NR 507 Week 1 Assignment: Immune Response (Edapt) | SOLVED
Document Content and Description Below
NR507 Advanced Pathophysiology Chapter 9: Alterations in Immunity and Inflammation 2 NR507 Advanced Pathophysiology Week 1 Chapter 9: Alterations in Immunity and Inflammation I. Inappropriate... immune responses may be: A. Exaggerated against environmental antigens B. Misdirected against the host’s own cells C. Directed against beneficial foreign tissues D. Insufficient to protect the host II. Hypersensitivity: Allergy, Autoimmunity, and Alloimmunity Table 9.3 Immunologic Mechanisms of Tissue Destruction Type Name Rate of Development Antibody Cells Involved Complement Examples I IgE-mediated Immediate IgE Mast No Seasonal Allergic Rhinitis II Tissue-Specific Immediate IgG, IgM Macrophages Frequently Autoimmune Diseases III Immune complex Immediate IgG, IgM Neutrophils Yes SLE IV Cell-mediated Delayed None Lymphocytes, macrophages No Poison Ivy A. Hypersensitivity: altered immunologic response to an antigen that results in disease or damage to the host. B. Autoimmune: disturbance in immunologic tolerance of self-antigens C. Autoimmune Diseases: when immune system attacks T cells D. Alloimmunity: immune system of 1 individual attacks another individual’s 1. Think transplant or fetuses E. Immunologic Homeostasis: steady state of tolerance to self-antigens. F. Most hypersensitivities occur because: 1. An original “insult” that alters immunologic homeostasis 2. The individual’s genetic makeup 3. An immunologic process that causes the symptoms of the disease G. Mechanisms of Hypersensitivity 1. Hypersensitivity requires sensitization which occurs when there’s enough antibodies or T cells available to cause a reaction 2. Anaphylaxis: itching erythema, headache, vomiting, difficulty breathing, etc 3. Type 1: IgE-Mediated Hypersensitivity Reactions a) Mediated b antigen-specific IgE and products of tissue mast cells b) Most potent mediator is histamine (1) Contracts bronchial smooth muscles, increases edema, and causes vasodilation from the H1 (2) Mast cells cause synthesis of bioactive lipid-derived mediators 4. Type II: Tissue-Specific Hypersensitivity Reactions: characterized by specific cell/ tissue being target of immune response a) General Mechanisms (1) Cell destroyed by antibody and activation of complement cascade (2) Antibody may cause cell destruction through phagocytosis (3) Antibody and complement may attract neutrophils (4) Antibody-dependent cell mediated cytotoxicity 5. Type III: Immune Complex-Mediated Hypersensivity Reactions a) Mechanism of Type 3 Hypersensitivity (1) Most are caused by antigen-antibody complexes that are formed in the circulation and deposited later in vessel walls or extravascular tissues (2) Bind to the soluble antigen tat was released in to the blood or body fluids, and the complex is then deposited into the tissues b) Immune Complex Disease (1) Serum Sickness: caused by the formation of immune complexes in the blood and their subsequent generalized deposition in target tissues (2) Arthus Reaction: localized immune complex-mediated inflammatory response. 6. Type IV: Cell-Mediated Hypersensitivity Reactions a) Mediated by the T lymphocytes and don’t involve antibodies b) Clinical examples include graft rejection and allergic reactions from contact of a substance H. Antigenic Targets of Hypersensitivity Reactions 1. Allergy a) Typical allergens that induce type 1 hypersensitivity include pollens, molds and fungi, foods, animals, cigarettes, and anything encountered in the environment. b) Type II and type III: drugs and soluble agents c) Type IV: plant based d) Genetic Predisposition: atopic—tend to produce higher quantities of IgE 2. Clinical Symptoms of Type 1 Allergies Table 9.4 Causes of Clinical Manifestations of Allergy Typical Allergen Mechanism of Hypersensitivity Clinical Manifestations Ingestants Foods Type 1 Gastrointestinal allergy Drugs Types 1, 2, 3 Urticaria, immediate drug reaction, hemolytic anemia, serum sickness Inhalants Pollens, dust, mold Type 1 Allergic rhinitis, brachial asthma Aspergillus fumigatus Types 1, 3 Allergic bronchopulmonary aspergillosis Thermophilic actinomycetes Types 3,4 Extrinsic allergic alveolitis Injectants Drugs Types 1, 2, 3 Immediate drug reaction, hemolytic anemia, serum sickness Bee Venom Type 1 Anaphylaxis Vaccines Type 3 Localized Arthus reaction Serum Types 1, 3 Anaphylaxis, serum sickness Contactants Poison ivy, metals Type 4 Contact dermatitis a) Mostly due to histamine b) Avoidance is the best method! 