EMT-B Final Exam Study Guide Questions And Answers Latest Update 2022
$ 15.5
NCSBN question bank. latest document with almost 1000 questions with correct answers provided.
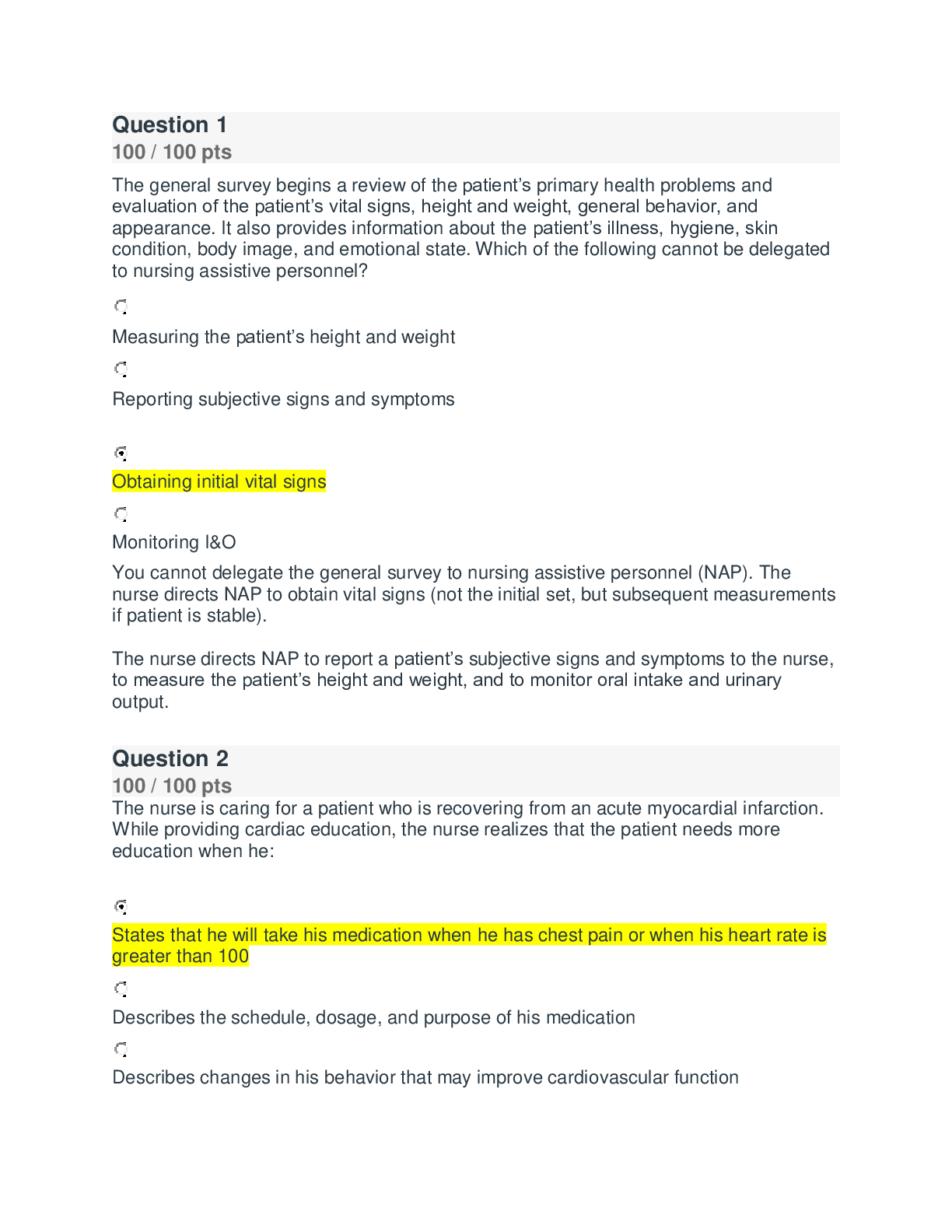
The general survey begins a review of the patient’s primary health problems and evaluation of the patient’s vital signs, height and weight, general behavior, and appearance. It also provides info ... rmation about the patient’s illness, hygiene, skin condition, body image, and emotional state. Which of the following cannot be delegated to nursing assistive personnel? Measuring the patient’s height and weight Reporting subjective signs and symptoms Obtaining initial vital signs Monitoring I&O You cannot delegate the general survey to nursing assistive personnel (NAP). The nurse directs NAP to obtain vital signs (not the initial set, but subsequent measurements if patient is stable). The nurse directs NAP to report a patient’s subjective signs and symptoms to the nurse, to measure the patient’s height and weight, and to monitor oral intake and urinary output. The nurse is caring for a patient who is recovering from an acute myocardial infarction. While providing cardiac education, the nurse realizes that the patient needs more education when he: States that he will take his medication when he has chest pain or when his heart rate is greater than 100 Describes the schedule, dosage, and purpose of his medication Describes changes in his behavior that may improve cardiovascular function Describes the benefits of taking his medication regularly The patient should not take medications for cardiovascular function intermittently. Medication should be taken on the regular prescribed schedule to prevent additional cardiac events. Describing changes in his behavior that may improve his cardiovascular function indicates that the patient understands steps he may take to improve his own health. The ability to accurately describe the schedule, dose, and purpose of his medication indicates that the patient understands his treatment. Understanding the benefits of taking his medication regularly should improve patient compliance with therapy. The patient is diagnosed with Bell’s palsy. The nurse assesses the patient and notices drooping of the patient’s right eye and the right side of his mouth. When the functions of the following nerves are compared, the most likely cause of these symptoms would be a dysfunction of: The trigeminal nerve (CN V) The glossopharyngeal nerve (CN IX) The seventh cranial nerve The oculomotor nerve (CN III) Assess cranial nerve (CN) VII (facial) by noting facial symmetry. Have patient frown, smile, puff out cheeks, and raise eyebrows. Expressions should be symmetrical; Bell’s palsy causes drooping of upper and lower face; cerebrovascular accident (CVA) causes asymmetry. Assess cranial nerve CN V (trigeminal) by applying light sensation with a cotton ball to symmetrical areas of face. Sensations should be symmetrical; unilateral decrease or loss of sensation is possibly due to CN V lesion or a lesion in higher sensory pathways. Assess cranial nerve CN III (oculomotor), IV (trochlear), and VI (abducens) by assessing extraocular movement (EOM) functioning. Ask patient to follow the movement of your finger through the six cardinal positions of gaze; measure pupillary reaction to light reflex and accommodation using a penlight. These cranial nerves are most likely to be affected by increasing intracranial pressure (ICP), which causes change in the pupil response or the pupil size; sometimes pupils change shape (more oval) or react sluggishly. ICP impairs EOMs. Damage to CN IX causes impaired swallowing; damage to CN X causes loss of gag reflex, hoarseness, and nasal voice. When the palate fails to rise and the uvula pulls toward the normal side, this indicates a unilateral paralysis. Which patient position maximizes the nurse’s ability to assess the patient’s body for symmetry? Supine Dorsal recumbent Prone Sitting Sitting upright provides full expansion of lungs and allows better visualization of symmetry of upper body parts. The supine position maximizes the nurse’s ability to assess pulse sites. The prone position is used only to assess extension of the hip joint. The dorsal recumbent position is used for abdominal assessment because it promotes relaxation of abdominal muscles. Before entering the room of a client on isolation where all protective barriers are required, the nurse first puts on the: Gown Eyewear Gloves Mask/respirator Apply the gown first, making sure that it covers all outer garments. Pull sleeves down to the wrist. Tie securely at the neck and waist. Apply gown first, making sure that it covers all outer garments. Pull sleeves down to the wrist. Next apply either a surgical mask or a fitted respirator around the mouth and nose. Goggles or a face shield is put on after the gown and mask are applied. Gloves are put on last. Droplet Precautions will be instituted for the patient admitted to the infectious disease unit with: Measles Herpes simplex Pulmonary TB Streptococcal pharyngitis Droplet Precautions are instituted when droplets are larger than 5 mm, as in the case of streptococcal pharyngitis. Contact Precautions are instituted for herpes simplex. Airborne Precautions are instituted for pulmonary TB and measles. The nurse needs to transfer the patient from the bed to the stretcher. The patient is unable to assist. Of the following, which would be the best technique for transferring the patient? Using the three-person lift technique Raising the head 30 degrees Having patient keeps arms to the side Correct Answer Using three nurses and a slide board Physical stress can be decreased significantly by the use of a slide board or a friction- reducing board positioned under a drawsheet beneath the patient. In addition, the patient is more comfortable using this method. The three-person lift for horizontal transfer from bed to stretcher is no longer recommended and, in fact, is discouraged. Lower the head of the bed as much as patient can tolerate. This maintains alignment of spinal column. Cross patient’s arms on chest to prevent injury to arms during transfer. The patient is an elderly gentleman who has been on bed rest for the past several days. When getting the patient up, the nurse should: Have the patient stand without dangling Tell the patient not to move his legs when dangling Tell the patient to hold his breath while dangling Raise the head of the bed and allow a few minutes before dangling Physiological changes associated with aging and prolonged bed rest may influence the effectiveness of the baroreceptors. In these patients, moving to the dangling position may cause a gravity-induced drop in blood pressure; thus, it is recommended to raise the head of the bed and allow a few minutes before dangling. Interventions to minimize orthostatic hypotension include movement of the legs and feet in the dangling position to promote venous return via intermittent contraction and relaxation of the skeletal leg muscles, and asking the patient to take several deep breaths before and during dangling. Dangling a patient before standing is an intermediate step that allows assessment of the individual before changing positions to maintain safety and prevent injury to the patient. The patient is a strict Orthodox Jew who has had a knee replacement and is using a continuous passive motion machine (CPM). The patient is concerned because the Sabbath is coming up, and he does not believe that he can use the machine on the Sabbath. The nurse should: Consult the rabbi to obtain permission for the patient Tell the patient that all he needs to do is turn his machine on and off Respect the patient’s wishes and not use the machine on the Sabbath Double the number of treatments the day before and after the Sabbath Orthodox Jews may not be able to operate a CPM machine during Sabbath and Holy Days. Consult the rabbi to obtain permission