HPI: Ms. Jones is a pleasant 28-year-old
African American woman who presented to
the clinic with complaints of upper stomach
pain after eating. She noticed the pain about
a month ago. She states that she
experiences
...
HPI: Ms. Jones is a pleasant 28-year-old
African American woman who presented to
the clinic with complaints of upper stomach
pain after eating. She noticed the pain about
a month ago. She states that she
experiences pain daily, but notes it to be
worse 3-4 times per week. Pain is a 5/10
and is located in her upper stomach. She
describes it “kind of like heartburn” but
states that it can be sharper. She notes it to
increase with consumption of food and
specifically fast food and spicy food make
pain worse. She does notice that she has
increased burping after meals. She states
that time generally makes the pain better,
but notes that she does treat the pain “every
few days” with an over the counter antacid
with some relief.
Social History: She denies any specific
changes in her diet recently, but notes that
she has increased her water intake.
Breakfast is usually a muffin or pumpkin
bread, lunch is a sandwich with chips,
dinner is a homemade meal of a meat and
vegetable, snacks are French fries or
pretzels. She denies coffee intake, but does
drink diet cola on a regular basis. She
denies use of tobacco and illicit drugs. She
drinks alcohol occasionally, last was 2
weeks ago, and was 1 drink. She does not
exercise.
Review of Systems: General: Denies
changes in weight and general fatigue. She
denies fevers, chills, and night sweats. •
Cardiac: Denies a diagnosis of
hypertension, but states that she has been
told her blood pressure was high in the past.
She denies known history of murmurs,
dyspnea on exertion, orthopnea,
paroxysmal nocturnal dyspnea, or edema.
This study source was downloaded by 100000831988016 from CourseHero.com on 05-06-2022 05:36:07 GMT -05:00
https://www.coursehero.com/file/47999252/GI-Tina-Jones-documentationdocx/
• Respiratory: She denies shortness of
breath, wheezing, cough, sputum,
hemoptysis, pneumonia, bronchitis,
emphysema, tuberculosis. She has a history
of asthma, last hospitalization was age 16,
last chest XR was age 16. • Gastrointestinal:
States that in general her appetite is
unchanged, although she does note that
she will occasionally experience loss of
appetite in anticipation of the pain
associated with eating. Denies nausea,
vomiting, diarrhea, and constipation. Bowel
movements are daily and generally brown in
color. Denies any change in stool color,
consistency, or frequency. Denies blood in
stool, dark stools, or maroon stools. No
blood in emesis. No known jaundice,
problems with liver or spleen.
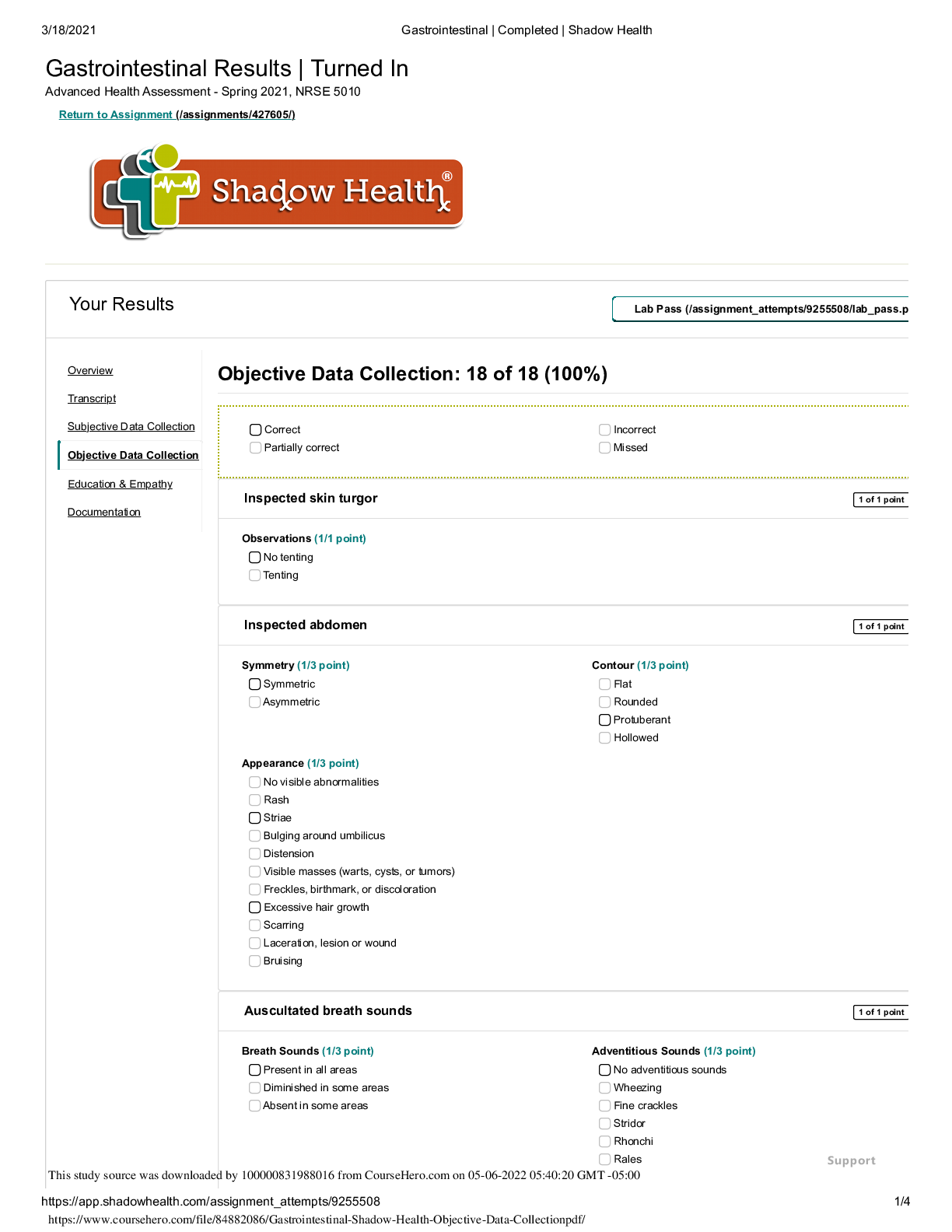
Objective
Liver span found at 7cm from costal margin.