3. Allergic Disease: Bee Sting Allergy a) Edema at site, hives itching, and swelling distal to site b) Severe: GI issues or respiratory c) Antihistamines have little effect because H1 has already caused severe bronchial smooth muscle contraction d) Use Epipen 4. Tests of IgE-Mediated Allergy a) Food challenges: small bites of food b) Desensitization (1) Minute quantities fo allergens are injected in increasing doses over prolonged periods (2) Blocking antibodies compete so the allergen is unable to bind to IgE on mast cells c) Type IV Allergic Hypersensitivies (1) Primary result is contact dermatitis confined to area of contact d) Types II and III (1) Typically with IgG or IgM responses (2) Usually allergic reaction to drugs 5. Autoimmunity: originate from coincidence of an initiating even in a genetically predisposed individual leading to an autoimmune mechanism that affects specific target tissues or cells a) Genetic Factors (1) Most are familial b) Breakdown of tolerance (1) Central tolerance develops in humans during the embryonic period as autoreactive lymphocytes are either eliminated or suppressed in the primary typhoid organs during differentiation and proliferation of immature T or B cells (2) Peripheral tolerance is maintained in the secondary lymphoid organs through the action of T-regulatory lymphocytes or antigen-presenting dendritic cells (3) Detrimental Immune Response: (a) Sequestered Antigen: hidden in immunologically privileged sites (b) Infectious Disease: molecular mimicry (c) Neoantigen: happens that become immunogenic after binding to self- proteins (d) Forbidden Clone: lymphocytes reactive against self-antigen are prevented from maturing (e) Defective Peripheral Tolerance: controlled by a variety of cells (f) Silent Imitators 6. Alloimmunity: occurs when an individual’s immune system reacts against antigens on the tissues of other members of the same species a) Transient Neonatal Alloimmunity: when the fetus is rejected by the mother I. Autoimmune and Allimmune Diseases 1. Systemic Lupus Erythematosus: chronic, multisystem, inflammatory disease 2. The most characteristic autoantibodies produced in SLE are against nucleic acids 3. Who: women between 20-40 years old 4. Clinical Manifestations: arthritis, vasculitis, hematologic abnormalities, anemia, and cardiovascular disease 5. Develops slowly 6. The serial or simultaneous presence of at least four clinical findings indicate disease presence: a) Facial rash confined to the cheeks b) Discoid rash c) Photosensitivity d) Oral or nasopharyngeal ulcers e) Nonerosive arthritis f) Serositis g) Renal disorder h) Neurologic disorders i) Hematologic disorders j) Immunologic