Final Exam Study Guide
· Thyroid
o Diagnosis & Evaluation
- What labs are used to diagnose?
For diagnosis we check TSH, T3, and T4 TSH - normal 0.3-6
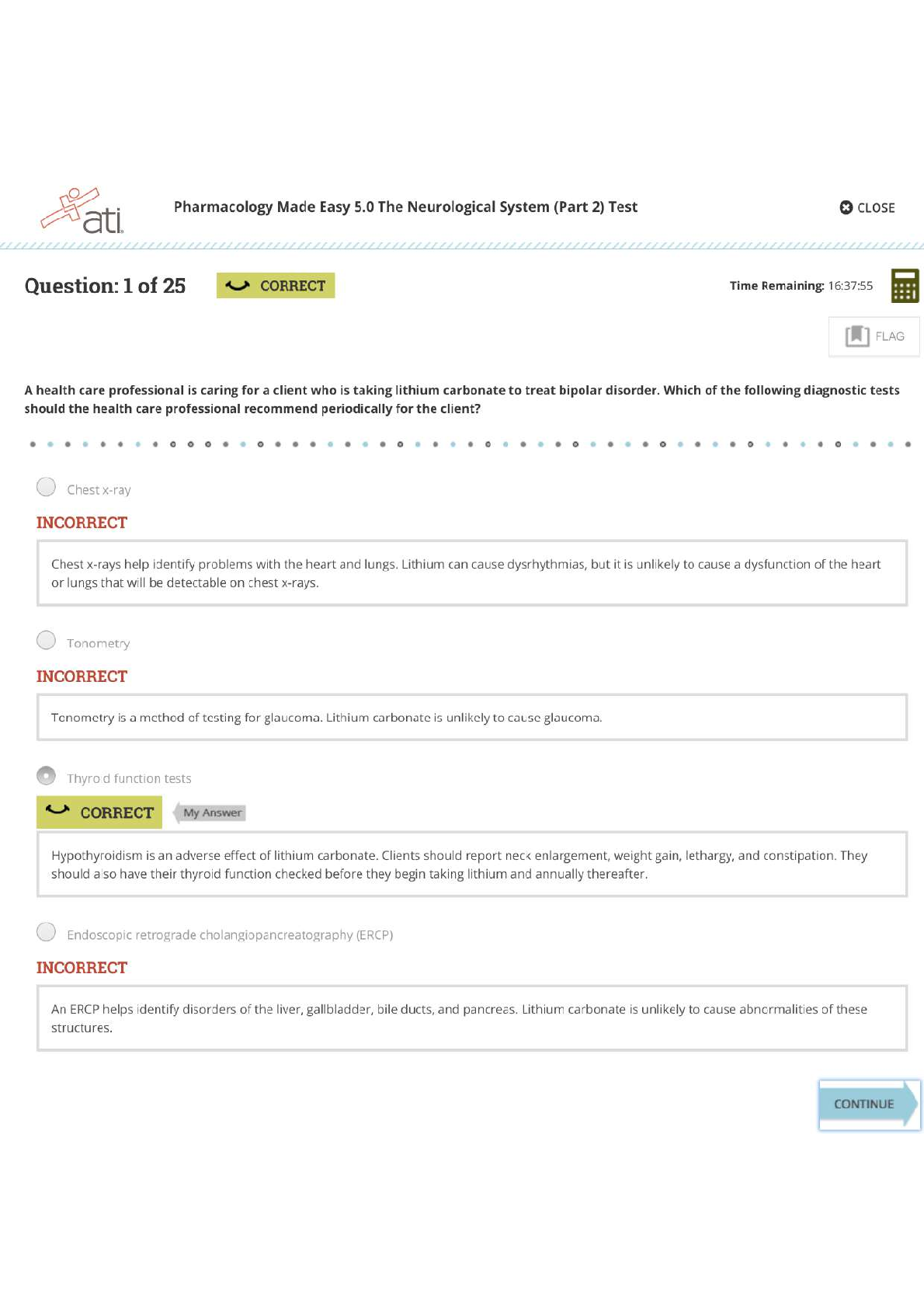
- in Hypothyroidism TSH would be elevated (>6) and T3
...
Final Exam Study Guide
· Thyroid
o Diagnosis & Evaluation
- What labs are used to diagnose?
