NCSBN – Lesson 7: Reduction of Risk Potential Study Guide
Chest Physiotherapy Therapeutic Procedures
Chest physiotherapy is an airway clearance technique used by health care providers.
• Abdominal & Pursed Lip Breat
...
NCSBN – Lesson 7: Reduction of Risk Potential Study Guide
Chest Physiotherapy Therapeutic Procedures
Chest physiotherapy is an airway clearance technique used by health care providers.
• Abdominal & Pursed Lip Breathing
o Breathing exercises include abdominal breathing and pursed lip breathing. The
client is positioned on their back with their knees bent and hands placed on their abdomen during abdominal breathing. Pursed lip breathing is done by taking a deep breath in through the nose and pursing the lips while breathing out the mouth. The exhalation through the pursed lips should take twice as long as the inhale.
• Coughing Techniques
o Ask your client to lean forward and take deep breaths and cough several times
during expiration. The cough must come from deep in the chest to help move secretions.
• Postural Drainage
o Place clients in positions that facilitate drainage (head down, prone, right and left
lateral, and upright). Secretions produced can be coughed or suctioned out.
• Percussion & Vibration
o Perform percussion and vibration during postural drainage. Percussion is a
rhythmic striking of the chest with cupped hands and is alternated with vibrations. Vibrations are executed when the client exhales and pressure is applied to the chest.
• Incentive Spirometer
o An incentive spirometer is used to maximize respiration and mobilize secretions.
Tracheostomy Care & Suctioning Therapeutic Procedures
• Complications of tracheostomy care include airway obstruction, tracheal necrosis and infection. Complications of suctioning include hypoxia, bronchospasm, vagal stimulation,
tissue trauma, cardiac dysrhythmia and infection.
• Maintaining a patent airway is the nursing priority.
• The cuff is used to prevent aspiration and the pressure should be maintained at 14-40 mmHg.
• Encourage fluids to facilitate removal of secretions and provide good oral hygiene. Indications for suctioning a tracheostomy include noisy respirations, restlessness, increase pulse or respirations, and a presence of mucus in the airway.
• Complications that you should be sure to assess for are infection, tracheal necrosis, and airway obstruction.
Oxygen Therapy Therapeutic Procedures
• Complications related to oxygen administration include infection, drying of mucosa, respiratory depression, oxygen toxicity and combustion. Be sure to change masks and
tubing daily and attach humidification if needed. Monitor the respiratory rate frequently to watch for depression and toxicity.
• If the client is using oxygen in their home, the visiting nurse will assess the electrical plugs and equipment. Remind the client of the danger associated with smoking near
oxygen. Place a sign on the front door that oxygen is in use.
Method
Nasal Cannula Oxygen Delivered
23-42% at 1-6 L/min
Method
Face Mask Oxygen Delivered
40-60% 6-8 L/min
Method
Partial Rebreather Mask Oxygen Delivered
50-75% at 8-11 L/min
Method
Nonrebreather Mask Oxygen Delivered
80-100% at 12 L/min
Method
Venturi Mask Oxygen Delivered
24-40% at 4-8 L/min
Method Oxygen Delivered
Tracheostomy Collar 30-100% at 8-10 L/min
Method
Oxygen Hood Oxygen Delivered
30-100% 8-10 L/min
Chest Tubes Therapeutic Procedures
A chest tube system is an intrapleural drainage system with one or more chest catheters in the pleural space attached to a drainage system.
• Nursing Considerations
o The water-seal chamber should be filled with sterile water to the level that is
specified by the manufacturer. If suction is to be used, the suction control chamber will need to be filled (per the health care provider's orders). Encourage clients to change positions as often as they can, cough and take deep breaths.
o The drainage system must be kept below the level of insertion. The system should be checked frequently for kinks in the tubing. Observe for fluctuations of fluid in the water-seal.
o To remove the chest tube, have clients forcibly bear down while holding their breath (Valsalva maneuver). The health care provider will remove the tube and the nurse will apply an occlusive dressing.
o Drainage in the system is expected; however, drainage that is more than 70-100 mL/hour is considered excessive and the health care provider should be notified.
o The chest tube insertion site is covered with an occlusive (airtight) dressing to prevent air from entering the pleural space.
o Positioning the drainage system below the client's chest allows gravity to drain the pleural space.
o
• Complications
o If there is an air leak in the system indicated by a constant bubbling in the
water-seal chamber, the health care provider must be contacted.
o If the chest tube becomes dislodged, the nurse will apply pressure over the site and let air escape. Contact the health care provider immediately.
o If the tube becomes disconnected from the drainage system, cut the contaminated tip off and insert a sterile connector. Then reattach it to the drainage system.
Central Venous Pressure (CVP) Therapeutic Procedures
CVP measures blood volume and efficiency of the cardiac pump. A central line is threaded into the right atrium to measure the central venous pressure.
• Procedure
o The client will have a catheter inserted in the jugular, subclavian or antecubital
vein.
o The manometer will attach to a three-way stopcock that is also connected to the IV to the central catheter.
o The stopcock is opened to allow fluid in the manometer to flow to the client.
o The client must be in a flat bed.
o When the level stabilizes, the reading is taken at the highest level of fluctuation.
o Normal readings range between 2-6 mm.
▪ High levels indicate hypervolemia and low levels indicate hypovolemia.
• Nursing Care
o Maintain a dry, sterile dressing and change dressing, IV bag, manometer and
tubing every 24 hours.
o Instruct clients to hold their breath when the CVP is inserted, withdrawn or
when a tube is changed to prevent an air embolism.
o Monitor clients for complications, which include pneumothorax from catheter insertion, air embolism or an infection at the insertion site.
Ear Procedures Therapeutic Procedures
Common ear procedures conducted by the nurse include ear irrigations and administering ear drops.
• Ear Irrigation
o The client will tilt their head and the nurse will direct a stream of fluid against the
sides of the ear canal.
o The client will lie on the affected side to improve drainage.
o Do not irrigate if you observe swelling or tenderness.
• Ear Drops
o Pull the outer ear up and back for an adult, or down and back for a child.
o Place the drops so they run down the wall of the ear canal. Have the client lie with the affected ear up to allow for absorption.
Eye Procedures Therapeutic Procedures
Common eye procedures include eye irrigation and eyedrop instillation.
• Eye Irrigation
o The client will tilt the head back and the nurse should direct fluid from the inner to the outer canthus using a small bulb syringe. Have a basin close by for fluid collection.
• Eyedrop Instillation
o The dropper should be sterile and will not touch the eye during the procedure.
o Have the client tilt their head back and look up.
▪ The drops should be placed into the center of the lower conjunctival sac.
▪ Have the client blink several times between drops.
Nasogastric Tubes
Therapeutic Procedures
A nasogastric tube may be placed to decompress the abdomen, administer medication or provide nutrition.
• 14-16 F
• Place the tube at the tip of the nose and measure by extending the tube to the earlobe and then down to the xiphoid process.
