NURSING > CASE STUDY > NR 601 Week 2 ACC/AHA Guidelines Discussion Graded A (All)
NR 601 Week 2 ACC/AHA Guidelines Discussion Graded A
Document Content and Description Below
Last updated: 3 years ago
Preview 1 out of 13 pages
Instant download
Buy this Document to get the Full Access Instantly
Provided by Students Who Aced it
We Verify Document Content to Gurantee Accuracy
Also available in bundle (1)
Click Below to Access Bundle(s)

NR 601 STUDY PACKAGE (Discussions, Assignments, Quizzes, Midterm and Final Exams)
NR 601 STUDY PACKAGE (Discussions, Assignments, Quizzes, Midterm and Final Exams)
By PROF 5 years ago
$150.5
48
Reviews( 0 )
Document information
Connected school, study & course
About the document
Uploaded On
Mar 31, 2021
Number of pages
13
Written in
All

Additional information
This document has been written for:
Uploaded
Mar 31, 2021
Downloads
0
Views
123
Document Keyword Tags
Recommended For You
Get more on CASE STUDY »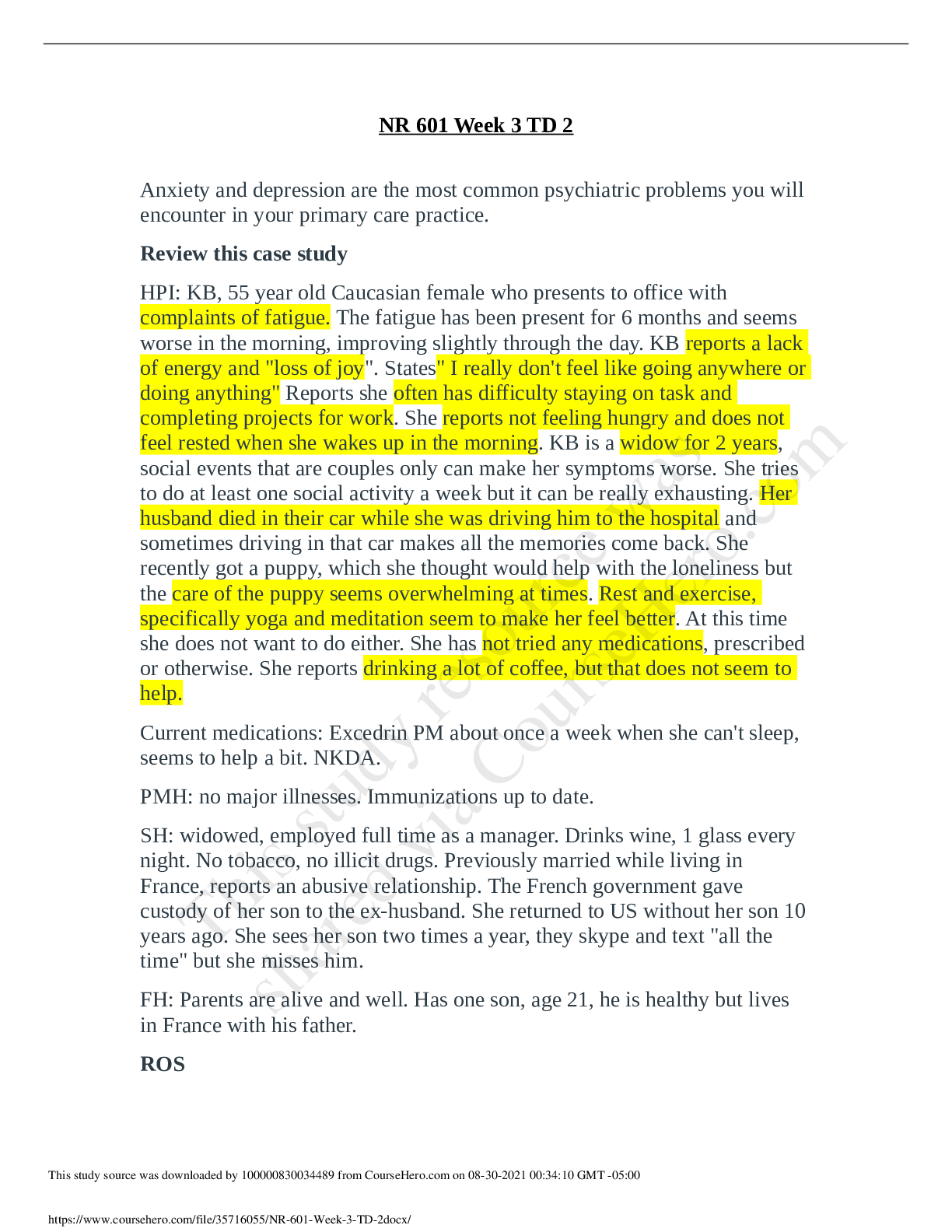
NR 601 Week 3 Psychiatric Disorders and Screening Discussion
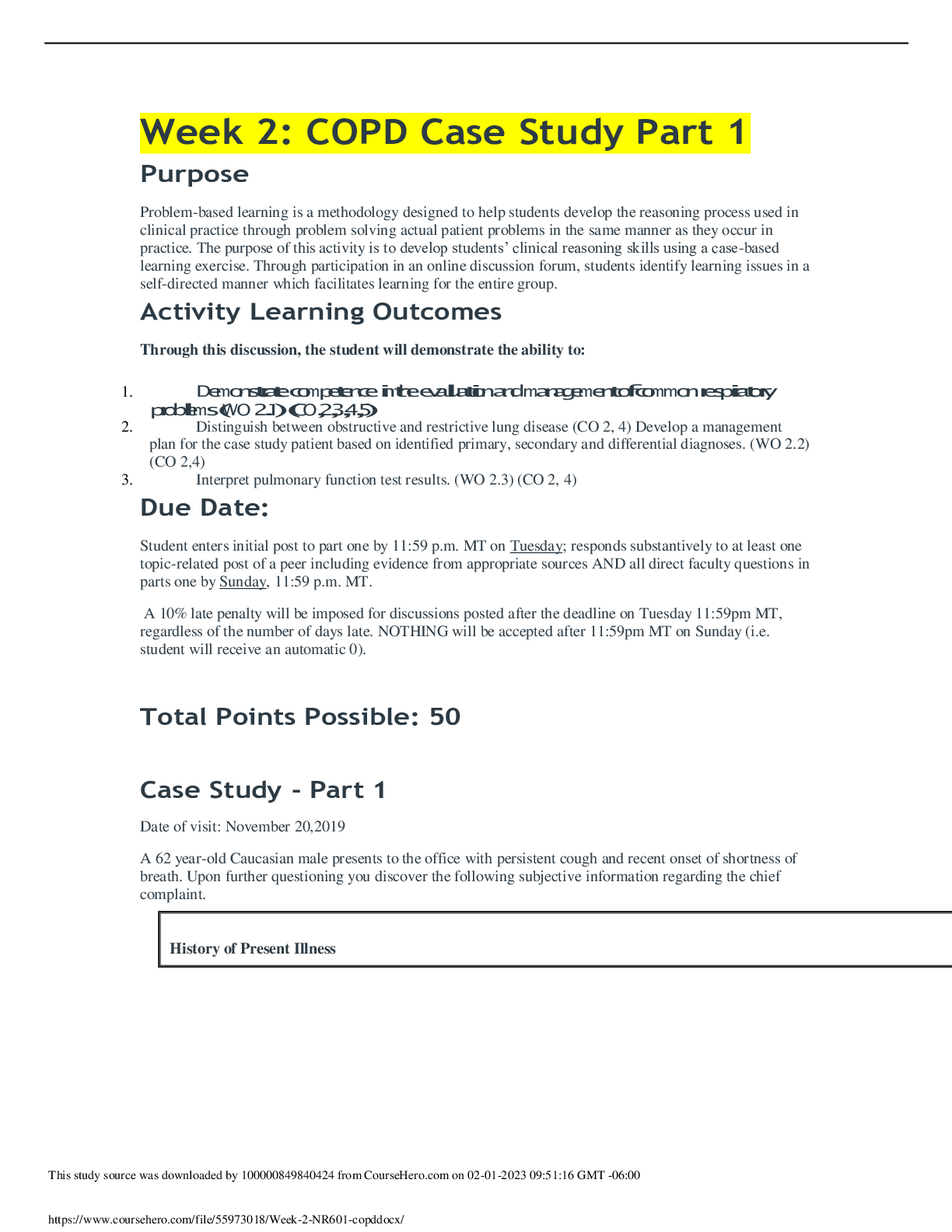
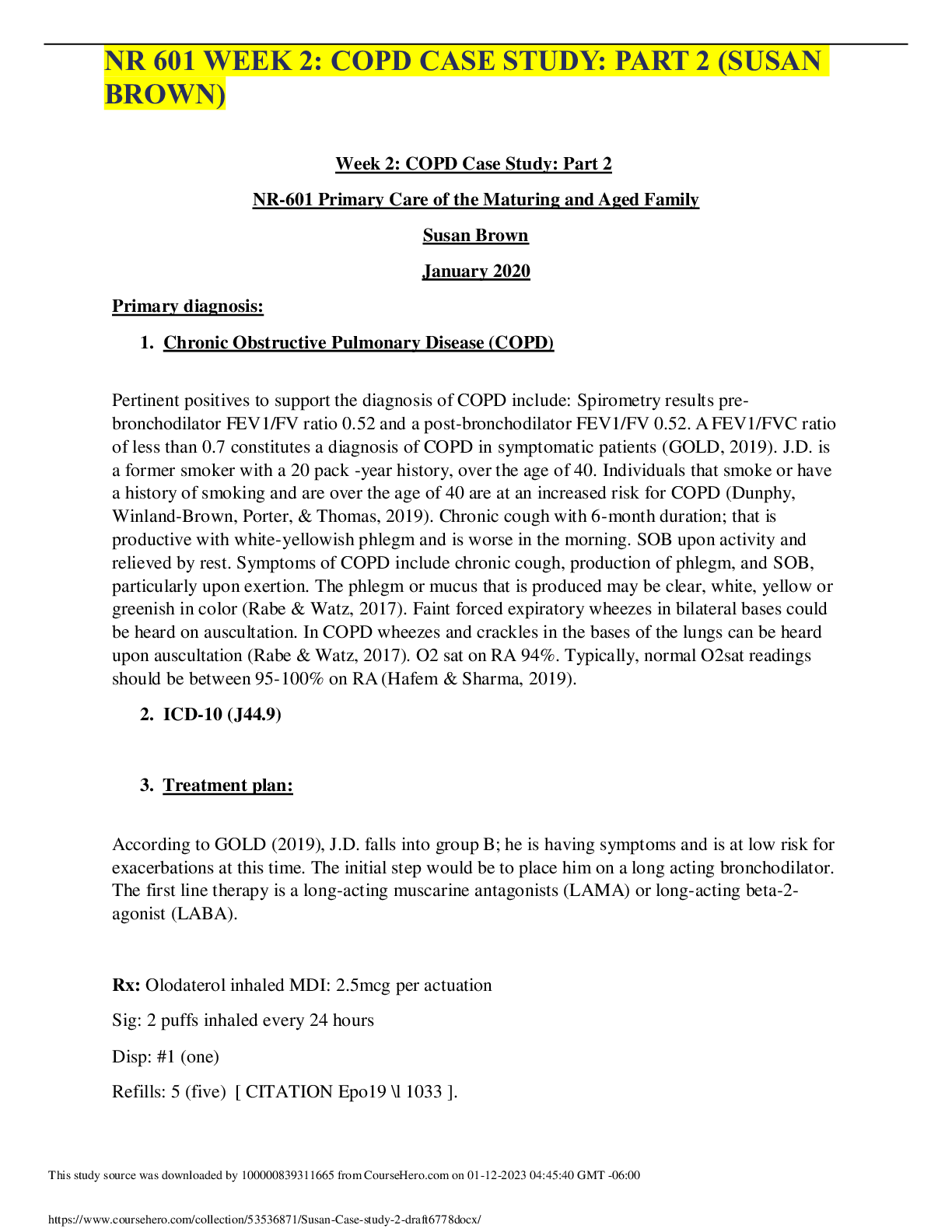
NR 601 Week 2 COPD Case Study Part 1 (Initial post, faculty an...