For diagnosis we check TSH, T3, and T4 TSH - normal 0.3-6
- in Hypothyroidism TSH would be elevated (>6) and T3 and T4 would be decreased and the opposite would happen with hyperthyroidism.
- Hyperthyroidism - TSH low (<0.3) , T4 normal, and T3 High
· Etiology can be related to exogenous T4 ingestion, a concurrent non- thyroidal illness, or amiodarone-induced thyroid dysfunction – Low TSH, high T4, normal T3
· The possibility of a TSH producing pituitary tumor, which would need to be evaluated further with magnetic resonance imaging. – Normal/elevated TSH, elevated T4 and T3
· Primary hyperthyroidism. However, other reasons for this thyroid function test abnormality could be exogenous T3 ingestion, or a functioning adenoma. – Low TSH, normal T4, high T3
Baseline Data: Obtain serum levels of thyroid-stimulating hormone (TSH), free triiodothyronine (T3), and free thyroxine (T4). Check baseline CBC and LFTs prior to initiation.
Monitoring: Check CBC with differential if signs or symptoms of infection. Check LFTs for signs or symptoms of liver dysfunction.
- Timeframe for re-check of labs after starting levothyroxine
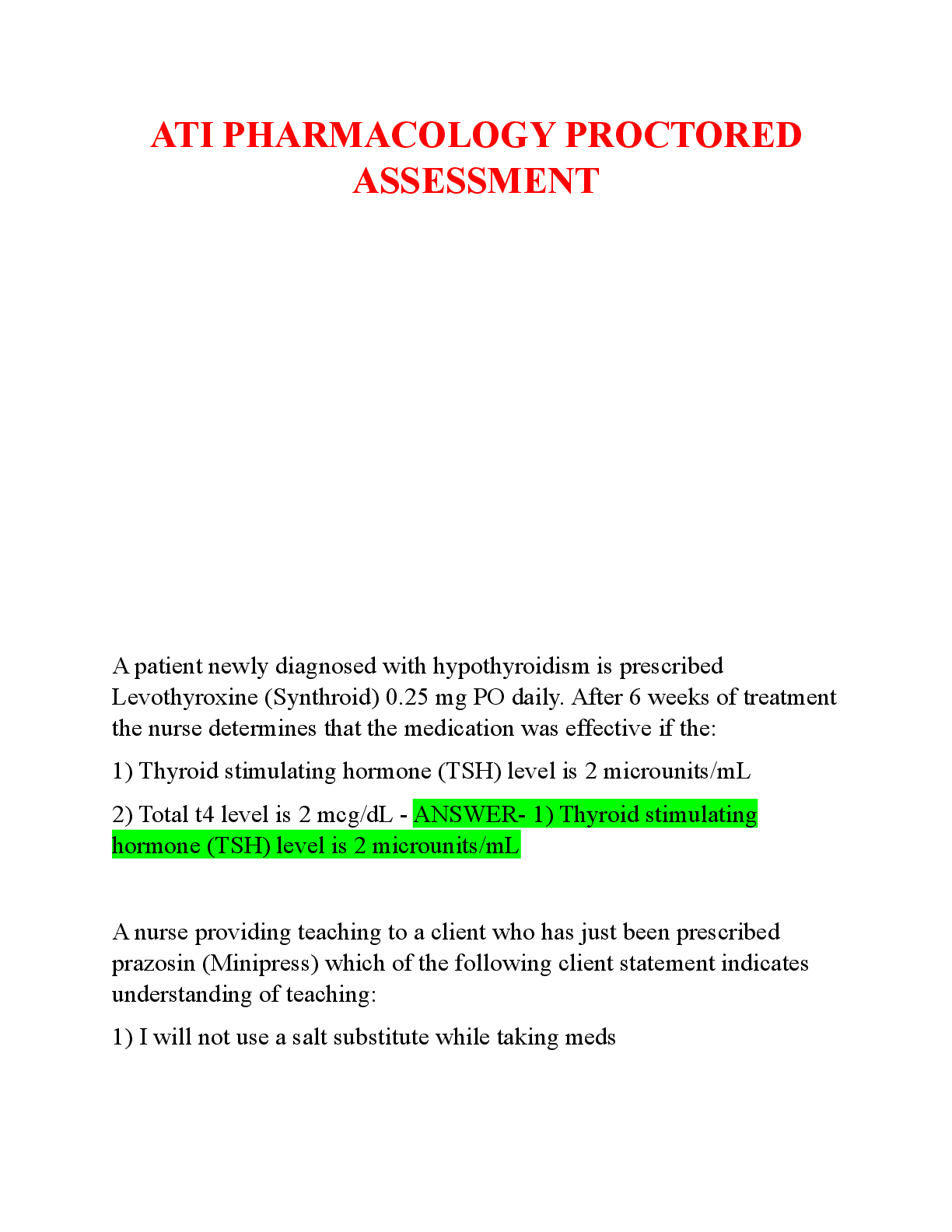
· Measurement of serum TSH is an important means of evaluation. Successful replacement therapy causes elevated TSH
levels to fall. However, TSH will not normalize quickly and often lags normalization of serum T3 and T4. Hence evaluation should not be done until 6 to 8 weeks after starting treatment.
