OBSTETRICS
Physiology of Pregnancy:
PREGNANCY
CO input increases 30-50% (max 20-24 weeks) (mostly due to increase in stroke volume)
SVR and arterial bp decreases (likely due to increase in progesterone)
od
...
OBSTETRICS
Physiology of Pregnancy:
PREGNANCY
CO input increases 30-50% (max 20-24 weeks) (mostly due to increase in stroke volume)
SVR and arterial bp decreases (likely due to increase in progesterone)
odecrease in systolic blood pressure of 5 to 10 mm Hg and in diastolic blood pressure of 10 to 15 mm Hg that nadirs at week 24.
Increase tidal volume 30-40% and total lung capacity decrease by 5% due to diaphragm
Increased red blood cell mass
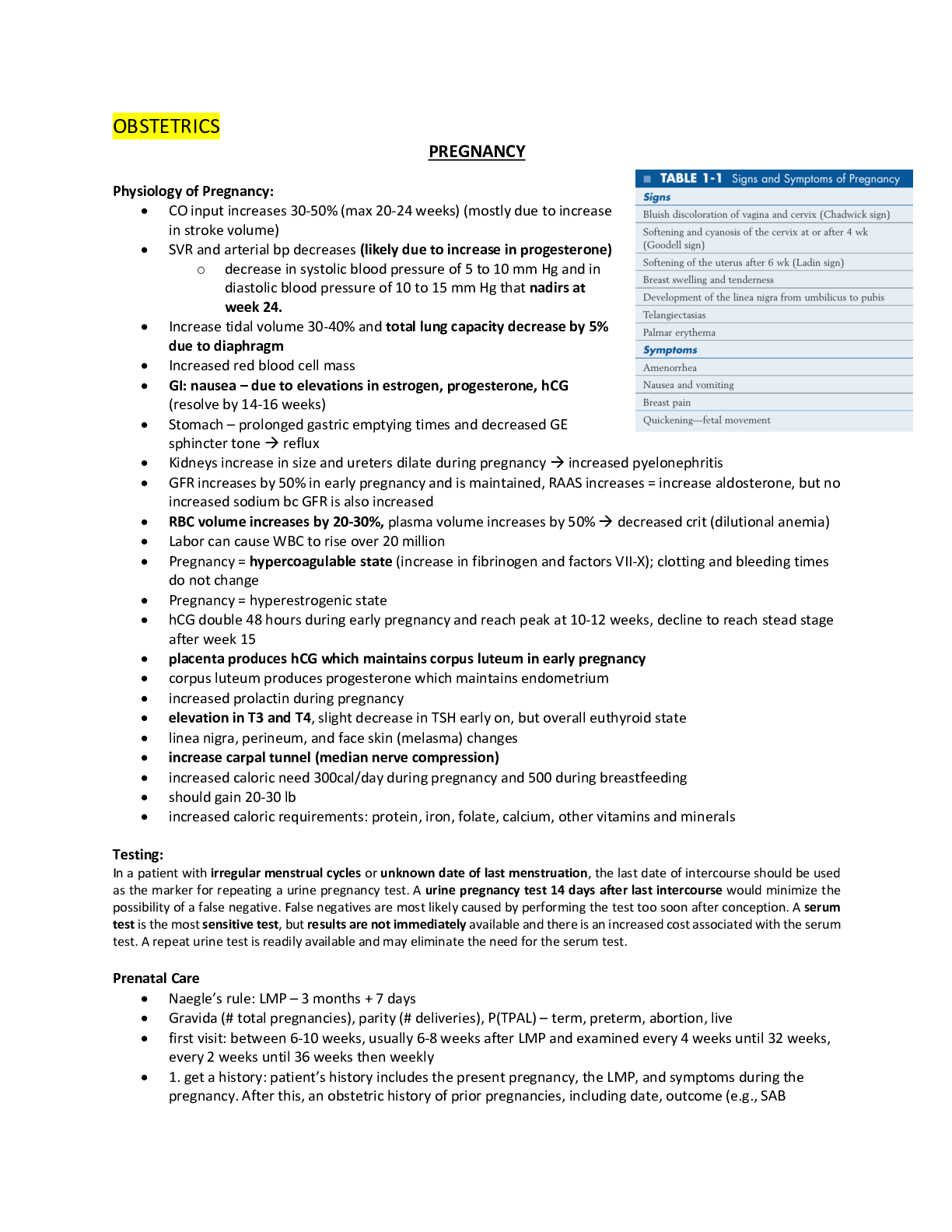
GI: nausea – due to elevations in estrogen, progesterone, hCG
(resolve by 14-16 weeks)
Stomach – prolonged gastric emptying times and decreased GE sphincter tone reflux
Kidneys increase in size and ureters dilate during pregnancy increased pyelonephritis
GFR increases by 50% in early pregnancy and is maintained, RAAS increases = increase aldosterone, but no increased sodium bc GFR is also increased
RBC volume increases by 20-30%, plasma volume increases by 50% decreased crit (dilutional anemia)
Labor can cause WBC to rise over 20 million
Pregnancy = hypercoagulable state (increase in fibrinogen and factors VII-X); clotting and bleeding times do not change
Pregnancy = hyperestrogenic state
hCG double 48 hours during early pregnancy and reach peak at 10-12 weeks, decline to reach stead stage after week 15
placenta produces hCG which maintains corpus luteum in early pregnancy
corpus luteum produces progesterone which maintains endometrium
increased prolactin during pregnancy
elevation in T3 and T4, slight decrease in TSH early on, but overall euthyroid state
linea nigra, perineum, and face skin (melasma) changes
increase carpal tunnel (median nerve compression)
increased caloric need 300cal/day during pregnancy and 500 during breastfeeding
should gain 20-30 lb
increased caloric requirements: protein, iron, folate, calcium, other vitamins and minerals
[Show More]



.png)
.png)



.png)
.png)