for the patient to use the CPM. Omitting a day of therapy may slow progress. Nurses should be responsible for turning the CPM on and off during the Sabbath and Holy Days. Only the physician can authorize changes in therapy. Check the physician’s orders to determine the patient’s activity level and types of exercise or assistive device. While ambulating, the patient becomes light-headed and starts to fall. The nurse should first: Ease the patient down to the floor Try to reach for a chair Push the patient back toward the bed Call for help If patient begins to fall, gently ease patient to floor by holding firmly onto gait belt; stand with feet apart to provide broad base of support, extend leg, and let patient gently slide to the floor. As patient slides, nurse bends knees to lower body. The nurse can cause more damage to self and patient by trying to catch patient. The nurse certainly will call for help, but this is not the first priority. The nurse must ensure that patient’s safety before getting help by easing him to the floor. When teaching the use of a three-point crutch gait, a nurse instructs the patient to: Move the left crutch and right foot, then move the right crutch and left foot Move the right crutch, left foot, left crutch, and right foot in sequence Move both crutches, then lift and swing the legs forward as far as the crutches Move both crutches and the affected leg first, then the stronger leg The proper sequence for the three-point crutch gait is to begin in tripod position. Advance both crutches and affected leg. Move stronger leg forward, stepping on floor. This is the proper sequence for the four-point gait, the two-point gait, and the swing-to gait. A patient with left hemiparesis is using a quad cane for ambulation. The following is the correct technique for the nurse to use in teaching the patient: Use the cane on the right side, with the cane moving forward first. Use the cane on the left side, with the left leg moving forward with the cane. Use the cane in either hand, with the right leg moving forward first. Use the cane in either hand, with the left leg moving beyond the forward placement of the cane. Begin by placing cane on the side opposite the involved leg. This provides added support for the weak or impaired side. Place cane forward 6 to 10 inches (15 to 25 cm), keeping body weight on both legs. This is incorrect in that the proper procedure begins by placing cane on the side opposite the involved leg to provide added support for the weak or impaired side. According to the National Association of Orthopaedic Nurses (NAON), which of the following is possibly the most effective cleansing solution for pin-site care? Chlorhexidine Normal saline Hydrogen peroxide None of the above The second group to develop Clinical Practice Guidelines is the United States–based NAON, which indicated that chlorhexidine 2 mg/mL solution is possibly the most effective cleansing solution for pin-site care. A British consensus group of orthopedic nurse experts recommends that pin sites be cleaned only with sterile normal saline or water to remove crusts around the pins (Walker, 2007). Walker found no definitive evidence to support a pin-site dressing containing an antimicrobial agent. Several studies found that although hydrogen peroxide is a common cleansing agent, it may cause damage to the healthy tissue surrounding the pin. The patient has a broken leg and needs to have a cast applied. When plaster of Paris is compared and contrasted versus the newer synthetic casts, which of the following statements is true? Plaster of Paris can tolerate earlier weight bearing than synthetic casts. Synthetic casts can withstand contact with water better than plaster. Plaster of Paris is more expensive than synthetic casts. Synthetic casts are lighter but take longer to set than plaster of Paris. Although the newer synthetic casts are more expensive than plaster of Paris, they can withstand contact with water without crumbling. A plaster of Paris cast has multiple rolls of open-weave cotton saturated with calcium sulfate crystals. These casts are heavier than synthetic casts and take 24 to 72 hours with no weight bearing or application of pressure while drying. Synthetic casts are lightweight, set in 15 minutes, and can sustain weight bearing or pressure in 15 to 30 minutes. When working with a patient who is being placed on an air mattress overlay, a nurse should: Keep clamps or pins attached to the sheets to keep them in place over the mattress Bring any plastic strips or flaps around the corners of the bed mattress Apply the preinflated overlay over the standard mattress Administer an analgesic after the patient is moved onto the mattress When preparing an air mattress/overlay, bring any plastic strips or flaps around the corners of the bed mattress. This secures the air mattress in place. Apply a deflated mattress flat over the surface of the bed mattress. The decision to administer analgesic would be based on the patient’s condition rather than on the procedure. Pins and other sharps should not be used, to avoid puncturing an air mattress. In a nursing home, an elderly patient drops his burning cigarette into a trash can and starts a fire. The most appropriate type of fire extinguisher for the nurse to use is the: Type D Type A Type C Type B Type A fire extinguishers are used for ordinary combustibles such as wood, cloth, paper, and plastic. A trash can fire would require a type A fire extinguisher. Type B fire extinguishers are used for flammable liquids such as gasoline, grease, paint, and anesthetic gas. Type C fire extinguishers are used for electrical fires. There is no Type D fire extinguisher. A general guideline for the assessment of a patient who has been restrained is: Every 15 minutes Every 1 hour Every 30 minutes Every 2 hours Following application, evaluate patient’s condition for signs of injury every 15 minutes. Frequent assessments prevent injury to patient and removal of restraint at earliest possible time. Observation and frequent assessments prevent complications such as suffocation, skin breakdown, and impaired circulation. However, the Joint Commission recommends that the patient’s condition be evaluated every 15 minutes. If the nurse restrains patient in an emergency situation because of violent or aggressive behavior that presents an immediate danger, a face-to-face physician assessment within 1 hour is needed to determine the patient’s continued need for restraints. Restraints should be removed at least every 2 hours. If the patient is violent or noncompliant, remove one restraint at a time and/or have staff assistance while removing restraints. Removal provides opportunity to change patient’s position, offer nutrients, perform full range of joint motion (ROJM), and toilet and exercise patient. A disaster is defined as: Any event or situation that results in multiple casualties and/or deaths An industrial accident and unplanned release of nuclear waste A catastrophic and/or destructive event that disrupts normal functioning An event that that results in human casualties that overwhelm the available health care resources A disaster is defined as a catastrophic and/or destructive event that disrupts normal functioning; it may include any anticipated or unexpected event whose effects lead to significant destruction and/or adverse consequences. Any event or situation that results in multiple casualties and/or deaths is called a mass casualty incident (MCI). An industrial accident and unplanned release of nuclear waste is classified as a technological disaster. A medical disaster is a catastrophic event that results in human casualties that overwhelm the available health care resources. The nurse frequently must assess a patient experiencing pain. When assessing the intensity of the pain, the nurse should: Use open-ended questions to find out about the sensation Offer the patient a pain scale to objectify the information