• Lubricate 3-4 inches of the tube
• Extend neck back on the insertion
• When you passed the nasal pharynx, asked patient to swallow (fluids), unless contraindicated to help with the placement of the tubing
• With the end of the tube just above the oral pharynx, flex the patient’s head FORWARD
• Advance the tube an inch or 2 as patient swallow
Nursing Interventions in Gastric or Intestinal Intubation
• Intubation
o Before inserting anything through the nares, check for patency and for history of
deviated septum, nosebleeds, anticoagulant therapy (if history is positive, confirm insertion route with care provider)
o Standard precautions must be used; gown and gloves are recommended and the nurse should also consider face and eye protection
o Remove client's dentures
o Position client in high Fowler's
o Measure for length of tube:
▪ Adults — from tip of nose to ear lobe to xiphoid process
▪ Infants — from tip of nose to earlobe to midway between xiphoid process and umbilicus
o Instruct client to bend head forward and to swallow during insertion; take small sips of cold fluid through a straw or ice chips may help (babies can suck on a pacifier)
o Lubricate 2-4 inches (5-10 cm) of the tube with lubricant
o Insert, but do not force, the tube
o Check placement of tube :
▪ By X-ray
▪ By aspiration of stomach contents to test for pH (for gastric placement, should be less than five)
▪ Do NOT auscultate for instilled air — you can't be sure that the sound you hear is actually coming from the GI tract
o Document:
▪ The reason for the tube insertion
▪ Type and size of tube
▪ The nature and amount of aspirate
▪ The type of suction and pressure setting if for suction
▪ The nature and amount of drainage
▪ The effectiveness of the intervention, i.e., no more nausea or vomiting
• Care of the intubated client:
o Provide frequent mouth and nose care
o Re-tape or anchor PRN
o Monitor fluid and electrolyte balance
o Monitor tube for patency — aspirate tube prior to any infusions and check for kinks
o Irrigate tube per orders — usually with tap water or sterile normal saline
o Monitor for signs of metabolic alkalosis or acidosis:
o Metabolic alkalosis — if tube is located in the stomach
o Metabolic acidosis — if tube is located in small intestine
o Record amount of and color of output
o Observe for and respond to complications: pulmonary aspiration, abdominal distention, nausea, vomiting
Surgical Drains
Therapeutic Procedures
Surgical drains are used to collect excess fluid from a surgical wound.
• Penrose
o A penrose drain is a simple latex drain that is freely laid inside the wound/site
without sutures to hold it in place. Drainage flows onto a gauze dressing.
• T-Tube
o A T-tube is commonly used after gallbladder surgery.
o It is placed in the common bile duct to allow the passage of bile.
o The nurse will keep the drain below the client's waist and fasten the drain to the dressing for safety.
o The nurse will monitor the drainage and teach their client how to care for the drain if they are being discharged with it.
o The drain must be clamped one hour before and after each meal.
• Jackson-Pratt Drain
o A Jackson-Pratt drain is a self-suction drain with a collection reservoir.
o The nurse will monitor the amount and character of the drainage and notify the health care provider if the drainage turns bright red.
• Hemovac
o A hemovac is a large, portable wound self-suction device with a reservoir.
o The hemovac is commonly used after a mastectomy.
o The nurse will monitor the amount and character of the drainage and notify the health care provider if the drainage turns bright red.
Enema
Therapeutic Procedures
• There are three types of enemas
o oil retention
o soapsuds
o tap water
• During the procedure, the solution is instilled into the rectum and sigmoid colon to promote defecation.
• The client will be in a Sims' position while the nurse inserts the tip of the tube no more than 3-4 inches into the rectum.
• The client should hold onto the solution for 5-10 minutes if possible.
• Do not administer an enema if the client complains of abdominal pain, nausea, vomiting or if you suspect appendicitis.
Urinary Catheters Therapeutic Procedures
• The nurse will provide perineal hygiene, using soap and water or otherwise following the health care organization's procedure.
• Observe the client for signs of inflammation or infection and maintain patency of the catheter (irrigate if ordered).
• Document intake and output (I/O).
• Empty system every shift or when it is half to three-quarters full. Be sure to keep the collection system lower than the level of the bladder. Take measures to prevent catheter-
associated urinary tract infections.
• In general, the larger the gauge number is the larger the catheter size
o Smallest effective catheter size is preferred to prevent trauma
▪ Children: 8 – 10 Fr
▪ Adults: 14 – 16 Fr
▪ Young girls: 12 Fr
o Types of Catheters
Ostomy
▪ ST Indwelling
• When urine outflow is obstructed
• When bladder, urethra, and surrounding structures have been surgically repaired
• When continuous or intermittent bladder irrigations are required
▪ LT Indwelling
• When chronic urinary retention is not manageable by intermittent catherization
• With terminal ill patients when bed linen changes or toileting is painful
• When skin is irritated by urine and forms skins rashes and shit
▪ Intermittent
• A single-use straight catheter is introduced for 5-10 mins, just long enough to drain the bladder
o Common in patients who have incomplete bladder emptying d/t neurogenic conditions
o Used to obtain a sterile urine specimen
o Used to assess residual urine after urination
o Used to manage residual stricture
• Coude Catheter
o Has a curved tip and is used for MALE patients who have
enlarged PROSTATES that partly obstructs the urethra
o Stiffer and easier to control than the straight tip catheter
Therapeutic Procedures
Creating an ostomy is a surgical procedure that creates an opening into the abdominal wall for fecal or urinary elimination. A portion of intestinal mucosa or ureter is brought through the abdominal wall, creating a stoma through which feces or urine can drain.
• Types
o Bowel ostomies include an ileostomy or colostomy.
o Urinary diversions include ileal conduit (ileal loop) and ureterostomies.
• Nursing Interventions
o The ostomy pouch should be emptied when it is about one half full using standard
precautions and the skin will need to be protected around the stoma (see organizational policy).
o The nurse will monitor for and report immediately if the stoma oozes blood when touched, if there is blood in the pouch or any kind of bleeding from the stoma.
o Contact the health care provider if a urinary diversion output is less than 30mL/hour or if the urine has a foul smell, is cloudy or has blood in it.
o If the client is experiencing a burning sensation around the base of the urinary diversion stoma or they have back pain, chills or a fever, an infection may be present.
o The nurse will also address any issues with body image, fear of mutilation or shame which are common with new ostomy clients.
o The nurse will also provide teaching on the types of equipment used in ostomy care and maintenance, how to irrigate a colostomy, how to prevent complications and how to avoid constipation, diarrhea and excessive gas.
Evaluate your Client's Stoma
You are documenting your observations of a client's stoma. Consider the image above. How would you describe the stoma's overall appearance?
Describe the color of the stoma.
How would you describe the shape?
Describe the overall appearance of the effluent. The color is brown-yellow, how would you describe the consistency.
Describe the characteristics of the peristomal skin. This stoma is moist, shiny and smooth.
The effluent is liquid. You would also describe the presence or absence of odor when you document the effluent. (It might be strong, foul, pungent, fecala, musty or sweet.)
The skin is intact, excoriated directly around the stoma. Hemodialysis
Therapeutic Procedures
• Hemodialysis removes accumulated waste products though the cleansing of the blood. It can be used short-term for acute illness or long-term with clients in renal failure.
• Complications include
o hemorrhage, hepatitis, nausea and vomiting, disequilibrium syndrome, muscle
cramps, air embolism and sepsis.
• The nurse will check the "thrill" and bruit every eight hours. Blood pressure and lab draws are not to be conducted on the affected extremity.
Intra-aortic Balloon Pump
• The intra-aortic balloon pump is a device that helps blood circulate after myocardial failure.
• The device will not be used with clients who have aortic regurgitation, dissection or an abdominal aortic aneurysm. Complications include infection, bleeding, hematoma, diminished or absent pulse and/or thrombus at insertion site. The pump can cause an aortic dissection or perforation, thrombocytopenia, dysrhythmias and myocardial failure.
• An informed consent form must be obtained prior to the procedure. The nurse will take the client's baseline vital signs, hemodynamic parameters and ECG as ordered. The nurse will monitor the client's level of consciousness (LOC) and obtain arterial blood gases as ordered. It is important to maintain asepsis, monitor I/O and monitor for complications frequently.
• IMPORTANT:
o The client cannot bend the leg in which the balloon was inserted. This is an
uncomfortable and difficult task for the client. Maintain emotional support to the client and family during the duration of the monitoring process.
Level of Consciousness
Pacemaker
Therapeutic Procedures
• A pacemaker is a battery-powered pulse generator that stimulates the heart via electrodes that transmit electricity to the heart. They are commonly used to correct dysrhythmias such as sinus bradycardia or ventricular tachycardia.
• Complications for pacemakers include
o infection, perforation of myocardium, pneumothorax, hemothroax, dysrhythmia,
thrombosis, pacemaker failure, syncope, hypotension, pallor, hiccups and shortness of breath.
• Informed consent must be obtained prior to the procedure. The nurse will initiate preoperative care as ordered. The client's vital signs and ECG will be monitored as well
as post-anesthesia care post-procedure. The client will be on bed rest as ordered.