disorders k) Presence of ANA 7. Lab: Positive ANA screening, the antibody testing 8. Goals of Tx: control symptoms and prevent further damage 9. Tx: a) Mild—NSAIDs b) Steroids for active c) Antimalarial for stable d) Immunosuppressive for severe e) IVIg works well J. Transfusion Reactions—Alloimmune 1. ABO groups a) Isohemagglutinins: naturally occurring antibodies 2. Rh System: antigens only on RBCs a) Hemolytic disease of Newborn: Rh- moms with Rh+ babies K. Graft Rejections 1. MHC molecules are major targets of transplant rejection 2. Hyperacute: immediate and rare 3. Acute: within days to months 4. Chronic: long, slow organ failure III. Deficiencies in Immunity A. Immune deficiency: failure of mechanisms of self-defense B. Primary: caused by genetic anomaly C. Acquired: caused by disease D. Initial Clinical Presentation 1. Clinical hallmark is recurrent severe infections 2. Usually have 8+ purulent ear infections, 2+ sinus infections, 2+ pneumonias, recurrent abscess or fungal infections 3. Types of recurrent infections could indicate types of immune defect a) T-cell: viruses, fungi/yeasts, microorganisms b) B-cell: encapsulated bacteria, rubella E. Primary Immune Deficiencies F. Secondary Immune Deficiencies 1. 1 Normal Physiologic Conditions a) Pregnancy: decreased reactivity b) Newborn: immunologically immature c) Psychological Stress: increased incidence of infection with long periods of stress d) Physical trauma G. Evaluation and Care of those with Immune Deficiency 1. Caution with routine vaccines 2. GVHB 3. Labs 4. Replacement Therapies a) Gamma-Globulin: IVIg b) Transplant and Transfusion: stem cells, bone marrow c) Treatment with Soluble Immune modulators d) Gene: SCID cloned and inserted [Show More]
Last updated: 2 years ago
Preview 1 out of 5 pages

Buy this document to get the full access instantly
Instant Download Access after purchase
Buy NowInstant download
We Accept:

Reviews( 0 )
$10.50
Can't find what you want? Try our AI powered Search
Document information
Connected school, study & course
About the document
Uploaded On
Oct 20, 2022
Number of pages
5
Written in

Additional information
This document has been written for:
Uploaded
Oct 20, 2022
Downloads
0
Views
171


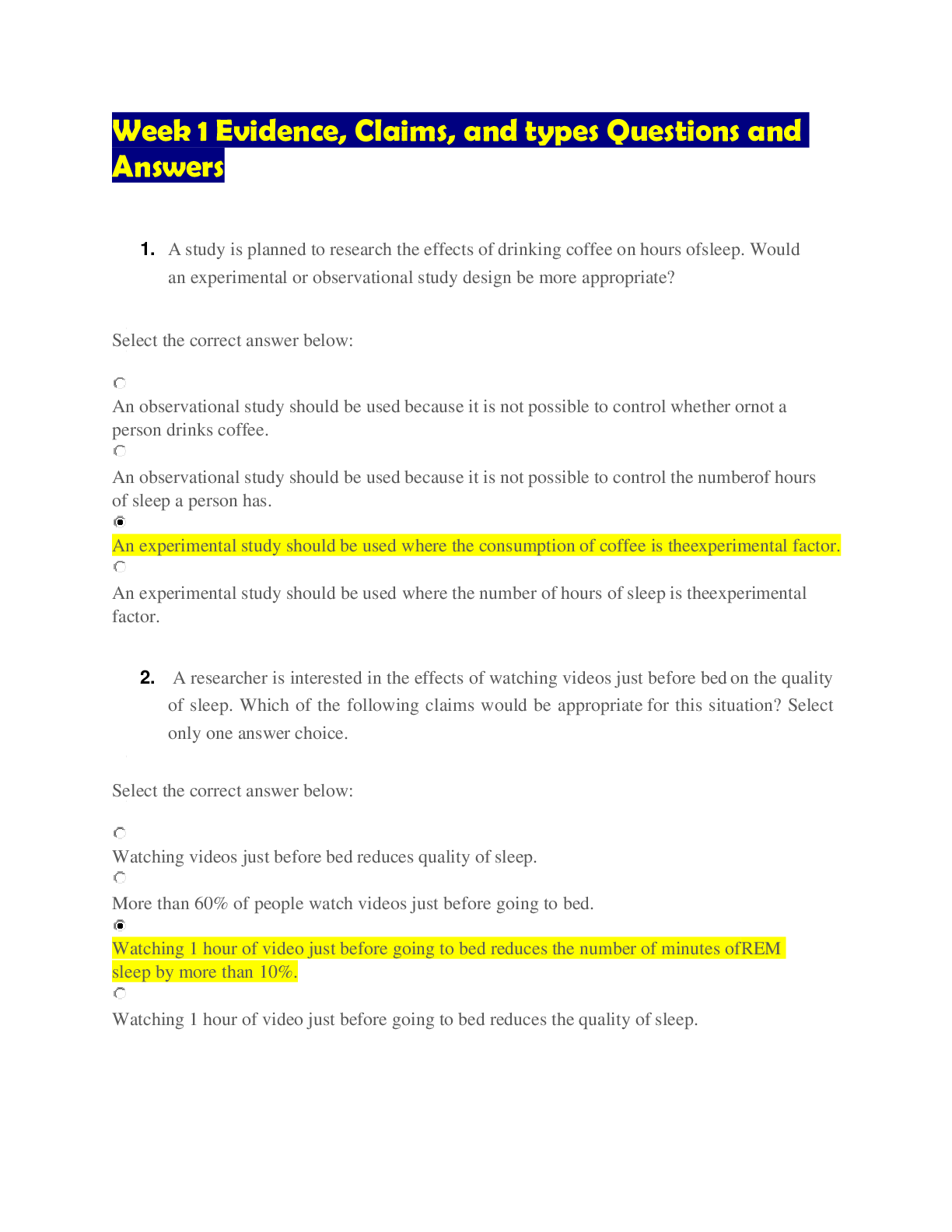
 Questions and Answers 100% VERIFIED.png)
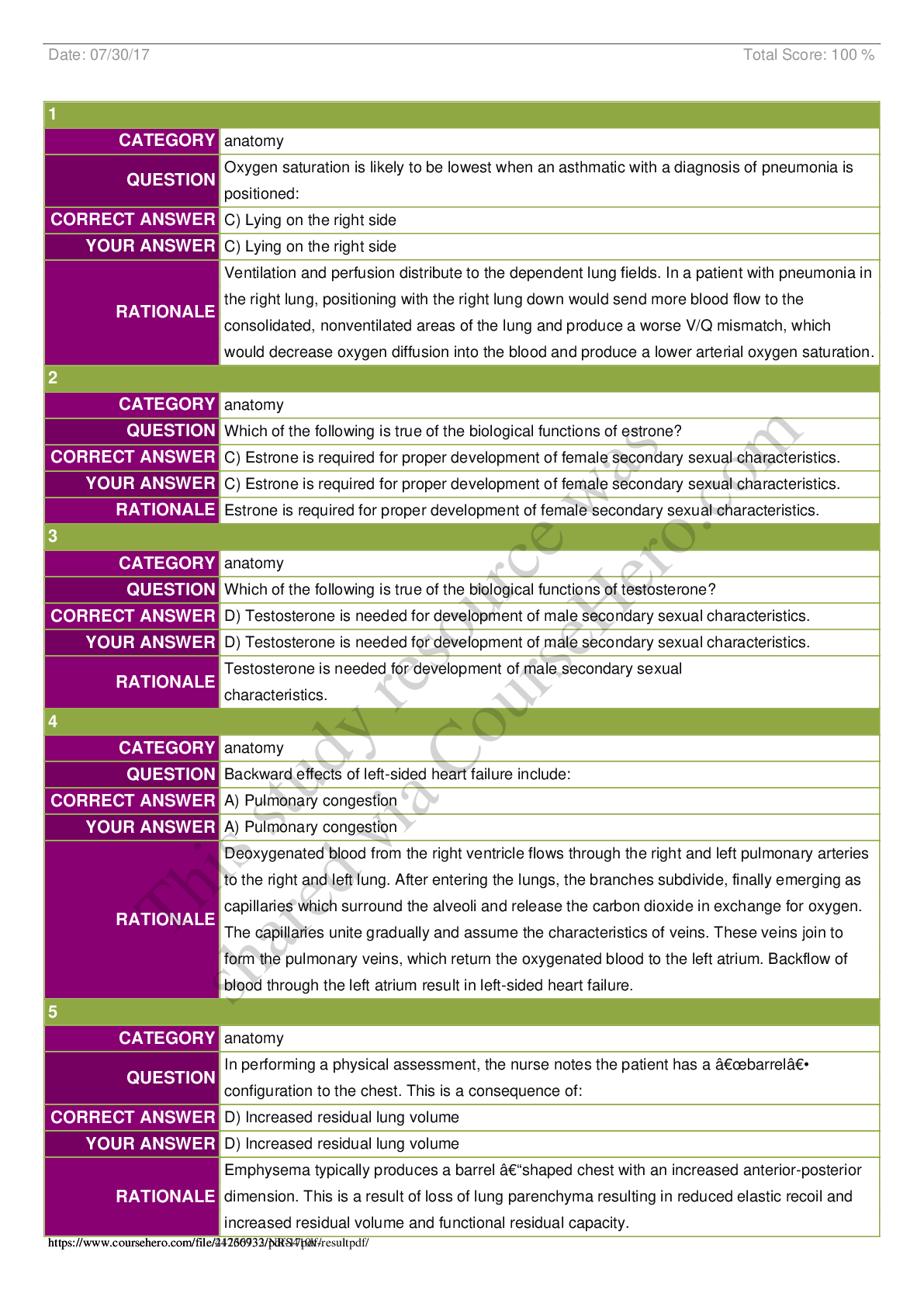
 Questions and Answers 100% correct Solutions.png)






.png)