Health Care > CASE STUDY > Case Study by Sara Martinez, Chamberlain College of Nursing, NR 601 Primary Care of the Maturing and (All)
Case Study by Sara Martinez, Chamberlain College of Nursing, NR 601 Primary Care of the Maturing and Aged Family Primary Diagnosis Diabetes Mellitus Type 2 (DM) (E11.9)
Document Content and Description Below
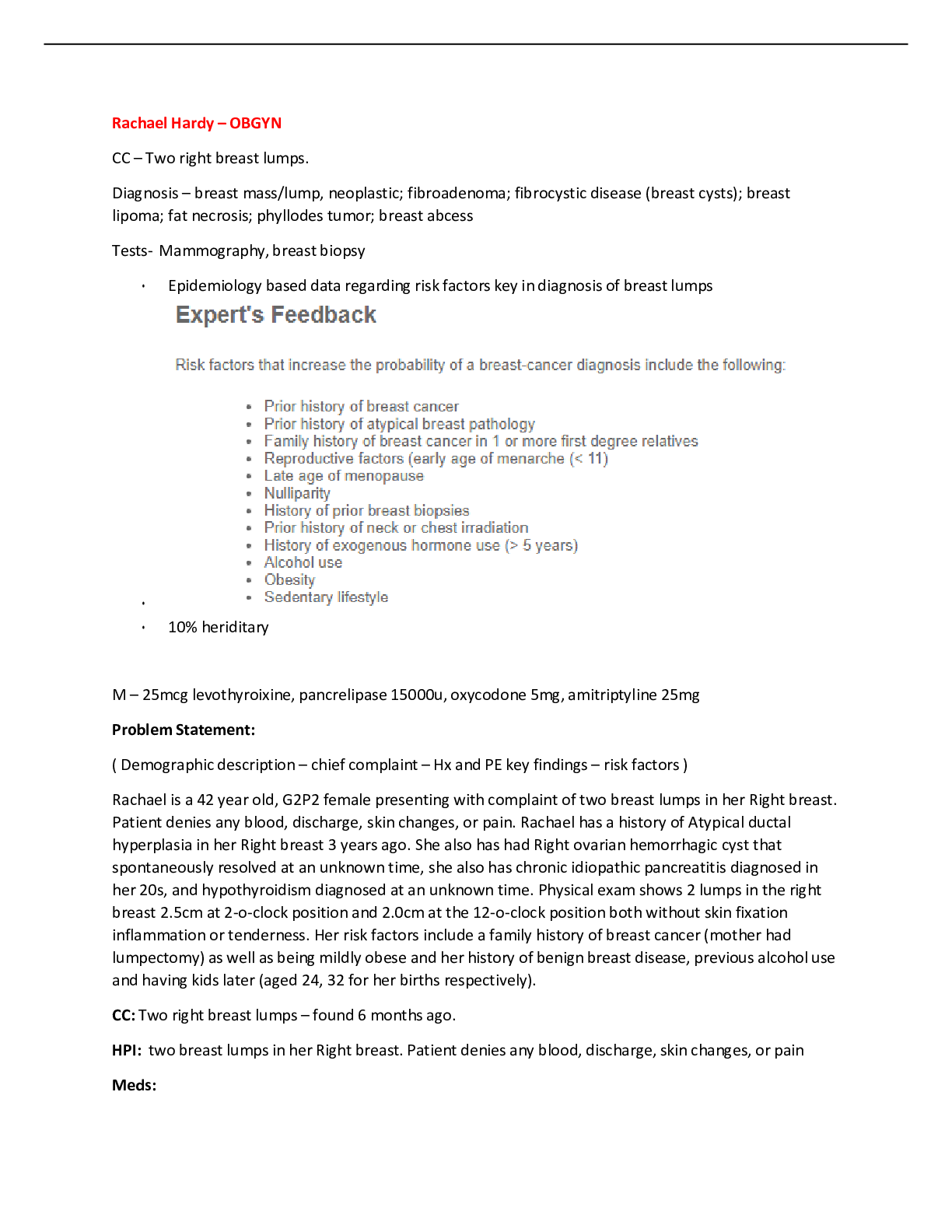
Case Study Sara Martinez Chamberlain College of Nursing NR 601: Primary Care of the Maturing and Aged Family The purpose of this case study is to present Mrs. R., a 56- year old Hispanic fem... ale, follow up visit in the clinic with the chief complaint of fatigue and weight gain. The onset of Mrs. R’s symptoms began three months ago. She reports going to the gym and exercising twice a week, at the gym she walks on the treadmill for 30 minutes in the effort of losing weight in which she has not lost any weight. The purpose of this case study is the analysis of objective and subjective findings in order to diagnose and construct a plan of management of Mrs. R’s chief complaint. To include the National Diabetes Guidelines which will be applied to the patient’s management plan. This paper will comprise of primary diagnosis, secondary diagnosis and differential diagnosis for Mrs. R, along with a plan for management and treatment of the primary diagnosis, secondary diagnosis, and the differential diagnosis. Involving diagnostics, medications, education, referrals and follow-up care. Furthermore, this paper will include the discussion of medication cost of all prescribed and ( OTC) over- the- counter medications. Assessment The following information provided by Mrs. R., reports does not understand why she has weight gain despite working out twice a week on the treadmill for 30 minutes each time, fatigue, increased thirst, hunger, and urination. She is 5’2.5, and 165 pounds according to the Center for Disease Control and Prevention BMI calculator (CDC) (2015), Mrs. R’s BMI is 29.7indicating she is overweight for her height of 5’2.5. The outcome of her urinalysis indicated 1+ glucose and a small amount of protein. Fasting glucose 126 mg/dl and HgbA1C 6.9%, according to the American Diabetes Association (ADA) (2018), meets the criteria for a primary diagnosis of diabetes. Lipid panel reveals her secondary diagnosis of hyperlipidemia and her raised cholesterol indicates the probability of increased risk for a stroke and cardiovascular disease (AACE, 2017). Differential diagnosis obesity due to her BMI of 29.7 for her weight and height her BMI should be 18.5 to 24.9 according to the Center for Disease Control and Prevention BMI calculator (CDC) (2015). Primary Diagnosis Diabetes Mellitus