Client teaching will include:
• How to take their pulse and when to report a sudden increase or decrease in rate
• Carry an ID card and request hand scanning at security check points at airports
• Avoid situations involving electromagnetic fields
• Periodic battery replacement and medical follow-up
• Frequent rest periods at home or work
Document information about your client's pacemaker including including the model of the pacemaker, date and time of insertion, location of the pulse generator, stimulation threshold and pacer rate.
Automatic Implantable Cardioverter-Defibrillator (AICD) Therapeutic Procedures
• An AICD is a pulse generator implanted in a subcutaneous pocket. It delivers an electrical shock to the heart when a ventricular tachycardia or ventricular fibrillation is
detected. It is used to treat life-threatening ventricular dysrhythmias.
• Complications include
o infection, malfunction and battery failure. Informed consent must be obtained
prior to the procedure. The nurse will initiate preoperative care as ordered including medications and ECG.
Client teaching will include:
• Findings of defibrillation discharge
• Importance of routine follow-up
• Findings of complications
• Limit activity as ordered
• Avoid strong magnetic fields
• Wear MedicAlert® identification
• Assure client that no household appliance will affect AICD
• Shock may be painful
Endotracheal Tubes
• Therapeutic Procedures
o Endotracheal tubes (ET) are placed when an artificial airway is needed.
o Check the tube placement by listening for bilateral breath sounds and looking for bilateral chest movement. The client will be monitored via pulse oximetry. Typically an X-ray is ordered for placement confirmation.
o The nurse will regularly assess tube placement and security, breath sounds, and bowel sounds.
o The ET tube should be marked where it touches the mouth or teeth and be secured with tape to stabilize.
Ventilator
• Therapeutic Procedures
o A ventilator is used when the client needs assistance getting oxygen into the lungs
and removing carbon dioxide from the body. The nurse must have the knowledge and skills to effectively and safely maintain a client that is on a ventilator.
• Ventilator Settings
o Tidal volume: amount of air delivered with each machine breath
o Rate: number of breaths delivered by the machine in a minute
o FIO2: fraction of inspired oxygen (written as 0.6)
o % O2: percent of oxygen (for example: 60%)
o FIO2 of 0.6 = 60% oxygen
o Signs: deep breaths (higher volume) delivered periodically by ventilator
o Positive end expiratory pressure (PEEP):
▪ Normal physiologic PEEP is equal or less than 5 cm H2O
▪ Provides a baseline of positive pressure throughout exhalation
▪ Used to reduce airway collapse and intrapulmonary shunting
• Nursing Considerations
o Clients on a ventilator will have their vital signs assessed every four hours.
o Breath sounds will be evaluated for any abnormalities and continuous pulse oximetry is required.
o The nurse will assess for suctioning needs and provide good oral care at least twice a shift.
o Evaluate symptoms of hypoxia, neurologic status and ABG. Be sure to observe for skin breakdown around the tube site and for complications of aspiration.
o The nurse will ensure ventilator is working properly.
▪ If the high-pressure alarm goes off – check for tube obstruction:
• Client biting the tube
• Increased secretions
• Tube slipping into right main stem bronchus
• Pneumothorax
▪ If the low pressure alarm goes off – check for disconnection of tubes.
Dressing
Types Description Use Advantage Disadvantage NC
Gauze • Oldest, most common dressing.
• It comes in woven and non- woven forms.
• Gauze may be impregnated with various products, e.g., antimicrobials. • draining wounds,
• necrotic wounds,
• wounds with tunnels, tracts or
dead space
• surgical incisions
• burns
• pressure ulcers. • Wicks away wound exudate
• Does not interact with wound
• Comes in many sizes and lengths • Must be held in place by a
secondary dressing
• Fibers may shed or adhere to wound
Non- Adherent • Made with a substance that hinders sticking (example: Telfa
pad).
• Nonmedicated tulles, silicone, and petrolatum-based woven
dressings • • absorbs wound exudate • does not stick to the wound. • Require a cover (absorbent)
dressings
Transparent Film • Made of polyurethane or copolymer.
• It has a porous adhesive layer that lets oxygen pass through and allows moisture vapor to
escape from the wound. • small, superficial wounds, e.g., over
IV insertion sites • Doesn't have to be removed to examine
wound
• Impermeable to external fluid and bacteria
• Available in many sizes • Fluid retention under dressing may
lead to peri-wound maceration • Has been used for small, superficial
wounds (skin tear or for high risk skin)
• stage I or II pressure ulcers
• partial-thickness wounds.
• Useful in securing IVs and other
tubings since they provide occlusive barrier
• Difficult to remove and may cause
unnecessary trauma: remove with a “LATERAL PULL”
technique
Hydrocolloi d • swells to accumulate exudate when it contacts the wound. • shallow to moderate dermal wounds,
e.g., venous or arterial ulcers and decubitus ulcers. • Debrides
• Maintains wound humidity
• Liquefies necrotic debris impermeable to contaminants
• May stay safely for days • Occlusive — does not allow air contact • Should not be used on heavily draining
or infected wounds
• Characteristic odour may accompany
dressing change and should not be confused with infection
Hydrogel • is impregnated with water or glycerin-based amorphous gel
(high water content)
• Available in gels, solid sheets, or impregnated gauze
• non-adherent. • Partial or full thickness wounds
• Burns
• deep or necrotic wounds
• radiation-damaged
skin. • Decreases pain
• Maintains humidity
• Debrides
• Does not stick to wound
• Can be used with infected wound • Must be covered with another
dressing • Should not used on draining wounds
• Solid sheets should not be used on infected wounds
Composites • combinations of two or more different products, featuring a
bacterial barrier, absorptive layer, foam, hydrocolloid or hydrogel.
• Increase absorbency and
autolysis • • Facilitate autolytic debridement
• Conformable and easy to apply and remove
• Come in many sizes and shapes • May be contraindicated for
stage IV pressure ulcers
• Adhesive borders limit use on fragile
skin • Use on wounds on which dressing may
stay in place for several days
Foam • is an absorptive dressing consisting of hydrophilic
polyurethane (non-adhesive or adhesive) or film-coated gel. • stages II-IV pressure ulcers
• partial- and full-
thickness wounds • Comes in many sizes, shapes and
forms
• Conformable
• Easy to apply and • Secondary dressing or tape may be
needed to secure in place
• Not recommended • Used on moderate to heavily draining
wounds
• Occlusive foams
• Sheets or cavity packing
• Some have fluid lock with drainage or surgical wounds. easy to remove (non-adherent) for non-draining wounds or dry eschar
• May lead to macerating
periwound skin if not changed appropriately SHOULD NOT be
used on heavily draining ort infected wounds
Alginates • made from polysaccharide from seaweed. • moderately or highly exudative
wounds. • Forms gel on wounds and moist
environments
• Reduces pain
• Can be used to pack cavities
• Low allergenic • Not recommended for dry wounds or
hard eschar
• May require secondary dressing
• Not recommended in anaerobic infections •
Hydrophilic Fibres • Sheet or packing strip of sodium carboxymethyl-cellulose
• Converts to a solid gel when activated by moisture (fluid lock) • Best for moderate amount of exudate • • • Not used on dry wounds
• Avoid packing into narrow deep sinuses
b/c of low tensile strength
Hypertonic • Sheet, ribbon, or gel impregnated with sodium
concentrate • Gel may be used on dry wounds • • • Gauze ribbon should not be used
on dry wounds
• May be painful on
sensitive tissues
Casting & Traction Therapeutic Procedures Casting
• Casting immobilizes the affected body part.
• Casts may be plaster or fiberglass.
o With plaster casts, immediately after the cast is placed it should not be covered
and allowed to dry.
o The client will avoid resting the cast on hard surfaces or edges.
o The affected limb should be elevated above the heart on a soft surface.
o Monitor for complications such as blueness/paleness, pain, numbness or tingling sensations on the affected area.
