NURSING > MED Resources. > ATI Respiratory Review 2022 (All)
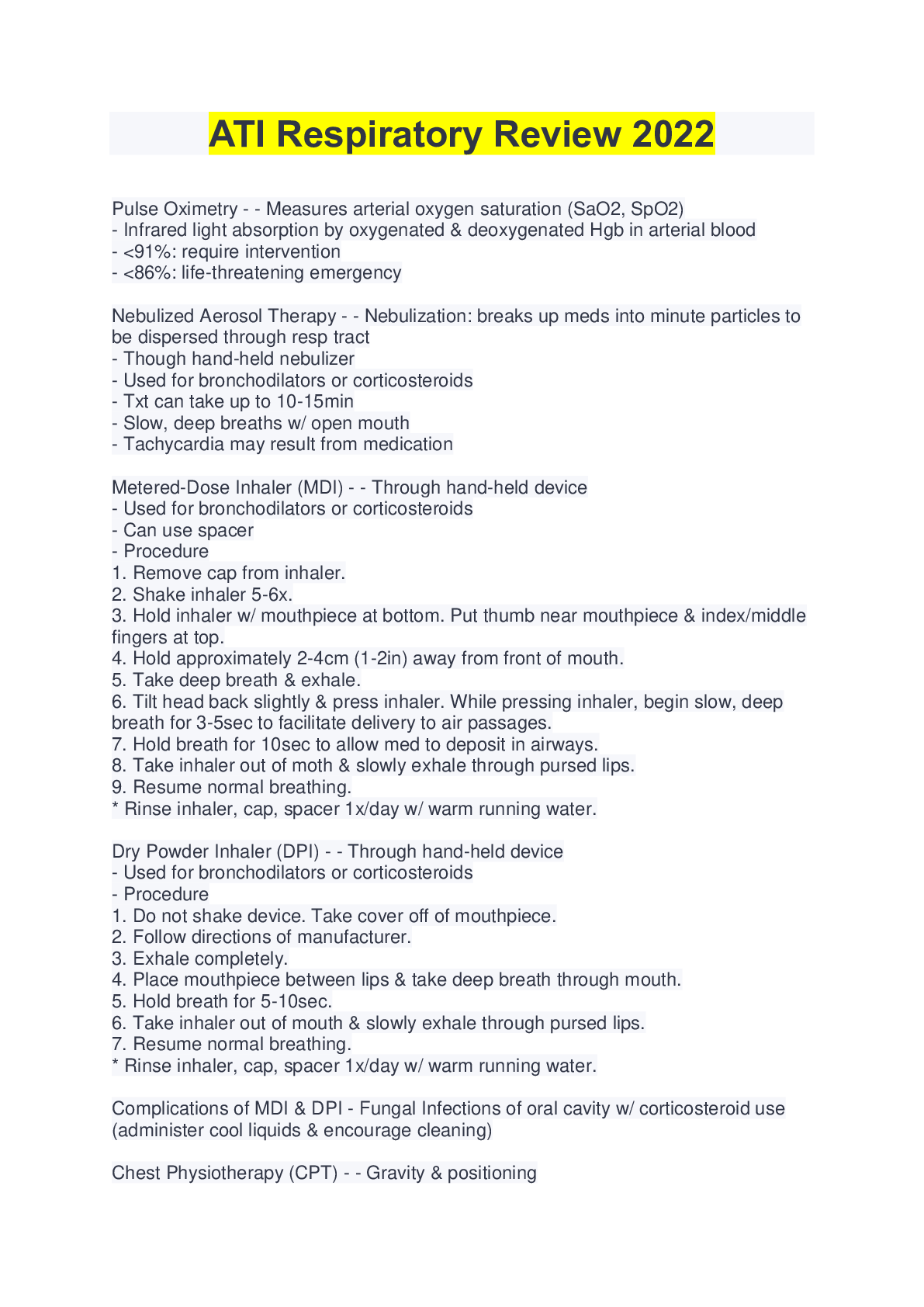
ATI Respiratory Review 2022
Document Content and Description Below
Last updated: 3 years ago
Preview 1 out of 12 pages
Instant download
Buy this Document to get the Full Access Instantly
Provided by Students Who Aced it
We Verify Document Content to Gurantee Accuracy
Also available in bundle (1)
Click Below to Access Bundle(s)
ATI Comprehensive Predictor, ATI RN Predictor, ATI COMPREHESIVE EXIT [NCLEX, RN comprehensive online practice, ATI Respiratory Review, ATI Pharmacology Practice
ATI Comprehensive Predictor Questions And Answers 2022, ATI RN Predictor Study Exam 2022, ATI COMPREHESIVE EXIT [NCLEX 2019/2022]; LOTS OF PICS, RN comprehensive online practice 2019/2022a, ATI Respir...
By BRAINEDGE 3 years ago
$22.5
6
Reviews( 0 )
Document information
Connected school, study & course
About the document
Uploaded On
Jul 16, 2022
Number of pages
12
Written in
All

Additional information
This document has been written for:
Uploaded
Jul 16, 2022
Downloads
0
Views
120
Document Keyword Tags
Recommended For You
Get more on MED Resources. »
ATI TEAS 7 Exam Test Bank – 300 Questions with Answers Latest...

ATI Fundamentals 2.0 Proctored Exam Test Bank 2025/2026 | 100...
ATI OB Test Bank | Actual Exam – 300 Questions & Verified Answ...

ATI MATERNAL NEWBORN PROCTORED EXAM | 33 VERSIONS Contains 260...
.png)
ATI MENTAL HEALTH EXAM A, B and C I Grade A+ Answers and C...

ATI MATERNAL NEWBORN PROCTORED EXAM WITH RATIONALES Version...