- yearly after stable.
- Signs and symptoms of hypo and hyperthyroidism
o Treatment
- Treatment of thyroid storm
· Propylthiouracil (PTU): Preferred treatment for thyroid storm. Thyrotoxic crisis can occur in patients with severe thyrotoxicosis when they undergo major surgery or develop a severe intercurrent illness (e.g., infection, sepsis). The syndrome is characterized by profound hyperthermia (105°F or even higher), severe tachycardia, restlessness, agitation, and tremor. Unconsciousness, coma, hypotension, and heart failure may ensue. These symptoms are produced by excessive levels of thyroid hormones. Thyrotoxic crisis can be life threatening and require immediate treatment. High doses of potassium iodide or strong iodine solution are given to suppress thyroid hormone release. Methimazole is given to suppress thyroid hormone synthesis. Prevents the oxidation of iodine, therefore
inhibiting incorporation of iodine into tyrosine. Prevents iodinated tyrosine from coupling. A β-blocker is given to reduce heart rate. Additional measures include sedation, cooling, and giving glucocorticoids and intravenous (IV) fluids.
- Result of not treating hypothyroidism during pregnancy
· It can cause neuropsychological damage such as IQ, mental development, and derangement of growth.
P.418 - The effect of maternal hypothyroidism is limited largely to the first trimester, a time during which the fetus is unable to produce thyroid hormones of its own. By the second trimester, the fetal thyroid gland is fully functional, and hence the fetus can supply its own hormones from then on. Therefore to help ensure healthy fetal development, maternal hypothyroidism must be diagnosed and treated very early.
-due to the nonspecific symptoms or sometimes asymptomatic hypothyroidism, some experts recommend routine hypothyroidism as soon as pregnancy is confirmed. Further adjustments are based on the serum TSH levels, which should be monitored closely.
- Medication to treat symptoms of hyperthyroidism (notice this is treating symptoms and not the hyperthyroidism itself)
· Beta blockers for tachycardia (propranolol/atenolol most popular)
- Drug/Food/Supplement interactions with levothyroxine
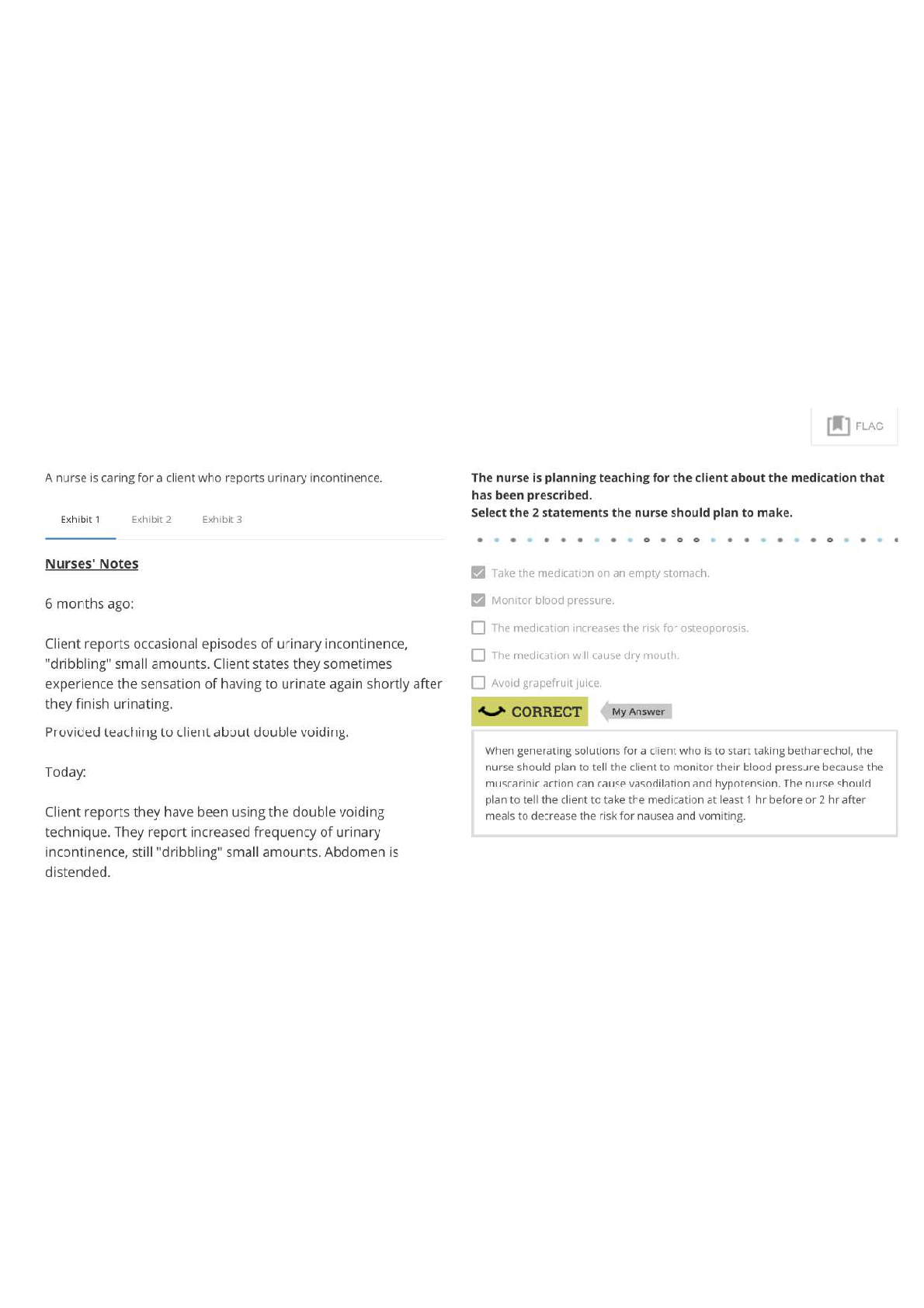
· Absorption of oral levothyroxine is reduced by food. Accordingly, to minimize variability in blood levels, levothyroxine should be taken on an empty stomach in the morning, at least 30 to 60 minutes before breakfast. Do not switch brands because they could have different levels.
· Absorption of levothyroxine can be reduced by the following drugs:
o • Histamine 2 (H2) receptor blockers (e.g., cimetidine [Tagamet])
o • Proton pump inhibitors (e.g., lansoprazole [Prevacid])
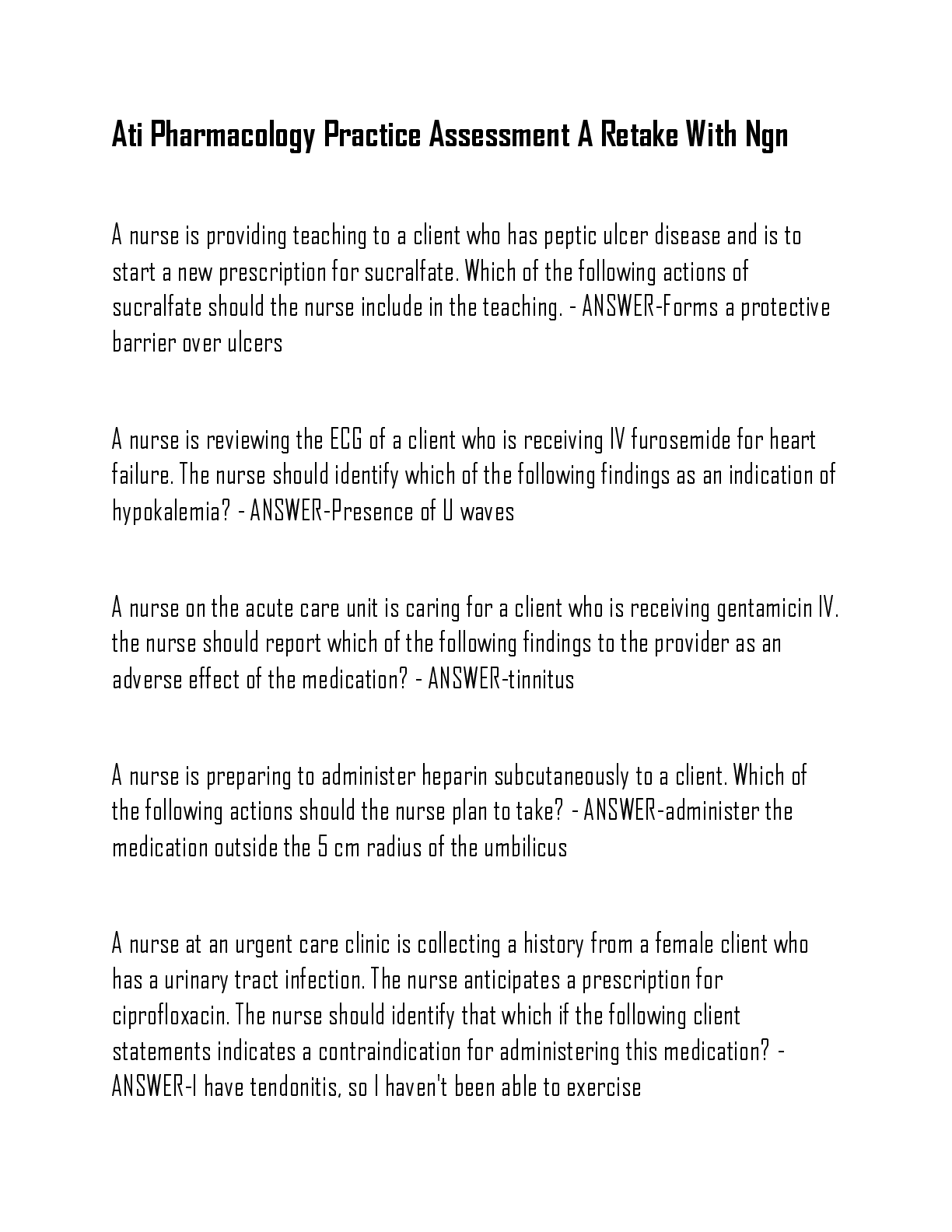
o • Sucralfate (Carafate)
o • Cholestyramine (Questran)
o • Colestipol (Colestid)
o • Aluminum-containing antacids (e.g., Maalox, Mylanta)
o • Calcium supplements (e.g., Tums, Os-Cal)