• Once the cast is dry, the client can be mobile. Encourage any prescribed exercises.
• The client will report any breaks or foul smells from the cast. Although difficult, the client should not scratch the skin under the cast or put anything underneath the
cast. If the skin breaks under the cast, an infection is likely.
• Complications include
o impaired circulation, peripheral nerve damage and pressure necrosis.
Traction
Traction –- pulling force and opposing force applied to an injured extremity.
• Purpose
o The purpose of traction:
▪ To align the needs of a fracture by pulling the limb into a normal anatomical position
▪ To reduce muscles spasms
▪ To relieve pain
▪ To take the pressure off the ends of bones by relaxing the muscle
• Application
o Traction is applied using one of two methods.
▪ Skin Traction
• Uses 5-7 pound (2.27-3.18 kg) weights attached to the skin to indirectly apply force
• Weights are attached either through tape, using straps, boots or cuffs
• Examples:
o Buck's traction: used to immobilize, position, and align the
lower extremity in the treatment of contractures and diseases of the hip and knee
▪ Russell’s traction
• Buck’s with a ling under the knee
o Promotion of neurovascular integrity is the most important aspect of care: assess pedal pulse, color, temperature, sensation and capillary refill of the involved extremity.
o Donlop's traction: used for children with fractures of the upper arm when the arm must remain flexed
o Pelvic traction
o Bryant's traction: used to immobilize both lower extremities in the treatment of a fractured femur or in the correction of a congenital hip dislocation
▪ Skeletal Traction
• Skeletal traction uses pins inserted into bones:
o Used when more pulling force is needed than skin traction
can provide
o Approximately 25-40 pounds (11.34-18.14 kg) of weight can be applied
o Requires the surgical placement of tongs, pins or screws into the bone
The TLSO (thoracolumbosacral orthotic) is a custom molded brace prescribed to give support to the spinal column from the sixth thoracic vertebra to the sacrum. Clients are advised to wear only a tight fitting t-shirt under the brace to protect the skin and absorb sweat. Although the brace will not be damaged by water, it is typically removed when showering; the client will need to lie down to remove or put on the brace. The health care provider will instruct the client about how often and how long to wear the brace each day. The client is instructed not to attempt to bend or to lift objects weighing more than 10 pounds.
• Nursing Care
o Traction:
▪ Be sure to know if the traction is to be applied either intermittently or continuously
▪ Be sure to know the amount of weight to be applied
▪ Check ropes and knots, pulleys and weights at least once a shift:
• Rope should move freely over pulleys
• Prevent friction, which will impair the efficiency of the traction
▪ Weights should hang freely
▪ Identify and maintain countertraction:
• Countertraction is the force opposing the pull of traction, which is generally provided by the client's body
• If countertraction is not maintained, the client is not in traction
• Sign of loss of countertraction is that the client slides down in bed
• Elevate the foot of the bed with shock blocks
▪ Maintain client in correct alignment and body position
▪ Skin care:
• Regular assessment for breakdown, especially coccyx and heels but also all bony prominences
• Assessment and care of pins, wires or tongs with skeletal traction and observe for signs of infection
• Assessment of skin by removing traction at least once per day for hygiene and reapplication (manual traction should be used while skin traction is off)
▪ Perform regular neurovascular checks approximately every four hours
and document:
• Sensation
• Temperature
• Movement
• Distal perfusion
▪ Assist client to cough and deep breathe and to use incentive spirometer
▪ Assist with range of motion exercises
▪ Assist client with use of trapeze
▪ Assess for skin breakdown
Bone Marrow Transplant Therapeutic Procedures
A bone marrow transplant is used to replace or stimulate non-functioning bone marrow. It is done through an intravenous infusion from the donor to the recipient. Clients with leukemia, aplastic anemia and immunodeficiency disorders are common candidates for bone marrow transplants.
• Types
o An autologous transplant is when a client receives their own bone marrow cells,
harvested before high-dose chemotherapy or radiation.
o A syngeneic transplant is used when the donor and recipient are identical twins.
o An allogeneic transplant is used when the donor is not genetically identical to recipient but is a match.
• Complications
o Infection: precautions to take to avoid infection
o Thrombocytopenia
o Anemia
o Micropulmonary emboli
o Bleeding
o Stomatitis
o Nutritional deficiencies
o Disease relapse
o Graft rejection
o Graft Versus Host Disease (GVHD):
▪ Occurs when donor T lymphocytes introduced into a host who is immunologically incompetent
▪ T lymphocytes proliferate and attack host cells, which they think are foreign
▪ GVHD risk peaks 30-50 days after BMT
▪ Graded according to degree of organ involvement
▪ Findings include dermatitis, hepatitis and enteritis with diarrhea
• Nursing Considerations
o Pharmacological treatment includes Cyclosporin A (immunosuppressant
drug), steroids and anti-thymocyte globulin (immunosuppressant drug).
o The nurse will explain the procedure to the client, answer any questions and obtain the client's informed consent. The nurse will also:
▪ Assess baseline hemodynamic status prior to the injection
▪ Assess vital signs every 15 minutes during infusion post-procedure
▪ Encourage intake of fluid and high protein, high calorie diet
▪ Provide frequent oral hygiene
▪ Weigh the client daily
▪ Measure I/O
▪ Monitor all mucous membranes, wounds and catheter sites daily
▪ Administer total parenteral nutrition (TPN) if ordered
▪ Maintain isolation as ordered (reverse isolation or laminar air flow room)
▪ Sterilize any non-sterile objects before bringing them into the room
▪ Administer medications as ordered
▪ Test urine, stool and emesis for occult blood
▪ Report any signs of bleeding immediately
▪ Avoid invasive procedures
▪ Maintain a safe environment
▪ Encourage progressive activity as ordered
▪ Provide emotional support
▪ Observe for findings of complications
• Client Teaching
o Self-care procedures
o Findings of complications
o Infection precautions
o Safety precautions
o Importance of good nutrition
o Importance of good oral hygiene Precautions - Bone Marrow Transplant
After discharge from the hospital, bone marrow recipients recover at home for 2-4 months and generally cannot return to full-time work for up to six months after the transplant. The following is a list of precautions these individuals should take to reduce their risk of infection.
• Don'ts
o The following is a list of things to minimize contact with or to avoid.
▪ Avoid contact with school children
▪ Avoid crowded places, e.g., movie theaters, grocery stores, department stores
▪ Avoid contact with anyone with a communicable disease
▪ Minimize contact with pets:
• Cats:
o Do not place the litter box in the kitchen, dining room or
other area of the house where food is prepared or eaten
o Someone else should be responsible for daily litter box cleaning for six months after the transplant
▪ Avoid contact with reptiles, ducklings or chicks
▪ Avoid swimming pools or walking/wading/playing in recreational water for first year
▪ Avoid immunizations without physician's approval
▪ Prevent infections transmitted by direct contact and respiratory transmission:
• Avoid gardening, mulching, raking, mowing, farming, or direct
contact with soil and plants
• Prevent respiratory infections:
o Avoid close contact with people who have respiratory
illnesses, e.g., cough, cold
o Avoid crowded areas, e.g., movie theaters, grocery stores, department stores
o Avoid construction sites
o Avoid wood-burning fireplaces
o Avoid the use of a room humidifier (due to water- harboring bacteria)
▪ Avoid restaurant food for first three months
▪ Avoid drinking well water, unless the water is tested more than twice a day for bacterial contamination
• Do's
o The following is a list of things to do.
