isease
Risk
Subjective Finding
Objective Findings
Diagnostics
Treatment
Education
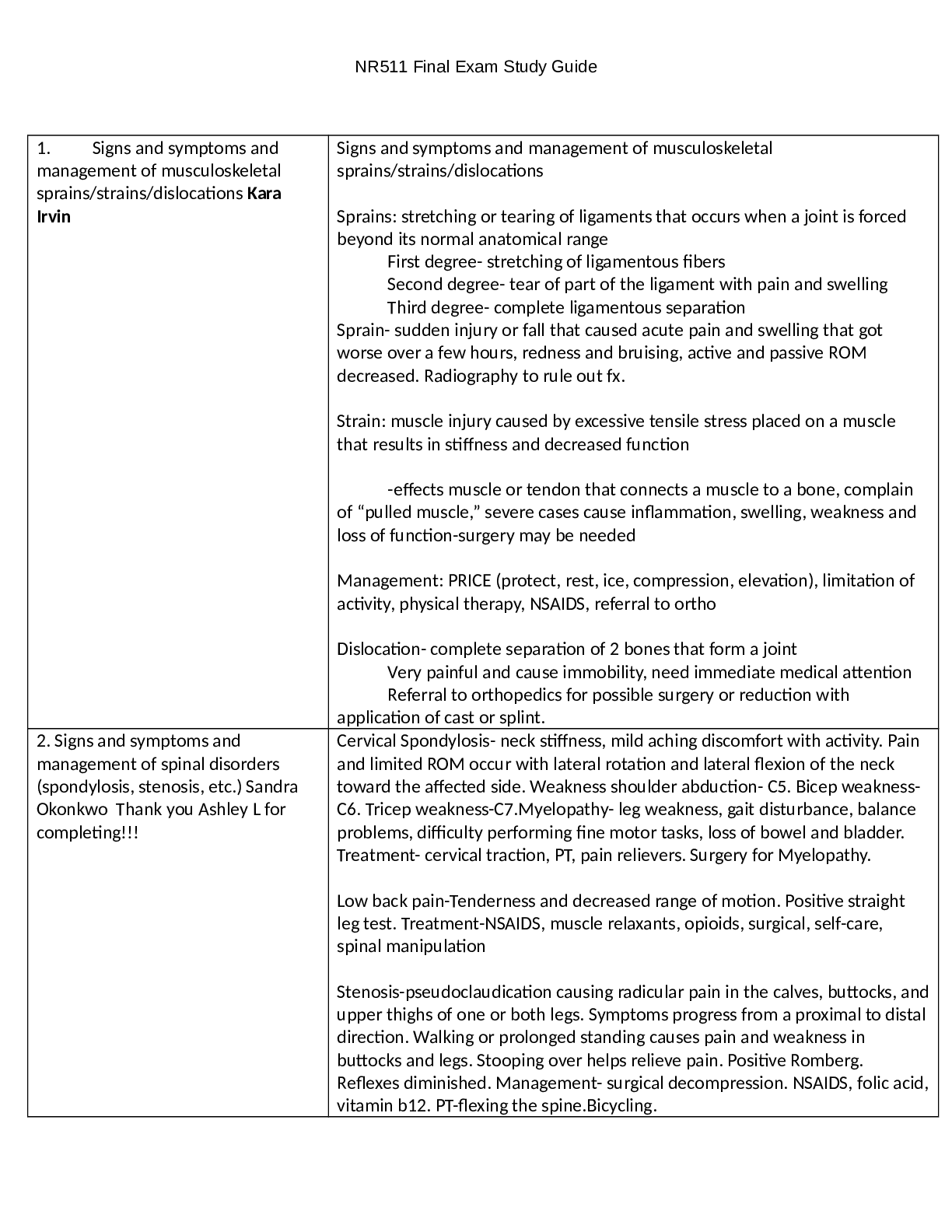
GI DISORDERS
Appendicitis
-Most common between 10-30yrs; but can occur at any age; rare in infants and older adults
-men more at
...
isease
Risk
Subjective Finding
Objective Findings
Diagnostics
Treatment
Education
GI DISORDERS
Appendicitis
-Most common between 10-30yrs; but can occur at any age; rare in infants and older adults
-men more at risk
- Diets low in fiber, high in fat, refined sugars, & other carbs at increased risk.
- Obstruction of appendix is cause of majority of appendicitis - contributing factors: Intra-abdominal tumors, positive family hx
- Recent roundworm infection or viral GI infection
-Dx made clinically, based primarily on H&P exam
- Classic presentation includes acute onset of mild to severe colicky, epigastric, or
periumbilical pain - Pain is vague at first then localizes within 24hrs to RLQ
- Pain exacerbated by walking\coughing
- Men may feel radiated pain in testes - Abd muscle rigidity, N\V, anorexia
- Mildly elevated temp 99-100F common
- If RLQ accompanied by shaking chills, perforation should be suspected
- Older adults may present with weakness, anorexia, abd distention, mild pain leading to delayed dx and increased morbidity.
-May have HTN\tachy proportional to
pain\symptoms -When lying flat, may flex R knee to relieve tension in abd muscle -Pain with palpation in abd, diffuse in early stages. Localized to RLQ later
-Positive for rebound pain; ask pt to cough to localize pain location
-Sudden cessation of pain means perforation and is ER
-Labs are not diagnostic and nonspecific -Women should have urine human chorionic gonadotrophin to r\o ectopic pregnancy - +Rovsing’s Sign- deep palpation & release in LLQ causes rebound pain in RLQ - +Psoas Sign- lift R leg against gentle pressure causes pain - +Obturator Sign- flex R hip & knee and slowly rotate internally causes pain - +McBurney’s Sign- pain with pressure applied to point between umbilicus & ilium
- x-ray\CT helpful when paired with positive H&P findings
-Surgical; preoperative care, NPO, correction of fluid\electrolyte imbalances
-Avoid narcotics -Atb with 3rd gen cephalosporin;
Ex:ampicillin, gentamycin, flagyl
-F\U with surgeon -Ambulation after surgery
-Adv diet when bowel sounds return -Return to hosp with s\s of infection -Avoid heavy lifting for at least 2 wks
Celiac disease ** (autoimmune disorder caused by an immunologic response to gluten)
Mostly diagnosed in adulthood.
A family member with celiac disease or dermatitis
herpetiformis Type 1 diabetes
Many asymptomatic. May complain of diarrhea,gas, dyspepsia, wt loss. Atypical symptoms: fatigue,
bone or joint pain, arthritis, osteoporosis, or
Muscle wasting (anemia), reduces subcutaneous fat, ataxia, & peripheral neuropathy (vitamin B12 deficiencies) osteoporosis or osteopenia (bone loss)
Serologic testing for anti-tTG IgA antibody
Total IgA (2% of pts have IgA deficiency and will falsely test negative)
duodenal biopsies
lifelong adherence to a strict gluten-free diet.
Referral to a dietician to help.
Some pts may need treatment with immunomodulating
teaching related to gluten free diet.
[Show More]