Question the patient about the location of the pain Ask about what precipitates the pain Descriptive scales are a more objective means of measuring pain intensity. Use a pain intensity scale appropriate to the patient’s age, developmental level, and comprehension, and ask the patient to rate pain. An appropriate pain rating scale is reliable, easily understood, and easy to use; and it reflects changes in pain intensity. Asking the patient what precipitates the pain does not assess intensity, but rather assesses the pain pattern. Asking the patient about the location of pain does not assess the intensity of the patient’s pain. To determine the quality of the patient’s pain, the nurse may ask open-ended questions to find out about the sensation experienced (e.g., “Tell me what your pain feels like”). This approach assists in identifying the underlying pain mechanism (e.g., somatic or neuropathic pain), but it may not reveal intensity or changes in intensity. The patient is scheduled for surgery later that afternoon. He is scheduled to have PCA therapy after surgery. The nurse should: Teach the patient about PCA after the patient comes out of recovery Teach the patient about PCA before surgery and before preoperative medication administration Inform the patient’s family to watch him carefully and to depress the PCA administration button whenever they think he needs it Tell the patient not to use PCA unless he can no longer tolerate the pain Instruct surgical patients preoperatively. Encourage patients to push button on timing unit whenever they feel pain. Tell patient not to delay if he is experiencing pain. Pain is easier to prevent than to treat. Inform patient and family that patient cannot overdose with PCA if only the patient pushes the button. The family should not push the button unless instructed to do so by the nurse. The patient is in the hospital and has gone for major abdominal surgery. When the patient returns from the recovery room, the nurse expects that he most likely will be receiving pain medication: Intramuscularly By mouth Intravenously Via epidural route Research shows the epidural route to be most effective in managing postoperative pain from thoracic and abdominal surgeries. The nurse recognizes that anticipatory grieving can be most beneficial for a patient or family because it can: Promote separation of the ill patient from the family Be discussed with others Be done in private Allow time for the process of grief The benefit of anticipatory grief is that it allows time for the process of grief (i.e., to say good-bye and complete life affairs). Anticipatory grief may help people move through the stages of grief as needed, allowing time to grieve in private, to discuss the anticipated loss with others, and then to “let go” of the loved one. It is not most beneficial for grieving to take place only in private. It is important for grief to be acknowledged by others, and for the individual to be able to receive the support of others in the grieving process. Anticipatory grieving can be discussed with others in most circumstances. However, at times, anticipatory grief may be disenfranchised grief as well, meaning it cannot be acknowledged openly, socially sanctioned, or publicly shared, such as when a partner is dying of AIDS. The benefit of anticipatory grieving is not so much that it can be discussed in most circumstances, as this discussion also can occur with normal grief when the actual loss has occurred. Anticipatory grief is the process of disengaging or “letting go” that occurs before an actual loss or death. The benefit is not derived from the separation of the ill patient from the family as much as it is from the process of being able to say good-bye, to put life affairs in order; as a result, it can help a patient or family to progress to a higher emotional state. An appropriate technique for the nurse to implement when caring for a client’s body after death is to: Inquire about particular cultural or spiritual practices Remove tubes and lines if the patient is to be autopsied Cover the patient with a sheet and transfer him or her to the morgue Remove the client’s ID band and put a new gown on the client Respect the individuality of the patient and family and support their right to have cultural or religious values and beliefs upheld. Identify and tag the body, leaving identification on the body as directed by agency policy to ensure proper identification of the body for delivery to morgue or mortuary. After viewing, remove linens and gown, per agency policy. Place body in shroud provided by the agency. The shroud protects from injury to the skin, avoids exposure of the body, and provides a barrier against potentially contaminated body fluids. Removal of tubes and lines is contraindicated if an autopsy is planned. For a patient in the final stages of dying, a nurse expects to: Elevate the head of the bed as tolerated Keep the patient cool Encourage the patient to eat and drink more Avoid catheterizing the client Poor circulation of body fluids, immobilization, and inability to expectorate secretions cause rattles and bubbling. Elevate the head with a pillow or raise the head of the bed; gently turn head to the side to drain secretions. Coolness, color, and temperature changes in hands, arms, legs, and feet. Place socks on feet. Cover with light cotton blanket. Keep warm blankets on client. Decreased muscle tone and consciousness may lead to incontinence of urine and/or bowel. Change bedding as appropriate. Use an indwelling catheter for patient comfort. Do not force patient to eat or drink; give ice chips, soft drinks, juice, as possible. Provide mouth care. The nurse is providing nail care for the patient who wants his fingernails “done.” The nurse should: Soak the fingernails for no longer than 10 minutes Clean under the nails using the end of a cotton swab Clean under the nails using an orange stick Clip the fingernail gently to prevent injury Unless the patient has diabetes, allow patient’s feet and fingernails to soak no longer than 10 minutes. Goal is to soften skin and debris beneath nails, without causing excessive dryness. Obtain physician’s order for cutting nails (required by most agencies). Patient’s skin may be cut accidentally. Certain patients are more at risk for infection, depending on their medical condition. Check agency policy for appropriate process for cleaning beneath nails. Do not use an orange stick or end of cotton swab; these splinter and can cause injury. The nurse has been caring for a patient with a stage IV ulcer. The ulcer has been steadily improving and now almost is healed. The nurse, at this point, can classify the ulcer as a: Stage III pressure ulcer Stage I pressure ulcer Healing stage IV pressure ulcer Stage II pressure ulcer “Downstaging” of granulating wounds is NOT appropriate because the full-thickness repair process involves replacement of lost normal tissue with granulation tissue. For example, a granulating stage IV wound should NOT be “downstaged” to a stage III. Therefore, a granulating stage IV wound is classified most appropriately as a “granulating stage IV,” or a “healing stage IV.” If the stage IV wound is healed completely, it can be classified as a “healed stage IV,” which conveys that the wound now is filled with granulation tissue and is resurfaced with epithelium. Question 27 100 / 100 pts When evaluating a client, a nurse observes an unexpected outcome of treatment when the surrounding skin of an ulcer becomes macerated. The nurse should: Use dressings with increased moisture absorption Monitor the client for systemic signs and symptoms Obtain a wound culture Apply pressure-reducing devices Select a dressing that has increased moisture-absorbing capacity. Dressings that increase moisture absorption will result in dryer skin that is less macerated. A wound culture is not indicated for macerated skin unless an increase in drainage or development of necrotic tissue