▪ Personal hygiene:
• Wash hands with antimicrobial soap and warm water, use hand sanitizer when outside the home:
o Before eating
o Before and after preparing food
o After touching pets or animals
o After sneezing, coughing, or blowing nose
o Before and after any central venous catheter care or intravenous infusion
o Before taking oral medications
o After touching soiled linens or clothes
• Brush teeth and gums
• Shower or bathe as usual; however, do not submerge central venous catheter under water
▪ Take prophylactic antibiotics
▪ Call the doctor if any of the following signs or symptoms occur:
• Cloudy or foul-smelling urine
• Cough with yellow or green sputum or a persistent, dry cough
• Diarrhea
• Exposure to varicella, strep throat, herpes, or mononucleosis
• Fever of 100° F (37.8° C) for allogeneic clients or 100.5° F (38.1° C) for autologous clients
• Lesions or white patches in the mouth or on the tongue
• Redness, swelling, tenderness, or drainage at the site of the
central venous catheter
• SOB
• Sinus drainage, nasal congestion, headaches, or tenderness along the upper cheekbones
• Skin rash
• Sore throat, scratchy throat, or pain when swallowing
• Sweats or chills
• Trouble urinating
• Vaginal discomfort, itching, or unusual discharge
▪ Note: individuals are not required to wear a mask when they go outside their homes, but some might feel "safer" wearing a mask
Client Care - Steroid Therapy
• Never discontinue medications abruptly – it could precipitate an acute crisis
• Take medication with breakfast – corresponds to biorhythms and reduces gastric irritation
• Take the higher dose in morning and lower doses in evening
• Always take medication with a meal or a snack
• Carry extra medication during travel
• Contact the health care provider during periods of acute or chronic stress, such as pregnancy or infections; medications will need to be adjusted and additional instructions
may be needed
• Wear MedicAlert® identification and always carry a medical card
• Avoid other people with infections or avoid going to crowded shopping malls, grocery stores, or other venues in times when the cold viruses and influenza are most evident
• Encourage weight-bearing exercise and an increase in protein and calcium intake, especially for women, who will be at an increased risk for bone loss and osteoporosis when undergoing steroid therapy
• Wear sun block with an SPF of 15 or higher; avoid direct sunlight from 10 am to 4 pm – due to increased sensitivity to sunlight
• Recognize the normal signs of infections and understand the importance of contacting the health care provider at the onset of any sign of infection – steroid use masks the signs of infection
• Be aware of the anticipated side effects of (long-term) steroid therapy, including:
o Weight gain
o Swelling of face, hands, ankles
o Skin changes:
▪ Excess hair growth on face, hands, arms, back, legs
▪ Easy bruising, thinning of skin
▪ Acne of the face, back and chest (teens and young adults)
o Mood swings and depression
o Increase in blood sugar levels – client may need to take insulin Radiation Therapy
Therapeutic Procedures
Radiation therapy uses high-energy radiation to shrink tumors and kill cancer cells. X-rays, gamma rays and charged particles are types of radiation used for cancer treatment. The nurse must have knowledge on how to prepare and provide aftercare for clients having radiation therapy.
• Radiation Safety
o Always minimize the client's exposure to radioactivity, whether the therapy is
intra-cavity, interstitial or metabolized.
• Side Effects
o The severity of the side effects depends on the location of the radiation.
o Acute
▪ Fatigue
▪ Reddened, dry, itchy skin (possible sloughing and oozing)
▪ Alopecia (hair falls out)
▪ Altered taste
▪ Xerostomia (dry mouth)
▪ Esophagitis
▪ Anorexia
▪ Nausea and vomiting
▪ Diarrhea
▪ Cystitis
▪ Anemia; decreased white blood count; decreased platelets
▪ Pneumonitis
▪ Decreased sperm count; sterility
o Chronic
▪ Permanent darkening of skin
▪ Permanent taste alteration
▪ Dental caries
▪ Fibrosis of gastrointestinal tract
▪ Malabsorption
▪ Radiation nephritis
▪ Cataracts
▪ Pulmonary and cardiovascular fibrosis
• Methods of Delivery
o Teletherapy is an external therapy treatment from a source outside the body.
The tumor area is marked and other anatomical areas are protected.
o Radiation is administered in small doses over time.
▪ Brachytherapy – is internal therapy radiation, which is placed in or directly on the body.
▪ Intra-cavity therapy – is when radiation is inserted into a body cavity. This is often used with gynecological cancers.
▪ Interstitial therapy – is the insertion of radioactive seeds, needles or capsules. This is used in head and neck lesions, intra-abdominal and intrathoracic lesions.
▪ Metabolized therapy – is when radioactive material is ingested, installed or injected into the body; used for thyroid, leukemia, bone and intra-pleural lesions.
• Nursing Considerations
o The nurse should be knowledgeable about the type of radiation used, the half-life
of the isotope, the amount of isotope being used and the method of delivery.
o The nurse will provide skin care and encourage the client to avoid using soaps and lotions on the radiated site.
o Small, frequent, bland meals will initially be provided and antiemetic's and antidiarrheals will be administered as ordered.
o Monitor the client for signs of dehydration and skin breakdown.
o Provide good oral care, emotional support and a restful environment.
o The nurse will teach the client:
▪ Utilize nutritional support strategies
▪ During treatment, do not wash marked area
▪ If the area must be cleansed, use only tepid water, no soap
▪ Do not wear tight clothing in the area
▪ Do not expose the area to sunlight
Diagnostic Tests
▪ Do not shave or scratch the area
▪ Do not use creams, lotions or oils on the area
▪ Avoid persons with known infections
▪ Avoid injury to the area
▪ Utilize strategies to conserve personal energy
The nurse will apply their knowledge and psychomotor skills when caring for clients undergoing diagnostic testing. They will be able to identify complications and provide the appropriate action. The nurse is also responsible for identifying normal and abnormal lab values and notifying the health care provider appropriately.
Diagnostic Tests - Cardiovascular
Nurses need a basic understanding of cardiovascular diagnostic tests. The tests are separated into the categories of:
• Laboratory Tests
o Arterial Blood Gases
▪ Measures tissue oxygenation, carbon dioxide removal and acid-base balance.
▪ The nurse will perform an Allen test to check collateral circulation. Arterial blood will be collected in a heparinized syringe because the test requires blood without clots. Air bubbles cannot be present in the specimen.
o (Serum) Enzymes/Cardiac Markers
▪ Creatinine kinase lab results are used to diagnose an acute myocardial infarction (MI) and is detected in the blood within 3-5 hours post MI. Murakami (MM) bands present indicate skeletal muscle damage and the presence of Myocardial B and R (MB) bands indicate heart muscle damage.
▪ Troponin is a regulatory protein found in striated muscle; troponin levels are elevated 4-8 hours after a heart attack. This test is used to diagnose a heart attack and to assess the degree of damage to the heart muscle. There are two different cardiac-specific isoforms: troponin I and troponin T.
o C-reactive Protein (CRP)
▪ CRP is a protein produced by the liver; levels rise with inflammation throughout the body. CRP may help determine the risk of future cardiac events in clients who have had a heart attack. CRP is a simple blood draw and no client preparation is required.
o Lipid Profile
▪ The lipid profile evaluates the risk for atherosclerosis.
▪ The client should take nothing by mouth (NPO) 10-12 hours prior to the blood draw; water is permitted.
▪ Triglycerides detect risks of atherosclerosis
o Brain Natriuretic Peptide (BNP) or N-terminal pro-BNP
▪ The BNP is used to measure the production of a hormone found in the left ventricle and helps diagnose and evaluate the client's risk of future cardiac events, including heart failure.
▪ It is used for prognosis and to monitor therapy.
▪ Normal range is 0.5-30 pg/mL.
• Scans and X-Rays
o Computed Tomography (CT)
▪ The CT test provides a three-dimensional assessment of the thorax
(lungs, heart, bones and tissue).
▪ This test may also detect fractures not visible in an X-ray.
▪ It is non-invasive and painless and typically takes around 20 minutes. If contrast dye is used and a reaction occurs, the nurse will monitor the
reaction.
o Magnetic Resonance Imaging (MRI)
▪ The MRI provides a detailed image of the body structures.
▪ It can be used to diagnose a heart issue but can also be used to diagnosis abnormalities in other systems.
▪ The nurse will explain the procedure and assess the client for claustrophobia and verify whether the client has any metal implants (e.g., pacemaker, screws).
• The client will remove all metal jewelry and objects.
o Nuclear Scan
▪ Before a nuclear scan, a radioactive material is injected.