No complaint of tenderness in all quadrants.
Liver palpable at 2 cm from costal margin.
No masses, no guarding, no distention. All
areas of abdomen normal to auscultation.
All blood vessels normal to auscultation.
Stomach tympanic throughout. Spleen not
palpable. Bilateral kidneys not palpable.
General: Ms. Jones is a pleasant, obese 28-
year-old African American woman in no
acute distress. She is alert and oriented.
She maintains eye contact throughout
interview and examination.
• Abdominal: Abdomen is soft and
protuberant without scars or skin lesions;
skin is warm and dry, without tenting. Bowel
sounds present and normoactive in all
quadrants. No tenderness to light or deep
palpation. Tympanic throughout. Liver is 7
cm at the MCL and 1 cm below the right
costal margin. Spleen and bilateral kidneys
are not palpable. No CVA tenderness.
• Cardiovascular: Regular rate and rhythm,
S1 and S2 present, no murmurs, rubs,
gallops, clicks, precordial movements. No
bruits with auscultation over abdominal
aorta. No femoral, iliac, or renal bruits.
This study source was downloaded by 100000831988016 from CourseHero.com on 05-06-2022 05:36:07 GMT -05:00
https://www.coursehero.com/file/47999252/GI-Tina-Jones-documentationdocx/
• Respiratory: Chest is symmetrical with
respirations. Lung sounds clear to
auscultation anteriorly and posteriorly
without wheezes, crackles, or cough.
Assessment
Patient has uncontrolled diabetes that is
causing polydipsia and polyuria. Patient
needs to make adjustments to her diet, as
she is consuming too many carbs. Her pain
is below the breastbone, and worsens when
she eats. It appears that the patient is
suffering from increased acid production, as
she is burping and hurting when eating. I
would treat her for GERD.
Gastroesophageal reflux disease without
evidence of esophagitis
Plan
Treat patient for GERD with histamine 2
receptor antagonist, since she is using
antacids more than once a week. Educate
patient on appropriate diet for diabetes.
Have patient follow up in two weeks. If
histamine 2 receptor antagonists do not
work, will try proton pump inhibitors.
Educate on lifestyle changes including
weight loss, engagement in daily physical
activity, and limitation of foods that may
aggravate symptoms including chocolate,
citrus, fruits, mints, coffee, alcohol, and
spicy foods. • Ms. Jones may elevate the
head of her bed or sleep on a wedgeshaped bolster for comfort or symptom
reduction. • Encourage to eat smaller meals
and to avoid eating 2-3 hours before
bedtime. • Educate on dietary reduction in
fat to decrease symptoms. • Trial of
ranitidine 150 mg by mouth daily for two
weeks. If reduction in symptoms, Ms. Jones
may continue therapy. If symptoms persist,
consider testing for helicobacter pylori, trial
of a proton pump inhibitor, or upper
endoscopy. • Educate on when to seek
emergent care including signs and
This study source was downloaded by 100000831988016 from CourseHero.com on 05-06-2022 05:36:07 GMT -05:00
https://www.coursehero.com/file/47999252/GI-Tina-Jones-documentationdocx/
symptoms of upper and lower
gastrointestinal bleed, weight loss, and
chest pain. • Return to clinic in two weeks
for evaluation and follow up.
HPI: Ms. Jones is a pleasant 28-year-old
African American woman who presented to
the clinic with complaints of upper stomach
pain after eating. She noticed the pain about
a month ago. She states that she
experiences pain daily, but notes it to be
worse 3-4 times per week. Pain is a 5/10
and is located in her upper stomach. She
describes it “kind of like heartburn” but
states that it can be sharper. She notes it to
increase with consumption of food and
specifically fast food and spicy food make
pain worse. She does notice that she has
increased burping after meals. She states
that time generally makes the pain better,
but notes that she does treat the pain “every
few days” with an over the counter antacid
with some relief.
Social History: She denies any specific
changes in her diet recently, but notes that
she has increased her water intake.
Breakfast is usually a muffin or pumpkin
bread, lunch is a sandwich with chips,
dinner is a homemade meal of a meat and
vegetable, snacks are French fries or
pretzels. She denies coffee intake, but does
drink diet cola on a regular basis. She
denies use of tobacco and illicit drugs. She
drinks alcohol occasionally, last was 2
weeks ago, and was 1 drink. She does not
exercise.
Review of Systems: General: Denies
changes in weight and general fatigue. She
denies fevers, chills, and night sweats. •
This study source was downloaded by 100000831988016 from CourseHero.com on 05-06-2022 05:36:07 GMT -05:00
https://www.coursehero.com/file/47999252/GI-Tina-Jones-documentationdocx/
Cardiac: Denies a diagnosis of
hypertension, but states that she has been
told her blood pressure was high in the past.
She denies known history of murmurs,
dyspnea on exertion, orthopnea,
paroxysmal nocturnal dyspnea, or edema.
• Respiratory: She denies shortness of
breath, wheezing, cough, sputum,
hemoptysis, pneumonia, bron
[Show More]








.png)