o • Iron supplements (e.g., ferrous sulfate)
o • Magnesium salts
• • Orlistat (Xenical)
· Levothyroxine can increase requirements for insulin and digoxin. When converting patients from a hypothyroid to a euthyroid state, dosages of insulin and digoxin may need to be increased.
· Several drugs can accelerate the metabolism of levothyroxine. Among these are
1. phenytoin (Dilantin),
2. carbamazepine (Tegretol, Carbatrol),
3. rifampin (Rifadin),
4. sertraline (Zoloft), and
5. phenobarbital. Accordingly, to maintain adequate levothyroxine levels, patients taking these drugs may need to increase their levothyroxine dosage.
· Warfarin.
o Levothyroxine accelerates the degradation of vitamin K–dependent clotting factors. As a result, the effects of warfarin are enhanced. If thyroid hormone replacement therapy is started in a patient taking warfarin, the dosage of warfarin may need to be reduced.
· Catecholamines.
o Thyroid hormones increase cardiac responsiveness to catecholamines, thereby increasing the risk for catecholamine-induced dysrhythmias.
Caution must be exercised when administering catecholamines to patients receiving levothyroxine and other thyroid preparations.
Diabetes
o How to confirm a diagnosis prior to beginning treatment
- Fasting plasma glucose >/=126 mg/dL, random plasma glucose >/= 200 mg/dL PLUS symptoms of diabetes, oral glucose tolerance test: 2-h plasma glucose >/= 200 mg/dL, hemoglobin A1c 6.5% or higher
o A1C
[Show More]