▪ The scan charts the flow through the client's heart and lungs. The nurse will monitor the client for allergic reaction.
o Radiographs (X-Rays)
▪ A chest X-ray is used to detect malfunctions within heart and lung physiology.
▪ The client will remove jewelry from neck and chest and female clients will wear a lead apron.
• Diagnostic Procedures
o Angiogram (Cardiac Catheterization)
▪ An angiography is used to evaluate specific areas of the arterial system by injecting a dye through a catheter (via the groin or arm) that makes coronary arteries visible on an X-ray.
▪ An angiogram is performed with the use of local anesthesia and intravenous sedation and takes approximately 20-30 minutes.
▪ If a blockage is found during the procedure, the surgeon may perform a percutaneous coronary intervention (PCI) to open the blockage.
▪ The client will need to sign a consent form, and then empty their bladder prior to the test.
▪ The nurse will assess pulse rate and explain to the client that some people feel heat, palpitations or like they need to cough when the dye is injected.
▪ Clients who have the catheter inserted in their groin will have a compression bandage on the site and must lie flat on their back for several hours post-procedure.
▪ The nurse will assess for a hematoma, distal pulses and vital signs frequently post-test.
▪ The nurse will also compare the client's skin temperature, color and sensation in both extremities and notify the provider if bleeding or vital signs change. Check your organization's policy on post-cardiac catheterization orders.
• Persons with diabetes and/or impaired kidney function are at high risk for developing contrast media-induced nephrotoxicity (CIN). Adequate hydration helps maintain renal blood flow and reduces the time the contrast media is in contact with the renal tubules and, therefore, will help prevent CIN. Serum creatinine levels are used to monitor for the development of CIN. Nephrotoxic drugs, such as ibuprofen, should not be used for procedures requiring contrast media. The oral hypoglycemic drug metformin increases the risk of lactic acidosis if CIN were to occur; it should be held the day of the procedure until kidney function returns to baseline (as determined by serum creatinine).
o Electrocardiogram (ECG)
▪ A 12-lead ECG takes about 10 minutes to perform at the bedside.
▪ With each beat, an electrical impulse travel through the heart.
▪ The P-wave is the impulse of the atria, followed by a flat line when the
electrical impulse goes to the bottom of the chambers. The QRS
complex is the impulse of the ventricles and the T-wave represents the electrical recovery or return to a resting state for the ventricles.
o Ultrasound Echocardiogram
▪ Non-invasive sound waves are used to diagnose and monitor heart failure,
differentiating between systolic and diastolic heart failure.
o Exercise Cardiac Stress Test (ECST)
▪ An ECST is used to assess the cardiovascular response to increased workload.
▪ It measures how heart and blood vessels respond to exertion.
▪ The client may walk on a treadmill or pedal a stationary bicycle with continuous ECG monitoring.
o Radionuclide Stress Testing (Nuclear Stress Test)
▪ During this test, a radioactive isotope (typically thallium or cardiolite) is injected into the client and nuclear images of the client's heart are taken, first during rest and then following exercise.
▪ A blockage in a coronary artery results in diminished blood flow, which shows up as a "cold" spot on the scan.
o Hemodynamic Monitoring
▪ Hemodynamic monitoring uses an invasive balloon-tipped, flow-directed cardiac catheter to provide continuous monitoring.
▪ Readings reflect left ventricular end diastolic pressure.
▪ Complications include
• pneumothorax, dysrhythmias, infection, sepsis and thrombophlebitis.
▪ The nurse will monitor pressures, assess and change dressings and maintain patency with the fluids. Strict asepsis and standard precautions are required.
o radiofrequency catheter ablation
▪ Clients with AF who are unresponsive to antiarrhythmics or electrical cardioversion can be treated by radiofrequency catheter ablation. The procedure, which is usually performed under conscious sedation, destroys any abnormal pacemaker cells so that erratic electrical signals are normalized. Sometimes more than one ablation is needed. After an ablation, the client will need to continue taking an anticoagulant and even antiarrhythmic medication.
Diagnostic Tests Diagnostic Tests - Urinary
Urinary diagnostic tests are separated into the categories of:
• Normal Values
Category Normal Values
Negative
Acetone
Category Normal Values
None or less than 1000/mL
Bacteria
Category Normal Values
None
Bilirubin
Category Normal Values
None to few
(Granular) Casts
Category Normal Values
110-250 mEq/24 hour
Chloride
Category Normal Values
Color Pale yellow
Normal Values
Men: 90-140 mL/min
Women: 85-125 mL/min
Category
Creatinine clearance
Category Normal Values
None
Crystals
Category Normal Values
Less than 0.5 grams/day
Glucose
Category Normal Values
None/negative
Ketones
Category Normal Values
7.4-12.2 HPF
Magnesium
Category Normal Values
Specific aromatic odor, similar to ammonia
Odor
Category Normal Values
500-800 mOsm/L
Osmolality
Category Normal Values
4.5-7.8
pH
Category Normal Values
Negative
Phenylketonuria
Category Normal Values
25-125 mEq/24 hour
Potassium
Category Normal Values
Negative
Protein
Category Normal Values
Less than 33 cells/high-powered field
Red Blood Cells
Category Normal Values
40-220 mEq/24 hour
Sodium
Category Normal Values
Specific Gravity 1.016-1.022
Category Normal Values
Less than or equal to 4 cells/high-powered field
White Blood Cells
Category Normal Values
3-7 mg/dL (or 250-750 mg/24 hour)
Uric Acid
Category Normal Values
0.5-1 mg/dL
Urobilinogen
• Laboratory Tests
o Urine Culture & Sensitivity
▪ Used to identify bacteria in the urine. The client will cleanse their external meatus and provide a midstream specimen.
▪ Normal levels are less than 100,000 colonies/mL.
o Creatinine Clearance (CC)
▪ CC is used to evaluate renal function.
▪ A 24-hour urine collection and a blood draw for a creatinine level at the end of the urine collection.
▪ Normal levels are between 1.42-2.08 mL/min.
o Blood Urea Nitrogen (BUN)
▪ The BUN is also collected to evaluate renal function. Values are affected by the client's protein intake, tissue breakdown and fluid volume changes.
▪ Normal levels are between 10-20 mg/dL (3.6-7.1 mmol/L).
o Schilling Test
▪ A Schilling test is used to diagnose vitamin B12 deficiency (pernicious anemia).
▪ A radioactive vitamin B12 is administered to the client.
• A low value excreted in the urine indicates pernicious anemia.
▪ Normal is greater than 10% of the dose excreted in 24 hours.
• Scans and X-Rays
o Renal Scan
▪ A renal scan is an evaluation of the kidneys.
▪ A radioactive isotope is injected via an IV and the radioactivity is measured by a radioactivity counter. T
▪ The nurse must help the client force fluids prior to the test.
o Ultrasound
▪ An ultrasound can provide images of the renal structures via sound waves.
▪ It is a non-invasive exam.
▪ The client must have a full bladder during the test.
▪ An ultrasound can provide images of structures in all of the body's systems.
• Diagnostic Procedures
o Cystometrogram
▪ Used to test the muscle tone of the bladder.
▪ The nurse will insert a Foley catheter. Let your client know that they will feel pressure during the test when saline is instilled into the bladder.
o Cystoscopy
▪ A cystoscopy provides direct visualization of the bladder and urethra.
▪ There is a bowel preparation the client must complete prior to the test.
▪ Before the test is administered, the nurse will encourage the client to be NPO if a general anesthetic is going to be used.
• The nurse will teach the client to breathe deeply during times of discomfort.
▪ Post-test, the nurse will monitor the character and volume of the urine and check for abdominal distention, urinary frequency and fever.
• Urine is typically pink in color after the exam.
• If the client experiences abdominal or pelvic pain post exam, it may indicate trauma.
• The nurse will also provide antimicrobial prophylaxis as ordered.
o Cystourethrogram
▪ A cystourethrogram is an X-ray or the bladder and urethra.