Type 2 (DM) (E11.9) Type 2 Diabetes is identified as adult-onset diabetes as specified by hyperglycemia, insulin deficiency and insulin resistance leading to the increased risk for developing vascular and neurologic complications (American Diabetes Association, 2018). Goroll (2014) states an insufficient amount of insulin that is expelled by the pancreas in order to meet the needs of a metabolic state resulting in hyperglycemia; this disease becomes evident as aging occurs in most cases. Indications of Type 2 Diabetes involve fatigue as the prime indicator. An indication of Type 2 Diabetes is polyuria, polydipsia, polyphagia and weight increase (Goroll, 2014). Pertinent positives for Mrs. R involve thirsty all the time (polydipsia), hungry all the time ( polyphagia), increase in urination particularly during the day (polyuria), increase in fatigue, inability to lose weight despite exercise, overweight, the patient's age and of Hispanic ethnicity. The lab work for her contains Hemoglobin A1C as 6.9%, fasting blood glucose as 126, small amount of protein with 1+ glucose and elevated cholesterol in which reveal a diagnosis of Diabetes Mellitus Type 2. Complications of Diabetes Type 2 such as renal failure, cardiovascular and peripheral vascular disease, glaucoma and blindness (Pippitt, Li, and Gurgle, 2016). Pertinent negatives no family history of Diabetes, no history of tobacco use, usually walk on the treadmill twice a week for 30 min. No personal history of Diabetes, or hyperlipidemia. No laboratory evidence of kidney disease according to the National Kidney Foundation (2018), for her age average GFR should be > or = to 90 both GFR of est. The non-AA result was 99 ml/min/1.73m and AA- 101 ml/min/1.73 placing her in the low-risk category no Chronic Kidney Disease. [Show More]
Last updated: 2 years ago
Preview 1 out of 21 pages
 (E11.png)
Buy this document to get the full access instantly
Instant Download Access after purchase
Buy NowInstant download
We Accept:

Reviews( 0 )
$14.00
Can't find what you want? Try our AI powered Search
Document information
Connected school, study & course
About the document
Uploaded On
Jun 13, 2021
Number of pages
21
Written in

Additional information
This document has been written for:
Uploaded
Jun 13, 2021
Downloads
0
Views
68
 (A Graded) Latest Questions and Complete Solutions.png)
, Latest Questions and Answers with Explanations, All Correct Study Guide, Download to Score A.png)
 Pneumonia Chronic Obstructive Pulmonary Disease Clinical Reasoning Case Study Medical surgical (NUR 201) Pneumonia-COPD case study solutions.png)


 – Chest Pain Complete Latest Solutions.png)







 – Chamberlain College of Nursing.png)