occurs. Pressure-reducing devices are not indicated for macerated skin. Macerated skin is a local reaction; the client would not need systemic monitoring unless the pressure ulcer extended beyond the original margins. The nurse decides that assistive personnel is able to assist with client care for contact lenses when the assistive personnel states: “Gloves aren’t necessary; the eye is a clean organ.” “It is normal for contact lens wearers to have red, teary eyes.” “I will check with the client to see if the lenses are disposable.” “If I am in a hurry I will use tap water for rinsing the lenses.” Let the patient be a resource in the care of each device. Although it is the nurse’s responsibility to ensure that patients do not damage the devices or injure themselves, patients familiar with their devices are likely to have an established routine and helpful tips. The replacement schedule is determined by the type of lenses the client wears; the client can provide that information. Tap water can contain microorganisms and may be absorbed into the lens, making it uncomfortable to wear. Clean, powder-free gloves are used to prevent the spread of microorganisms during care of contact lenses. Pain, tearing, discomfort, and redness can indicate conjunctivitis and should be referred to the client’s provider if symptoms persist. The name Tylenol is known as this medication’s: Chemical name Generic name Trade name United States Pharmacopeia A medication trade name or brand name is used to market the medication. The trade name has the symbol ™ at the upper right of the name, indicating a manufacturer’s trademark for the name (e.g., Panadol™, Tempra™, Tylenol™). The chemical name describes the medication’s composition and molecular structure, such as N-acetyl-para-aminophenol, commonly known as Tylenol. The chemical name rarely is used in clinical practice. A manufacturer who first develops a medication gives the generic name of a medication. Acetaminophen is the generic name for Tylenol. The generic name is the official name that is listed in official publications such as the United States Pharmacopeia (USP). The USP is a drug book that lists all drugs by generic name. Aspirin is known as AspergumTM’s: United States Pharmacopeia Chemical name Trade name Generic name A manufacturer who first develops a medication gives the generic name of a medication. Acetaminophen is the generic name for Tylenol. The generic name is the official name that is listed in official publications such as the USP The chemical name describes the medication’s composition and molecular structure, such as N-acetyl-para-aminophenol, commonly known as Tylenol. The chemical name rarely is used in clinical practice. A medication trade name or brand name is used to market the medication. The trade name has the symbol ™ at the upper right of the name, indicating a manufacturer’s trademark of the name (e.g., Panadol™, Tempra™, Tylenol™). The USP is a drug book that lists all drugs by generic name. The nurse is to administer several medications to the patient via the nasogastric (NG) tube. What should the nurse do first? Add the medication to the tube feeding being given Check for placement of the NG tube Administer all of the medications mixed together Crush all tablets and capsules before administration Check placement of feeding tube by observing gastric contents and checking pH of aspirate contents. Gastric pH should be 4 or less. This ensures proper tube placement and reduces the risk of introducing fluids into the respiratory tract. Never add medications directly to the tube feeding. Not all tablets can be crushed, such as sustained-release tablets, nor should all capsules be opened. Medications should be reviewed carefully before a tablet is crushed or a capsule is opened. To administer more than one medication, give each separately, and flush between medications with 10 mL of water. Keeping the medications separate allows for accurate identification of medication if a dose is spilled. In addition, some medications are not compatible with each other, and this may cause clogging of the tube. The patient is to receive three different medications via nasogastric tube. What is the total amount of water the nurse should prepare to administer? 30 mL of water 5 mL of water 15 mL of water 80 mL of water 30 mL of water would be administered before and after the medication and 15 to 30 mL between medications for a total of at least 90 mL. The nurse is teaching the patient how to use a topical medication. Which statement indicates an understanding of the procedure? “If the patch falls off, I will put a new one on in the same place.” “I can dispose of used materials in the household trash as usual.” “If my skin is irritated, I will cleanse it using water only.” “If the patch starts to come off, I can secure it with tape.” If skin is inflamed, instruct patients to use only warm water rinse without soap for cleansing. Instruct patient how to manage a transdermal patch that begins to peel off before the next dose is due. Rather than tape the patch or cover it, instruct the patient to remove the patch, clean the skin, and apply a new patch to a different area. Instruct the patient to wrap applicators, used patches, and similar materials and dispose into cardboard or plastic disposable containers. Careful disposal is necessary to ensure the safety of the patient, other adults, pets, and children. An expected response from a vaginal instillation is evident when: Local pruritus is evident A small amount of discharge that is the same color as the medication is noted White curd-like patches appear on the vaginal walls The vaginal walls are bright pink or red in color Some vaginal discharge that is the same color as the medication is an expected outcome after vaginal instillation. Local pruritus indicates inflammation or infection and is an unexpected outcome. Bright pink or red vaginal walls or white curd-like patches are signs of a possible yeast infection. Bright pink or red vaginal walls or white curd-like patches are signs of a possible yeast infection. Intradermal injections are administered correctly when the nurse: Injects at a 45-degree angle Selects a 22-gauge needle Uses a 1-inch needle Correct Answer Identifies the site at 3 fingerwidths below the antecubital space A site that is 3 to 4 fingerwidths below the antecubital space and 1 handwidth above the wrist and is free of bruises, inflammation, or edema is selected for intradermal injection. To administer an injection intradermally, use a tuberculin or small syringe with a short, fine-gauge (25 to 27) needle. The angle of insertion for an intradermal injection is 5 to 15 degrees. The nurse is preparing to start an infusion of ciprofloxacin to run as a piggyback infusion. For the system to run properly, the nurse must: Plug the piggyback into the lowest port on the primary bag’s tubing Stop the primary bag from running so the piggyback can run Hang the bag lower than the primary infusion Connect the bag to the upper Y-port of a primary infusion line A piggyback is a small (25 to 250 mL) IV bag or bottle connected to a short tubing line that connects to the upper Y-port of a primary infusion line or to an intermittent venous access. The set is called a “piggyback” because the small bag or bottle is set higher than the primary infusion bag or bottle. In the piggyback setup, the main line does not infuse when a compatible piggybacked medication is infusing. The port of the primary IV line contains a back-check valve that automatically stops the flow of the primary infusion once the piggyback infusion flows. After the piggyback solution infuses and the solution within the tubing falls below the level of the primary infusion drip chamber, the back-check valve opens, and the primary infusion starts to flow again. The patient is in respiratory distress but does not have COPD. The physician wants the patient to receive the highest possible concentration