▪ A catheter will be inserted into the urethra and a radiopaque dye will be injected.
• The client will then void and X-rays will be taken.
o Intravenous Pyelogram (IVP)
▪ This test provides an X-ray visualization of the kidneys, ureters and bladder.
▪ A bowel preparation is required, and the client will be NPO after midnight.
▪ Assess client for iodine sensitivity to avoid an anaphylactic reaction.
▪ During the injection of the radiopaque dye into the vein, the client may experience burning in the vein or a salty taste in their mouth, which is
normal.
• X-rays are taken at intervals after the dye is injected.
▪ X-rays are typically taken after the test as well. The client should be aware of and report any signs of a dye reaction, which include edema,
itching, wheezing and SOB.
o Kidney Biopsy
▪ In a kidney biopsy, tissue is obtained via a needle aspiration.
▪ The client must be NPO 6-8 hours prior to the biopsy.
▪ An X-ray is taken before the procedure and the skin is marked to indicate the lower pole of the kidney.
Diagnostic Tests
▪ The client will be in the prone position.
• Instruct clients to hold their breath during the needle insertion.
▪ Pressure will be applied to the site for 20 minutes and the client will be
kept on the affected side for 30-60 minutes.
▪ A pressure dressing will be applied and vital signs will need to be
checked every 15 minutes for the first hour.
▪ The nurse will observe for hematuria and site bleeding.
▪ The client will be on bedrest for 6-8 hours and kept flat in the bed. The client's intake should be increased as well.
Diagnostic Tests - Gastrointestinal
Gastrointestinal diagnostic tests are separated into the categories of:
• Laboratory Tests
o Alpha-fetoprotein (AFP) Tumor Markers
▪ Used to diagnose and monitor therapy for some cancers of the liver.
▪ This is a simple blood test and no special client preparation is needed.
o Amylase
▪ Amylase is typically ordered with a lipase test to help diagnose and
monitor acute chronic pancreatitis.
▪ The client will restrict food for 1-2 hours before the test and avoid opiates for two hours before the test.
• Normal value is 23-85 u/dL.
o Ammonia
▪ Ammonia levels are used primarily to investigate the cause of changes in behavior and altered levels of consciousness due to severe liver disease and used to support a diagnosis of Reye's syndrome.
▪ Instruct your client to refrain from smoking for several days prior to the collection of the sample.
• Normal value is 15-45 mcg/dL (11-32 mcmol/L).
o Bilirubin
▪ A bilirubin level is used to detect the presence of bilirubin due to hemolytic or liver disease.
▪ The test is a simple blood draw and no client preparation is needed.
▪ For infants, the nurse will perform a heel stick.
o Fecal Occult Blood (also known as Guaiac Smear Test)
▪ Fecal occult blood (also known as a Guaiac smear test) is used to screen for lower GI bleeding, which may indicate colon cancer.
▪ This test is part of routine examination to begin at age 50, unless family history of colon cancer exists.
• Usually the test involves taking samples of three different stool samples on three different days.
▪ Leading up to the test, clients should avoid
• eating red meat (w/n 3 days
• turnips, cauliflower, broccoli, bananas, cantaloupe, beets, drinking alcohol
• taking NSAIDs (ibuprofen/naproxene)
• corticosteroids (can cause gastric irritation, including peptic ulcer)
• taking vitamin C.
▪ Females should not collect a stool sample during their menstrual period. Instruct her to wait until after her period has stopped.
o Lipase
▪ Lipase levels are used to diagnose acute and chronic pancreatitis, biliary obstruction, hepatitis and cirrhosis. It is usually ordered with serum amylase.
• Normal value is 0-160 U/L.
o Liver Enzyme Tests
Standard liver enzyme tests include:
▪ Serum albumin levels are used to detect protein malnutrition.
• Normal levels are between 3.5-5.5 g/dL.
▪ Alanine transaminase (ALT) will increase with liver disease/hepatitis.
• Normal levels are between 10-40 units.
▪ Aspartate aminotransferase (AST) will increase with liver disease/hepatitis.
• Normal levels are between 10-40 units.
▪ Alkaline phosphatase evaluates liver and bone function.
• The client should be NPO (nothing by mouth) for 8-12 hours prior to the test.
• A list of client medications should be sent to the lab with the sample.
o Normal values are 0-120 units and 104 FU/L in children and adolescents.
o Prothrombin Time (PT)
▪ PT, also known as pro time or international normalized ratio, is used to determine how well anticoagulants are working and to diagnosis bleeding disorders.
▪ A client's PT may be prolonged in hepatic disease.
• Normal PT is 9.5-12.0 seconds.
• The specimen will be put on ice and pressure applied to the site for five minutes, or fifteen minutes if the client is on
anticoagulant.
o Partial Thromboplastin Time
▪ PTT is used to investigate a bleeding or thrombotic episode.
▪ It monitors the effectiveness of heparin therapy and detects coagulation disorders.
▪ In liver disease, PTT is prolonged due to lack of vitamin K.
o Stool Cultures
▪ Stool cultures are primarily used to identify pathogenic bacteria in the GI tract, e.g., salmonella, shigella, campylobacter, E. coli 0157:H7, usually when there is prolonged or severe diarrhea.
▪ Stool cultures can also be used to check for white blood cells (WBC) and toxins.
▪ Instruct your clients that a fresh stool sample is needed, and to be careful
not to contaminate the sample(s) with urine or menses.
o Ova & Parasite
▪ The ova and parasite test is used to determine if a stool sample contains parasites or ova that are associated with intestinal infections, e.g., amebiasis, giardiasis.
o Qualitative Fecal Fat Test
▪ A qualitative fecal fat test checks for poor absorption of nutrients by the digestive tract (also known as malabsorption syndrome).
▪ Stool is collected over a 72-hour period and checked for fat and meat fibers.
▪ For one to two weeks prior to the test, clients may need to stop taking medications such as antacids, antidiarrheal medications, anti-parasite medications, antibiotics, enemas, laxatives or NSAIDs.
• Scans and X-rays
o Liver Scan
▪ A liver scan is used to evaluate the size and shape of the liver.
▪ The scan is also a way to visualize scar tissue, cysts or tumors.
• A radiopaque dye is also used during the exam.
▪ Be sure to ask your client about allergies and previous iodine sensitivity
prior to the administration of the radiopaque dye.
▪ The client must be monitored for anaphylaxis.
• An aqueous-based dye is available for clients who are
hypersensitive.
o Splenoportogram
▪ This test is used to determine the adequacy of the portal blood flow and also uses a contrast media of organic iodine.
▪ Assess the client for allergies and previous iodine sensitivity to avoid possible allergic reactions.
• Diagnostic Procedures
o Gastric Aspirate
▪ Gastric aspirate is used to evaluate the presence of blood, abnormal bacterial, pH or malignant cells.
▪ The client is NPO before the test.
▪ A nasogastric (NG) tube is inserted and the client's stomach contents are aspirated out.
▪ Histamine can sometimes be given to stimulate hydrochloric acid
secretions.
• The nurse will encourage fluids post-test.
o Upper GI Series (Barium Swallow)
▪ Clients will ingest barium sulfate to determine patency and size of esophagus, size and condition of gastric walls and patency of pyloric valve.
▪ This test also can determine the rate passage to small bowel.
▪ The nurse will encourage clients to drink fluids and provide laxatives to prevent constipation.
• Explain to clients that their stool will be white from the barium.
o Lower GI Series (Barium Enema)
▪ Barium is instilled into the colon via the rectum for fluoroscopy X-rays to view for tumors, polyps, strictures, ulcerations, inflammation or obstruction of the colon.
▪ The client must stay on a low-residue diet for 1-2 days prior to the test.
▪ The client will be on a clear liquid diet and take a laxative the evening before the test.
▪ The client will use a cleansing enema until they are clear the morning of the test.
▪ The nurse will administer cleansing enemas after the exam to remove barium and prevent impaction.
