisions can be made in the event that his condition becomes irreversible.
Additionally, because Jack’s condition has caused an altered level of consciousness, in addition to the changes caused by his Parkinson’s Disease--it is important to educate the family and the patient when/if the condition improves and the patient is to heal and eventually be discharged. Given that there are potential long-term effects of septic shock and MODS, it is important to teach the patient and family members of any risks. The long-term effects may include insomnia, disabling muscle joint pains, decreased cognitive function, organ dysfunction, anxiety and/or depression, mood changes, etc. It is vital to address Jack’s emotional needs as well by having family support present but also working to develop coping skills to deal with his condition and the aftermath but also his depression from being bed ridden. This may include frequent reorientation and administration of antidepressants and anxiolytics. It is imperative to educate Jack on his condition and involve him in his plan of care, which may instill a sense of empowerment in him.
[Show More]


 All 16 Questions Fully Answered Graded A.png)
 (A Graded) Latest Questions and Complete Solutions.png)