of oxygen. Which of the following would best meet this criterion? Correct Answer Plastic face mask with reservoir bag Venturi mask Face tent Simple face mask When used as a nonrebreather, the plastic face mask with a reservoir bag delivers 60% to 100% oxygen at appropriate flow rates. This oxygen mask maintains a high- concentration oxygen supply in the reservoir bag. Frequently inspect the bag to make sure it is inflated. If it is deflated, the patient breathes in large amounts of exhaled carbon dioxide. The simple face mask is used for short-term oxygen therapy. It fits loosely and delivers oxygen concentrations from 40% to 60%. The mask is contraindicated for patients with carbon dioxide retention because it will make the retention worse. A Venturi mask is a cone-shaped device with entrainment ports of various sizes at the base of the mask. The entrainment ports adjust to permit regulation of fractional inspired oxygen pressure difference (FIO2) from 24% to 60%. This mask is useful because it delivers a more precise concentration of oxygen to the patient. The face tent is a shield-like device that fits under the patient’s chin and sweeps around the face. It is used primarily for humidification and for oxygen only when the patient cannot or will not tolerate a tight- fitting mask. A patient is admitted to the emergency department following a motor vehicle accident. The patient is unconscious and has a broken jaw and facial lacerations. The patient’s breath sounds are diminished, and the doctor suspects atelectasis. The patient most likely is a candidate for: BiPAP None of the above CPAP Noninvasive ventilation Noninvasive ventilation, including CPAP and BiPAP, is contraindicated in cardiac or respiratory arrest, nonrespiratory organ failure, facial surgery or trauma, inability to protect the airway and/or high risk for aspiration, and inability to clear secretions. The physician has ordered that the patient receive percussion and vibration to help clear airway secretions. Where must the nurse place her hands? On the patient’s clavicles On the patient’s spine and sternum On the patient’s abdomen On the patient’s ribs Perform percussion, vibration, and shaking only over the ribs. The clavicles, breast tissue, sternum, spine, waist, and abdomen are never used for percussion and vibration. The nurse is caring for an infant who has been vomiting and who is having breathing problems. What should the nurse do to suction the infant? Place the infant in a prone position Place the infant in a supine position Suction only when a large amount of mucus is present Use bulb syringe and compress the bulb after it is in place Position infants with breathing problems or excessive vomitus in prone position. Maintain healthy infants in supine position. Airways of infants and children are smaller than those of an adult; even small amounts of mucus cause airway obstruction. Compress syringe before insertion to prevent forcing secretions into infant’s bronchi. In the acute care environment, what is the wall suction pressure setting for adults? 100 to 120 mm Hg 20 to 40 mm Hg 100 to 150 mm Hg 80 to 100 mm Hg Adults require suction of 100 to 150 mm Hg. Suction pressure of 20 to 40 mm Hg is too low for adults; it is even less than infants or preterm infants require. 80 to 100 mm Hg is also too low for adults, although it would be appropriate for infants. 100 to 120 mm Hg would be appropriate for children. A patient develops respiratory distress during suctioning of the endotracheal tube. What should the nurse do? Encourage the patient to cough and deep-breathe Administer oxygen directly through the catheter Remove and reinsert the catheter Continue to remove thick secretions If patient develops respiratory distress during the suction procedure, immediately withdraw catheter, and supply additional oxygen and breaths as needed. In an emergency, disconnect suction, and attach oxygen at prescribed flow rate through the catheter. The nurse is caring for a patient who is sedated and is on a ventilator. When assessing the patient, the nurse notes that there is a sound that may indicate that air is escaping around the tube. What should the nurse do? Suction the patient Verify correct position of the tube and assess cuff pressure Repeat taping or securing procedure Prepare for reintubation If air is escaping around the tube, verify correct position of tube. If tube position is correct, assess proper cuff inflation. If tube position is incorrect, reposition according to protocol or notify physician. In case of unexpected extubation, remain with patient, call for assistance, assist respirations with bag-valve mask as needed, assess patient for airway patency, spontaneous breathing, and vital signs, and prepare for reintubation. Air escaping from around the tube is not usually an indicator of extubation. Repeat taping or securing procedure when there is movement of the endotracheal tube. Suction the patient if unequal breath sounds are noted. Evaluate ET tube for proper depth before and after ET tube care. Preparation for tracheostomy care in the acute care environment includes: Preparing cotton applicators with normal saline and hydrogen peroxide Using clean technique, gloves, and supplies Removing and cleaning the outer cannula Placing the patient in high-Fowler’s position Open two cotton-tipped swab packages, and pour normal saline on one package and leave the other package dry. Open sterile tracheostomy kit. Apply gloves. Keep dominant hand sterile throughout procedure. Assist patient to a position that is comfortable for both nurse and patient (usually supine or semi-Fowler’s). While touching only the outer aspect of the tube, remove the inner cannula with nondominant hand. Drop inner cannula into hydrogen peroxide basin. The nurse is caring for a patient who is comatose and on a ventilator. When she enters the room, she notices that the patient’s trachea has shifted toward the left side of the patient’s neck, and he has become tachycardic. She assesses the patient’s blood pressure and notes that it is 84/38. The nurse calls for help, knowing that the patient has a: Pneumothorax on the right side Myocardial infarction Pneumothorax on the left side Hemothorax A tension pneumothorax occurs from rupture in the pleura when air accumulates in the pleural space more rapidly than it is removed. If left untreated, the lung on the affected side collapses, and the mediastinum and trachea shift to the opposite (unaffected) side. The patient has sudden chest pain, a fall in blood pressure, and tachycardia; and cardiopulmonary arrest can occur. Patients with chest trauma, fractured ribs, and invasive thoracic bedside procedures (such as insertion of central lines), and those on high-pressure mechanical ventilation are at risk for tension pneumothorax. A hemothorax is a collapse of the lung caused by an accumulation of blood and fluid in the pleural cavity between the chest wall and the lung, usually as a result of trauma. Nothing in this scenario would suggest myocardial infarction. What condition is indicated when a patient with a chest tube experiences sharp stabbing chest pain without a change in pulse or blood pressure? Pneumonitis A tension pneumothorax A myocardial infarction Tube displacement Sharp stabbing chest pain with or without decreased blood pressure and increased heart rate may indicate a tension pneumothorax. A chest tube is not an expected treatment for pneumonitis. Tube displacement is an unexpected outcome and can lead to increased pneumothorax. Immediately apply pressure over chest tube insertion site. Myocardial infarction pain is expressed as “crushing” or “pressure” over the sternal area. Which of the following is the correct positioning for a patient after a chest tube has been inserted for a hemothorax? Supine High-Fowler’s Side-lying Semi-Fowler’s High-Fowler’s position to drain fluid (hemothorax). After the tube is placed, assist patient to a comfortable