NURSING > STUDY GUIDE > NR 667- VISE STUDY GUIDE-comprehensive -2022 (All)
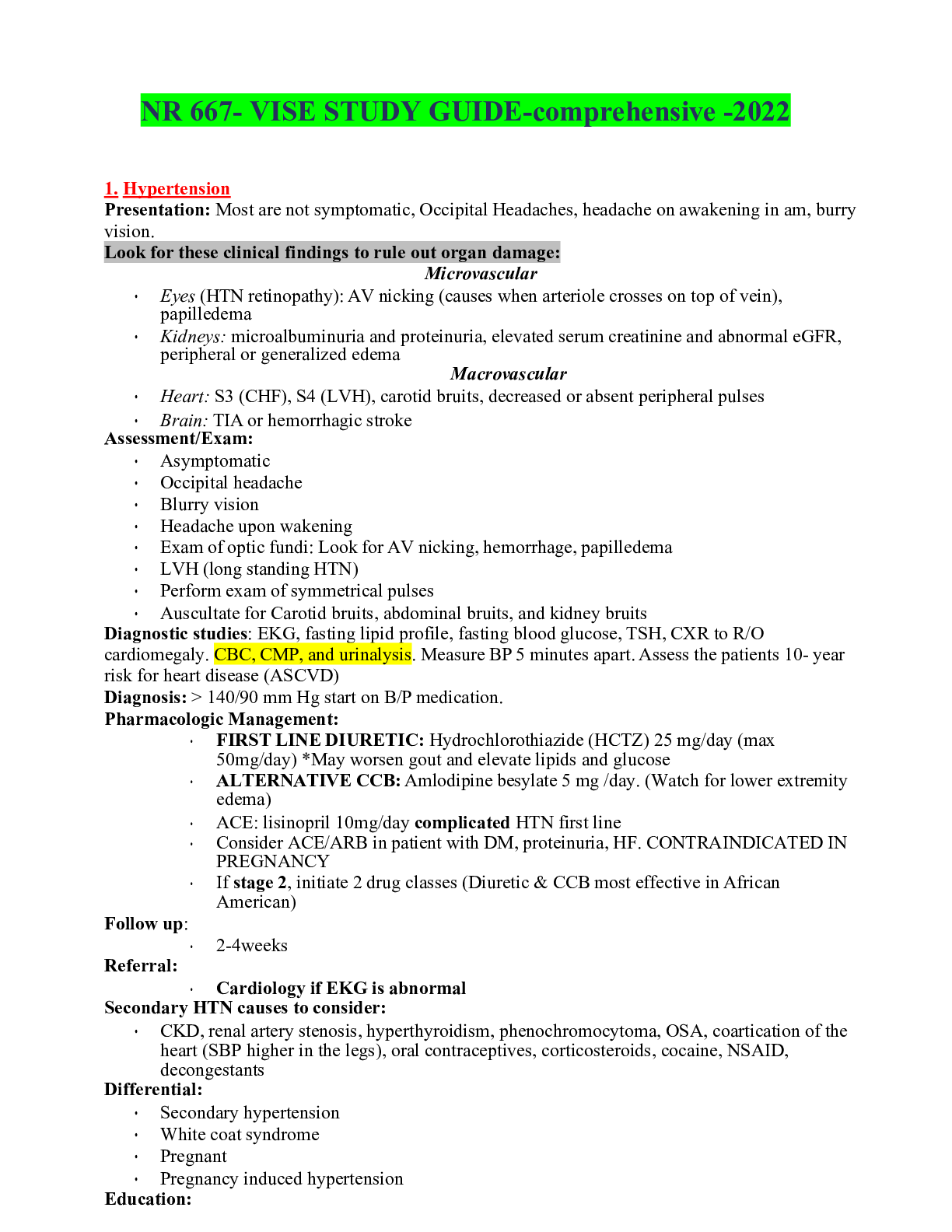
NR 667- VISE STUDY GUIDE-comprehensive -2022
Document Content and Description Below
Last updated: 3 years ago
Preview 1 out of 28 pages
Instant download
Buy this Document to get the Full Access Instantly
Provided by Students Who Aced it
We Verify Document Content to Gurantee Accuracy
Reviews( 0 )
Document information
Connected school, study & course
About the document
Uploaded On
Aug 03, 2022
Number of pages
28
Written in
All

Additional information
This document has been written for:
Uploaded
Aug 03, 2022
Downloads
0
Views
77
Document Keyword Tags
Recommended For You
Get more on STUDY GUIDE »![Preview of NR667 Complete Question Bank with Correct Answers: Final Exam Study Guide [2026 Updated]](https://browseimages.nyc3.digitaloceanspaces.com/paper-images/2026/02/25/AULA53fD2026-02-25-02-58699ee3d811bc7.png)
NR667 Complete Question Bank with Correct Answers: Final Exam...

North Carolina Wesleyan College NUR 111 NR 667 narrative templ...


NR 667 Clinical Education Assessment (CEA) Examination: An Ext...
NR 667_SAMPLE_Capstone_Portfolio_Parts_12 CAPSTONE PORTFOLIO P...

CHIM NCE Health Information Management Practice Exam 1 – Ver...



TEST BANK for Davis Advantage for Psychiatric Mental Health Nu...