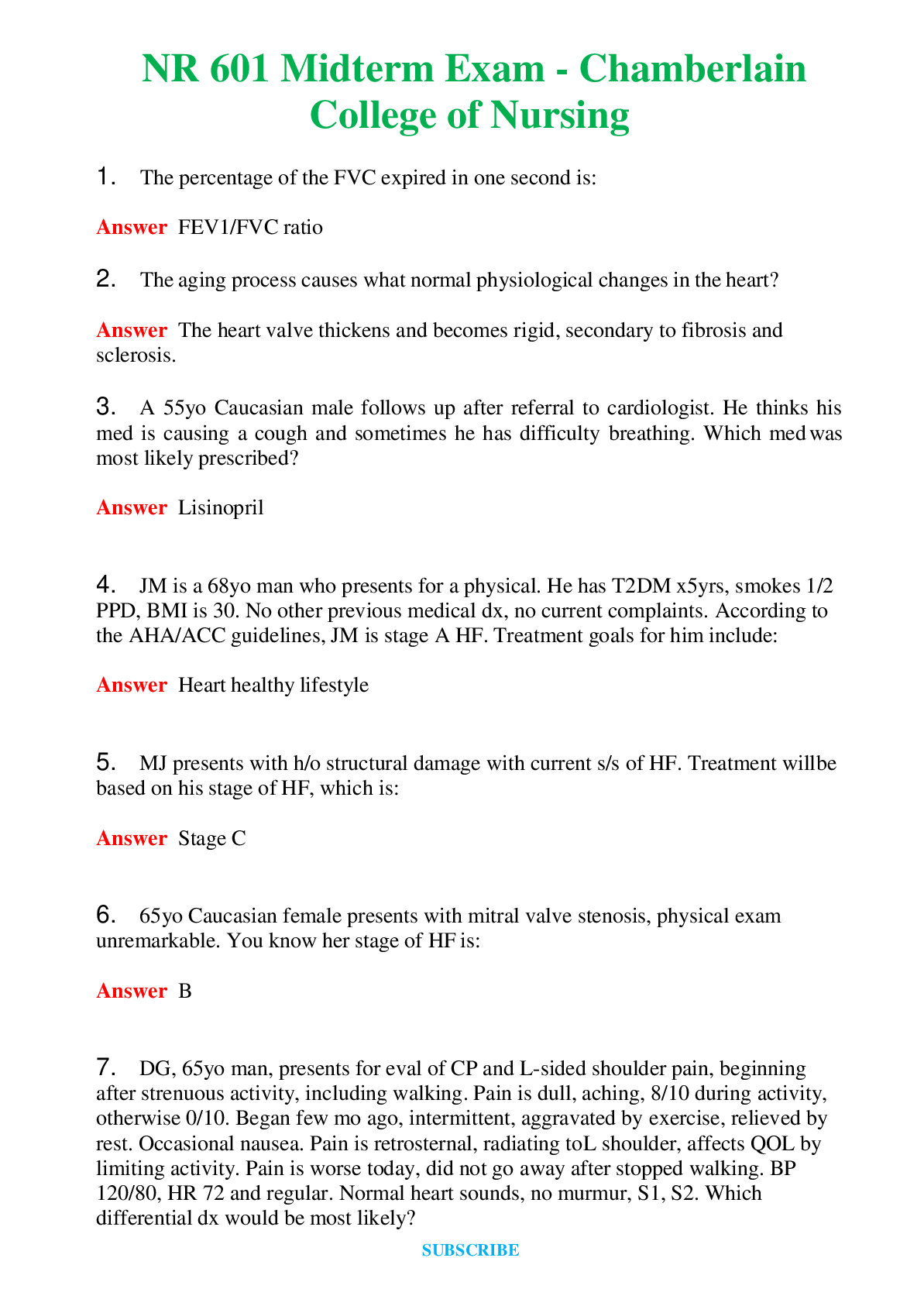
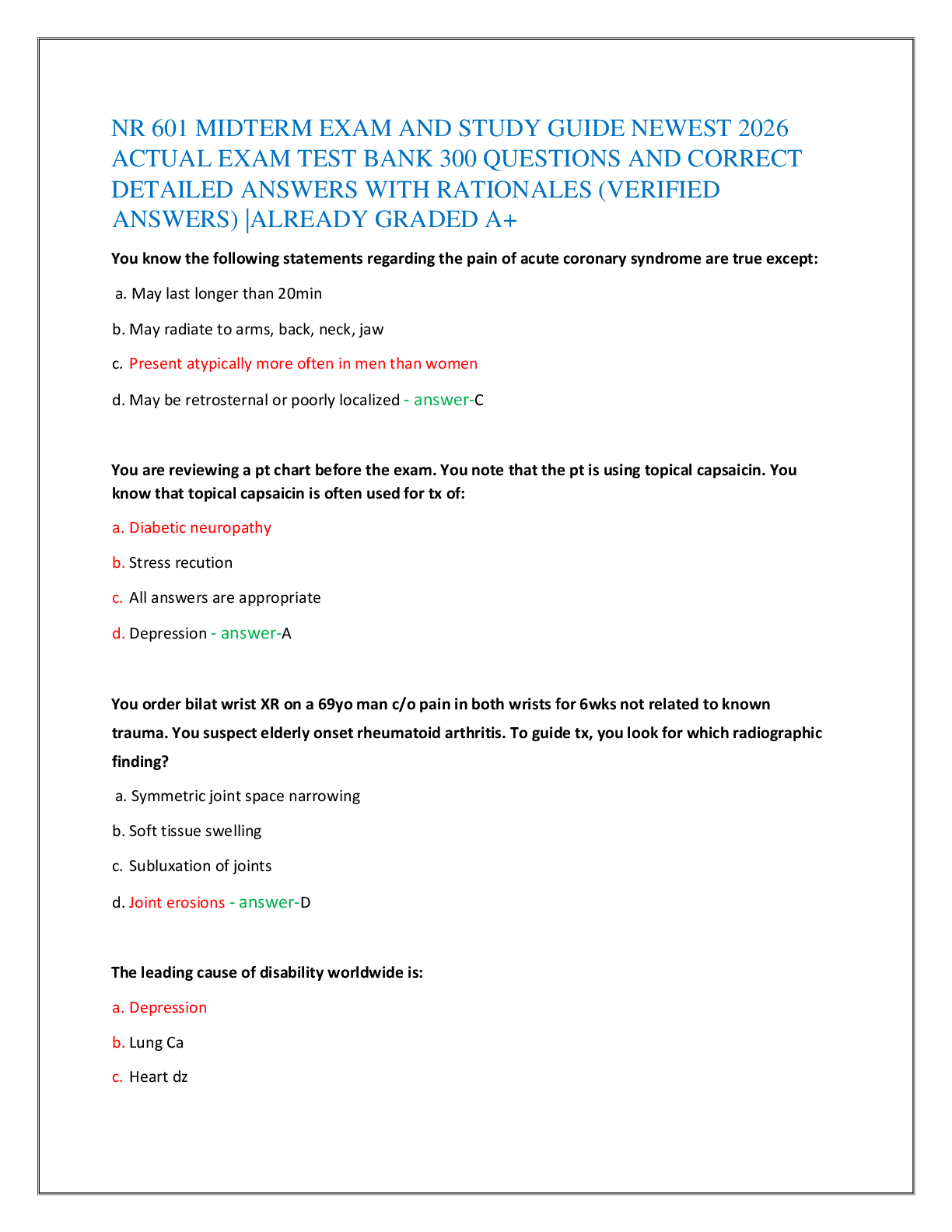
NR 601 Midterm Exam - Chamberlain College of Nursing Questi...