position. Supine does not facilitate drainage or removal of air or fluid, and side-lying does not facilitate lung expansion. Semi-Fowler’s to high-Fowler’s position to evacuate air (pneumothorax). What is the expected amount of drainage for an adult patient with a pleural chest tube? Correct Answer 100 to 3000 mL during the first 3 hours 400 to 500 mL during the first 24 hours 10 to 50 mL during the first 2 hours 200 mL during the first 24 hours In the adult, between 100 and 3000 mL of fluid may drain from a pleural tube during the first 3 hours after insertion. The 24-hour rate is 500 to 1000 mL. The nurse finds a patient lying on the bathroom floor. The patient is unresponsive and has a pulse but is not breathing. What should the nurse do first? Start chest compressions until an AED is available Give 2 breaths using a bag-mask device Give 2 breaths using mouth-to-mouth without a barrier device Give 2 breaths using a mouth-to-mouth with barrier device and watch for chest movement Give 2 breaths using a mouth-to-mouth with barrier device or mouth-to-mask device or bag-mask device. Watch for chest rise and fall. In a hospital setting where protected methods of artificial ventilation are available, mouth-to-mouth without a barrier device is not recommended because of the risk for microbial contamination. Watch for chest rise and fall. Motion, by itself, could be caused by fasciculation and is not indicative of air moving into and out of the chest. Airway always precedes circulation in the basic life support protocol. A nurse needs to specifically prevent air emboli that may result from IV therapy. What should the nurse make sure to do to prevent air emboli? Use a needleless system Prime the tubing completely Select a larger-gauge needle or catheter Check for medication compatibility Prime infusion tubing by filling with IV solution. Be certain tubing is clear of air and air bubbles. Large air bubbles can act as emboli. A needleless system does not specifically prevent introduction of air emboli. Medication incompatibility may lead to crystallization of the medication and my cause emboli to form from precipitate. It will not lead, however, to air embolism. Catheter size does not contribute to emboli formation. Which of the following steps is necessary when a patient is prepared for IV insertion? Shaving the hair from the site Selecting a proximal site in an extremity Vigorously taping and massaging the selected vein Applying a tourniquet 4 to 6 inches above the selected site Apply a flat tourniquet around the arm, above the antecubital fossa or 4 to 6 inches (10 to 15 cm) above proposed insertion site. Do not shave the area. Shaving may cause microabrasions and may predispose to infection. Use the most distal site in the nondominant arm, if possible. Vigorous friction and multiple tapping of the veins, especially in older adults, may cause hematoma and/or venous constriction. The nurse is caring for a patient who receives intermittent intravenous antibiotic therapy. Between doses, the nurse uses intravenous fluid to keep the vein patent. At what infusion rate should he/she set the IV to achieve that goal? 75 mL/hour 5 mL/hour 50 mL/hour Correct Answer 15 mL/hour The minimal rate used to keep a vein patent is about 10 to 15 mL/hour. What should the nurse do when discontinuing a peripheral IV? Keep the hub perpendicular to the skin Inspect the catheter for intactness after removal Withdraw the catheter quickly Apply pressure to the site for 1 minute Inspect catheter for intactness after removal, noting tip integrity and length. Place clean sterile gauze above site, and withdraw catheter, using a slow, steady motion. Keep the hub parallel to the skin. Do not raise or lift catheter before it is completely out of the vein, to avoid trauma or hematoma formation. Apply pressure to the site for 2 to 3 minutes, using a dry, sterile gauze pad. Secure with tape. Note: Apply pressure for 5 to 10 minutes if patient is on anticoagulants. What should the nurse do to decrease the potential for infection related to IV therapy? Use clean technique for dressing changes After cleansing the skin, dab dry with a sterile gauze pad Change the IV tubing every 12 hours Palpate the insertion site daily through the intact dressing Palpate catheter insertion site for tenderness daily through the intact dressing. Perform hand hygiene before and after palpating, inserting, replacing, or dressing any intravascular device. Maintain use of sterile dressings. Replace IV tubing no more frequently than at 72 hour intervals unless clinically indicated. Allow site to air-dry before proceeding with procedure. The patient has received a total of 7 units of blood over the last 24 hours. The nurse assesses the patient’s laboratory test results in the morning. Which of the following would be an expected complication? Hypokalemia Iron deficiency Hypercalcemia Hypocalcemia Blood that is preserved with citrate phosphate dextrose (CPD) contains a high concentration of citrate ions. The excess citrate may combine with the ionized calcium in the recipient’s blood, resulting in transient low ionized calcium levels. Although ionized calcium deficiency resulting from blood transfusions is rare, it is more likely to occur in young children, older adults, and patients with osteoporosis. When blood is stored, there is continual destruction of RBCs, which releases potassium from the cells into the plasma. If blood is transfused rapidly, transient hyperkalemia may occur before the potassium is reabsorbed. Patients receiving multiple transfusions should be assessed for iron overload. The patient has received a total of 7 units of blood over the last 8 hours. The nurse assesses the patient’s laboratory test results. Which of the following would be an expected complication? Iron deficiency Hypokalemia Hypercalcemia Hyperkalemia When blood is stored, there is continual destruction of RBCs, which releases potassium from the cells into the plasma. If blood is transfused rapidly, transient hyperkalemia may occur before the potassium is reabsorbed. Blood that is preserved with citrate phosphate dextrose (CPD) contains a high concentration of citrate ions. The excess citrate may combine with the ionized calcium in the recipient’s blood, resulting in transient low ionized calcium levels. Patients receiving multiple transfusions should be assessed for iron overload. The patient is to receive 1 unit of packed RBCs. The nurse obtains the blood from the blood bank and returns to the unit to find that the patient has been taken to radiology for a CT scan and is expected to return in about an hour. What should the nurse do? Go to radiology and administer the blood Keep the blood refrigerated until the patient returns Return the blood to the blood bank Hang the blood in the patient’s room and start it when the patient returns Initiate the blood transfusion within 30 minutes from time of release from blood bank. If you cannot do this because the patient is in the bathroom or the physician has to be notified of an elevated temperature, immediately return the blood to the blood bank, and retrieve it when you can administer it. The nurse is caring for a patient diagnosed with severe dehydration. She notes that the patient’s albumin level is 4.0. What may this indicate? An acute nutritional deficiency A long-term nutritional deficiency The patient is in a compromised protein state The level may be falsely high In patients who are dehydrated or who have received infusions of albumin, fresh frozen plasma, or whole blood, serum albumin will have levels that appear normal. Normal serum albumin values are between 3.5 and 5.0 g/dL. Albumin is a useful test for monitoring long-term nutrition changes because normal values still may be found among patients who are malnourished. For nutritional analysis, values between 2.8 and 3.5 g/dL indicate compromised protein status. Normal serum albumin values are between 3.5 and 5.0 g/dL. The nurse determines that a nasogastric (NG) tube needs irrigation when she: Does not encounter resistance when aspirating the residual Obtains more than 200 mL of residual volume Obtains a reduced volume of thick secretions Obtains a small amount of thin watery residual Thick secretions and a reduced volume of secretions indicate need to irrigate tube. Excess volume of secretions (more than 200 mL) indicates delayed gastric emptying. Irrigating the NG tube will not help. Thick secretions and a reduced volume of secretions indicate need to irrigate tube. Note ease with which tube feeding infuses through tubing. Failure of formula to infuse as desired may indicate developing obstruction. The nurse is initiating a continuous tube feeding for a patient who has a gastrostomy tube. Which of the following procedures indicates proper practice? Change the bag every 24 hours Allow the container to empty gradually over 60 minutes Increase the rate of administration quickly Do not use water to flush the tube Rinse bag and tubing with warm water whenever feedings are interrupted. Use a new administration set every 24 hours. Allowing the container to empty over 30 to 60 minutes is the method used for intermittent administration of tube feeding. Administer water via feeding tube as ordered or between feedings. Provides patient with source of water to help maintain fluid and electrolyte balance. Clears tubing of formula. Advance rate of concentration of tube feeding gradually. Helps to prevent diarrhea and gastric intolerance to formula. The nurse determines that the patient may have fluid overload as a result of assessing: Increased urine specific gravity Increased skin temperature Oliguria Distended neck veins Cardiovascular signs of fluid volume excess include bounding pulse rate, blood pressure normal with or without orthostatic changes, third heart sound (S3), and distended neck veins. Oliguria is a renal sign of fluid volume deficit. Increased skin temperature is a sign of fluid volume deficit. Increased urine specific gravity is a renal sign of fluid volume deficit. The nurse is caring for a patient who had a colostomy placed 5 days earlier. The nurse notes that the stoma is red and moist. What should the nurse do? Change the appliance pouch Notify the physician immediately Apply pressure Note the condition of the stoma in her note The stoma should be red or pink and moist. If it is gray, purple, or black, report this to the charge nurse or physician. Applying pressure is used to control active bleeding. The information given in the question does not indicate that there is a need to change the appliance at this time. When assessing the patient with a noncontinent urinary diversion, the nurse finds that the urine has mucous shreds. What should the nurse do first? Note the characteristics of the urine in her notes Instruct patient to consume less water Cleanse the stoma with soap and water Culture any drainage Mucous shreds are normal when urine flows through an intestinal segment. Obtain urine specimen for culture and sensitivity to test for possible infection when ordered by the physician if urine output is less than 30 mL/hour or urine has a foul odor. Teach patients the significance and importance of drinking 1.5 to 2 quarts of fluid daily to prevent urinary tract infection. Avoid soap; it leaves residue on skin, which interferes with pouch adhesion. The nurse is caring for a patient who has a urinary diversion. She notices that the patient has a temperature of 102° F and foul-smelling urine. What should the nurse do next? Catheterize the patient to obtain a sterile urine specimen Notify the physician Obtain a urine culture from the patient’s pouch Realize that these are normal findings Obtain physician’s order for catheterization. Although the nurse realizes the need for catheterization, it is an invasive procedure, and an invasive procedure requires a physician’s order. Obtaining a specimen of urine in a pouch does not provide an accurate finding because of the likely risk of contamination by microorganisms. Some mucus in urine is expected, but any blood in the urine, excessively cloudy urine, chills, fever (101° F or higher), or back (flank) pain should be reported to the physician. Currently, it is estimated that surgical site infections account for what percentage of hospital-acquired infections? 10 to 20 22 to 40 45 to 70 75 to 100 The Centers for Disease Control and Prevention’s (CDC) National Nosocomial Infections Surveillance (NNIS) system reports that surgical site infections (SSIs) account for 22% of hospital-acquired infections. Current research indicates that 40% of hospital-acquired infections are surgical site infections. What is the effect of the presence of hyperglycemia in the immediate postoperative period? Increases the risk for infection in the diabetic patient only Decreases the risk for surgical site infection Has no effect on the body’s ability to fight infection Increases the risk for infection in diabetic and nondiabetic patients The presence of hyperglycemia in the immediate postoperative period increases the risk for infection in both diabetic and nondiabetic patients. The higher the serum glucose, the greater is the potential for infection in both patient groups. Hyperglycemia has been shown to inhibit the body’s ability to fight infection. Immediate postoperative glucose control also has been correlated with a reduction in surgical infection. When is healing by primary intention expected? When the wound is left open and is allowed to heal When a surgical wound is left open for 3 to 5 days When connective tissue development is evident When the edges of a clean incision remain close together Healing by primary intention occurs when the edges of a clean surgical incision remain close together. The wound heals quickly, and tissue loss is minimal or absent. The skin cells quickly regenerate, and the capillary walls stretch across under the suture line to form a smooth surface as they join. Wounds that are left open and are allowed to heal by scar formation are classified as healing by secondary intention. Connective tissue development is evident during healing by secondary intention. Healing by tertiary intention occurs when surgical wounds are not closed immediately but are left open for 3 to 5 days to allow edema or infection to diminish. What should the nurse do when removing intermittent sutures? Snip the suture as close to the knot as possible Pull up the knot to apply as much tension as possible Snip the suture as close to the skin as possible Snip both sides of the suture before removing Snip suture as close to the skin as possible at end distal to the knot. Never snip both ends of suture; there will be no way to remove the part of the suture situated below the surface. Grasp knot of suture with forceps, and gently pull up knot while slipping tip of scissors under suture near skin. The nurse is caring for a patient who has a negative-pressure dressing. The nurse realizes that initially the dressing should be: Changed every shift Changed daily Changed every 8 hours Intact for 22 of 24 hours To optimize wound healing, the negative pressure of a traditional negative-pressure wound therapy (NPWT) unit is maintained for 22 of 24 hours per day. As the wound heals, the settings may change. Once NPWT is initiated, it must remain intact for 22 of 24 hours. The schedule for changing NPWT dressings varies. An infected wound may need a dressing change every 24 hours, whereas a clean wound can be changed 3 times a week. How does a nurse categorize for documentation exudate that is clear and watery? Sanguineous Purulent Serous Serosanguineous Serous drainage is a clear, watery plasma. Purulent drainage is a thick yellow, green, or brown drainage. Sanguineous drainage indicates fresh bleeding. Serosanguineous drainage is a pale drainage that is more watery than sanguineous drainage. Which of the following would require using caution in