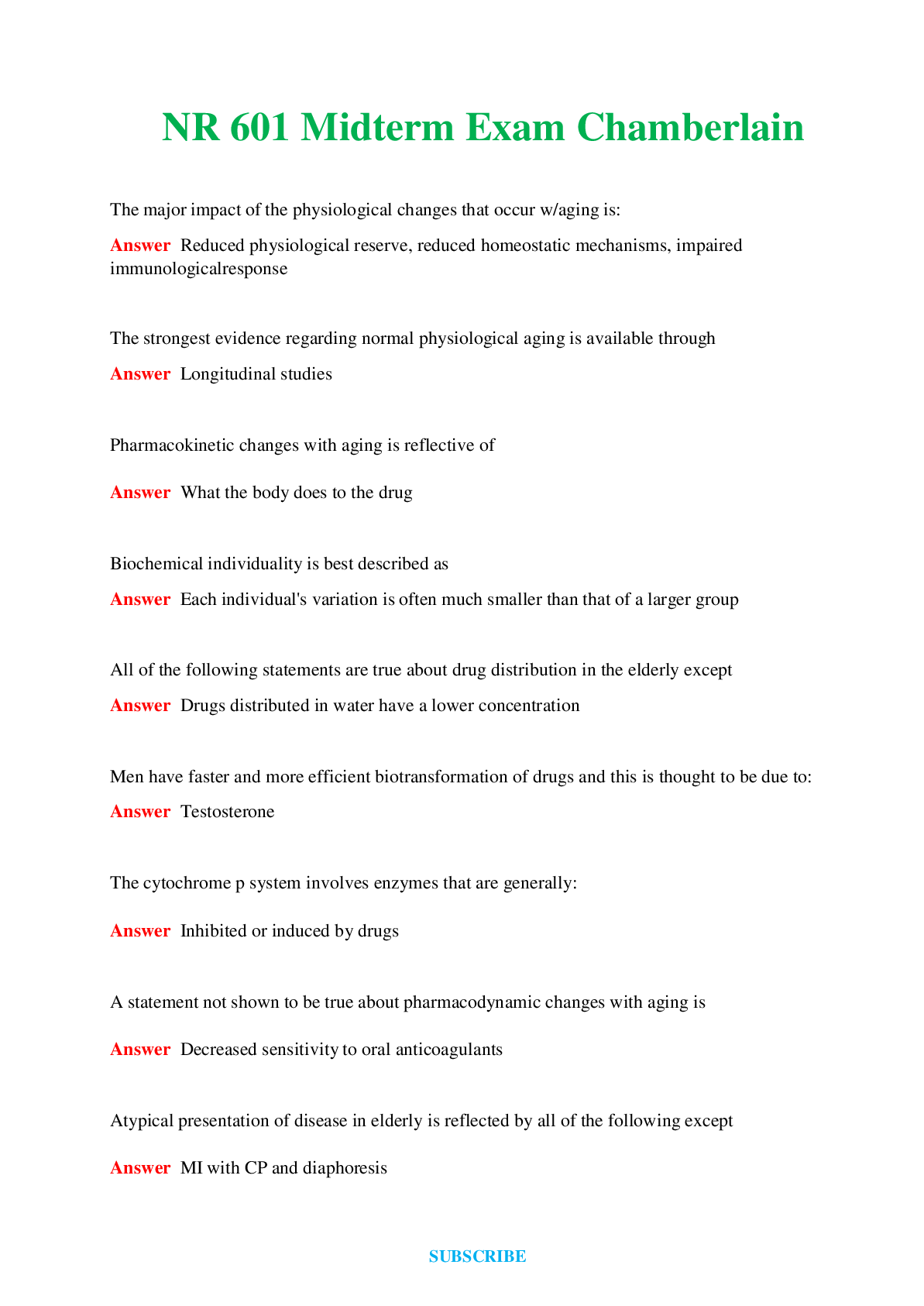
NR 601 Midterm Exam Chamberlain Questions and Answers (Veri...
NR 601 Midterm Exam (Version 2) Chamberlain Questions and An...
TEST BANK for Davis Advantage for Psychiatric Mental Health Nu...
Test Bank For Fundamentals of Nursing 11th Edition Potter Perr...