applying cold therapy? Chronic pain Sprains Joint trauma Circulatory insufficiency Conditions that require caution with cold therapy include circulatory insufficiency, cold allergy, and advanced diabetes. Cold therapy is used immediately after direct trauma such as sprain, strains, fractures, or muscle spasms; after superficial lacerations or puncture wounds; after minor burns; with chronic pain of arthritis and joint trauma; with delayed-onset muscle soreness; and with inflammation. The nurse is visiting an elderly patient who lives with his wife and daughter. He has several daily medications, including antihypertensives, antiarrhythmics, diuretics, and pain medication. The patient’s wife states that he takes all of the pills in the morning and some at night. The nurse should examine the pills and suggest which of the following? Increase the different types of pain medication to prevent addiction to one Administer at bedtime medications that are likely to cause confusion Take the diuretics at bedtime Take the antiarrhythmics and antihypertensives together in the morning to prevent hypotension during sleep Administer at bedtime medications that are likely to cause confusion to reduce the risk for confusion during waking hours, which contributes to disorientation and the risk for falling. However, do not recommend this if the patient has nocturia. Space antihypertensives and antiarrhythmics at different times to minimize side effects. Have diuretics taken early in the day and not at night, so that the diuretic effect occurs during the day while the patient is awake. Reduce the number of pain medications used when possible. Drugs create sedative effects, increasing the risk for falls. The patient’s caregiver is checking the patient’s nasogastric (NG) tube for gastric residual before proceeding with the patient’s next feeding. The patient aspirates 250 mL of residual for the second hour in a row. The caregiver held the tube feeding within the last hour. What should the caregiver do now? Contact the health care provider Hold the feeding again Proceed with the feeding Give half of the feeding and see how the patient tolerates it If aspirates remain at more than 200 mL after an hour, instruct patient or caregiver to contact home care nurse or health care provider. Information that should be provided to the caregiver of a patient with a nasogastric (NG) tube includes: Aspirating every 4 hours when receiving continuous drip feedings Keeping unused formula at room temperature Providing half of the feeding if the residual exceeds 250 mL Keeping the head of the bed lowered for feedings Patient and caregivers need to document intake and output (I&O), daily weights, amount of gastric fluid aspirated before each feeding (or every 4 hours if receiving continuous feeding), date and time of feedings, amount and type of formula, any additives, and date and time administration sets are changed. Instruct patient or caregiver that the patient should sit up in a chair or have the head of the bed elevated at least 30 to 45 degrees while receiving feedings or medications or when tube is flushed. Refrigerate unused formula. If gastric aspirates are greater than or equal to 200 mL, instruct patient or caregiver to return gastric contents and delay tube feeding for 1 hour. If aspirates remain greater than or equal to 200 mL after an hour, instruct patient or caregiver to contact home health nurse or health care provider. During a sputum collection, the patient becomes hypoxic. What action should the nurse take? Stop the procedure and provide oxygen, if ordered Continue to complete the procedure quickly Suction the patient thoroughly Have the patient lie down and take deep breaths before continuing with the specimen collection If the patient becomes hypoxic, discontinue the procedure until stable and provide oxygen therapy as needed, if ordered. Suctioning can decrease usable oxygen to the patient. Which action should a nurse take following a procedure requiring intravenous moderate sedation? Take vital signs every 30 minutes until stable Monitor airway patency and vital signs every 5 minutes for 30 minutes Take vital signs every 15 minutes for the next 2 hours Report a Ramsay sedation score that is less than 3 to the physician After procedure: monitor airway patency, vital signs, SpO2, pain score, level of consciousness, every 5 minutes for at least 30 minutes, then every 15 minutes for an hour and then every 30 minutes until the patient meets the discharge criteria on the agency’s designated scoring system. Report only a Ramsay sedation score higher than 3 to the physician. A nurse is alert to a possible delayed reaction to the dye injected during an angiography. For which response should she monitor the patient? Dyspnea. Thirst. Pallor. Numbness and tingling. Assess patient for possible delayed reaction to iodine dye - dyspnea, hives, tachycardia, and rash. Reaction occurs up to 6 hours after injection of dye. Thirst, by itself, is not a major warning sign of reaction to the dye. Pallor, by itself, is not a major warning sign of reaction to the dye. Patient’s report of any feelings of pain, dyspnea, numbness or tingling or other untoward symptoms may indicate cardiac complications or procedure site complications, but not of reaction to the dye. Then explaining about a lumbar puncture, a nurse informs a patient that during the procedure he or she will be asked to: Breathe deeply during the needle insertion Change position Correct Answer Remain very still Cough during the fluid aspiration Emphasize the importance of remaining immobile during procedure to prevent trauma, especially with the lumbar puncture because sudden movement is a risk for spinal cord nerve root damage. Also, instruct patient not to cough, sneeze, or breathe deeply during the procedures because these actions increase the risk for needle displacement and damage of other structures. When explaining what to expect during a bronchoscopy, a nurse informs a patient that: The tube will be passed through the nose. Nothing will be given by mouth for 2 to 3 hours prior. No food or fluid will be provided until the gag reflex returns. An anesthetic solution will be swallowed. Do not allow patient to eat or drink until the tracheobronchial anesthesia has worn off and the gag reflex has returned, usually 2 hours. Instruct patient not to swallow local anesthetic. The bronchoscope is introduced into the mouth, to the pharynx, to pass through the glottis. Patient should have taken nothing by mouth for at least 8 hours before a bronchoscopy. For an upper gastrointestinal endoscopy, a nurse should: Suction the patient every 5 minutes. Place the patient in high-Fowler’s position. Provide fluids immediately after the test is finished. Remove the patient’s dentures. Remove patient’s dentures and other dental appliances to prevent dislodgement of dental structures during intubation phase. Position tip of cannula for easy access in the patient’s mouth to drain oral secretions; suction as needed. Help the patient to maintain left lateral Sims’ position. Instruct the patient not to eat or drink after the procedure until the gag reflex returns, which is usually about 2 hours after the procedure. Quiz Score: 7,400 out of 8,000 Submission Details: [Show More]
Last updated: 3 years ago
Preview 1 out of 47 pages
Buy this document to get the full access instantly
Instant Download Access after purchase
Buy NowInstant download
We Accept:

Can't find what you want? Try our AI powered Search
Connected school, study & course
About the document
Uploaded On
Apr 01, 2021
Number of pages
47
Written in
All
This document has been written for:
Uploaded
Apr 01, 2021
Downloads
0
Views
136
Scholarfriends.com Online Platform by Browsegrades Inc. 651N South Broad St, Middletown DE. United States.
We're available through e-mail, Twitter, Facebook, and live chat.
FAQ
Questions? Leave a message!
Copyright © Scholarfriends · High quality services·



.png)