• X-rays may be repeated after all the barium has left the body.
o Paracentesis
▪ A paracentesis is a needle aspiration of fluid from the abdominal cavity used for diagnostic examination of the ascetic fluid and the treatment of ascites.
▪ This procedure is done at the bedside.
▪ The client will be in a semi-Fowler's position.
▪ Tell the client to empty the bladder prior to the procedure to avoid an accidental perforation.
o Endoscope
▪ Prior to the endoscopy, the nurse will verify that clients have signed the
informed consent form and has been NPO for at least eight hours.
▪ The nurse will let clients know they may experience throat numbness afterwards, due to the anesthetic spray or the gargle they will do before the procedure.
▪ The nurse will monitor clients post-procedure for vobmiting of blood or respiratory distress.
▪ Clients will remain NPO until the nurse is able to verify a gag reflex.
▪ Clients can expect to have an irritated throat for a few days post- procedure.
o Cholecystogram & Cholangiography
▪ These exams are conducted to visualize the gallbladder and bile duct.
▪ A radiopaque material is injected directly into the biliary tree.
▪ Advise your client to refrain from fatty foods the night before the test.
▪ The dye is in a tablet form and should be ingested the evening before (assess client allergies first).
• The client will be NPO after the tablet is taken.
o Liver Biopsy
▪ A sample is taken via a needle aspiration.
▪ The client must be NPO for at least six hours prior to the test.
▪ Prior to the biopsy, vitamin K will be administered intramuscularly
(IM) to decrease the chance of hemorrhage.
▪ A sedative is also administered prior to the biopsy.
▪ Clients will be in a supine position, lateral with arms elevated. Clients will be asked to hold their breath for 5-10 seconds while the biopsy is
being obtained.
▪ Clients will be positioned on their right side for three hours post-test.
▪ It is a priority to check vital signs frequently to evaluate for hemorrhage and shock.
▪ Clients should expect mild local pain that may radiate to the right shoulder.
▪ Clients should report any abdominal pain immediately (may indicate a perforation) and avoid heavy lifting for at least one week.
o Celiac Axis Arteriography
▪ Used for liver and pancreas visualization.
▪ This test uses a contrast media of organic iodine, so evaluate the client's allergies and sensitivity to iodine.
▪ Anaphylaxis during this test is common.
Diagnostic Tests
Diagnostic Tests - Respiratory
The following section is about respiratory diagnostic tests. The tests are separated into the categories of:
• Laboratory Tests
o Arterial Blood Gases (ABG)
▪ See normal values under cardiovascular system.
o Blood Cultures
▪ Usually 2-3 blood samples are collected at timed intervals and/or from different veins.
▪ These samples are placed in culture bottles to grow both aerobic and anaerobic specimens to determine causative agent and potential treatment.
o Sputum Analysis
▪ A sputum analysis is used to identify the cause of a pulmonary infection.
• It is also used to determine abnormal lung cells.
▪ The nurse will encourage fluid intake the night before the test.
▪ The collection should take place in the morning if possible.
▪ The client will rinse their mouth with water prior to test.
• Instruct your client not to brush their teeth, eat or use mouthwash before the test.
o Acid-fast Bacillus (AFB) Smear & Culture
▪ This test is used to identify a causative agent for tuberculosis and monitor the effectiveness of treatment.
▪ Usually three sputum samples are collected, early in the morning.
▪ Clients can rinse their mouth with plain water (no mouthwash).
▪ The difference between sputum and spit should be emphasized. A
sample may be collected on three different days.
• Scans and X-rays
o Chest X-ray (CXR)
▪ A chest X-ray is a non-invasive, painless exam used to evaluate the lungs.
o Computed Tomography (CT)
▪ This is a non-invasive, painless process that produces two-dimensional images of organs, bones and tissues.
▪ It takes about 20 minutes and occasionally a contrast dye is used.
▪ Although very little radiation is used, pregnant women should avoid the test.
o Magnetic Resonance Imaging (MRI)
▪ A chest MRI can provide detailed information to diagnose lung problems such as a tumor or pleural disorder, blood vessel problems or abnormal lymph nodes.
▪ Chest MRI can help explain the results of other imaging tests such as chest X-rays and chest CT scans.
▪ Clients may feel claustrophobic inside the MRI unit.
▪ Clients must remove all metal prior to the test; MRI cannot be used on
clients with metal implants.
o Nuclear Lung Scanning
▪ This test is useful in diagnosis of conditions such as pulmonary embolus, lung infection or inflammation.
▪ It uses minute amounts of short-lived, radioactive materials to depict
the flow of air and blood in the lungs.
▪ It may be done in two states: a lung perfusion scan and then a lung ventilation scan.
o Positron Emission Tomography (PET)
▪ A PET is used when cancer is suspected.
▪ This radiographic imaging technique differentiates metabolic rate differences in malignant and benign tissues.
o Pulmonary Artery Angiography
▪ This test is used to detect narrowing, blockages and vessel malformation in the arteries.
▪ A radiopaque dye is injected into the pulmonary artery and conventional X-rays are used to view the dye in the lungs. (An allergy assessment is required before the testing.)
o Ultrasound
▪ During an ultrasound, part of the body is exposed to high-frequency sound waves to produce pictures of inside the body.
▪ An ultrasound of the chest can be used to assess the lungs.
▪ Conventional ultrasound displays images in thin, flat sections; 3-D formats are now available.
▪ Clients may need to be NPO 12 hours before the exam
▪ A Doppler ultrasound evaluates blood velocity as it flows through a blood vessel.
• A clear, water-based gel is applied to the area of the body being studied to help the transducer make secure contact with the body and eliminate air pockets between the transducer and the skin.
o Lung Scan
▪ A lung scan is used to evaluate pulmonary perfusion when pulmonary infraction or space-occupying disorders are suspected.
▪ A perfusion scan is done via an intravenous injection of iodinated radioactive dye (allergies must be assessed).
▪ A high level of radioactivity = good perfusion.
▪ Low levels of radioactivity = obstructed areas.
▪ A ventilation scan uses radioactive gas that is inhaled by the client. The gas should be equal in distribution.
o Lung Biopsy
▪ A piece of lung tissue is removed for a culture and/or cytology.
▪ The nurse will administer pre-meditcation sedatives or analgesics as ordered.
▪ The client will hold their breath in mid-expiration. T
• The biopsy is performed with a fluoroscopic monitoring.
▪ The nurse will monitor vital signs and breath sounds every four hours for 24 hours.
• A sterile dressing will be applied post-biopsy.
• The client will report any signs of respiratory distress.
• A chest X-ray is taken after the procedure to check for a pneumothorax.
• Diagnostic Procedures
o Mantoux Test
▪ The Mantoux test or Purified Protein Derivative Standard (PPD) is used to determine exposure to and infection with Mycobacterium tuberculosis.
▪ It is administered via an intradermal injection of a small amount of purified protein derivative (PPD) solution.
▪ Readings of the reaction, if any, are taken 48-72 hours after the injection.
A positive result is when the injection site is red and swollen.
▪ False positive results may occur in individuals who have received a Bacille Calmette-Guerin (BCG) vaccination.
o Radioallergosorbent Test (RAST): Alllergy Skin Test
▪ RAST is used to identify measurable allergen-specific antibodies, e.g., IgE.
▪ It tests for reactions to certain respiratory and food allergy stimulants.
▪ It is a simple blood test and no special prep is needed.
o Pulse Oximetry
▪ This test measures oxygenation saturation through the skin or finger.
▪ Clean the site and remove nail polish if possible.
• Normal value ranges from 95-100%.
o Bronchoscopy
▪ Bronchoscopy is a direct visual examination of the larynx and airways using a bronchoscope.
▪ This test is usually used to investigate source of bleeding in the lungs and is also used to treat certain conditions, i.e., remove secretions, blood, pus and foreign bodies or to place drugs in specific areas of the lung.
▪ Clients should be NPO at least four hours before the procedure and in most cases a sedative is given as well as a local anesthetic.
▪ Clients may experience a sore throat post-test.
▪ Clients will be asked to sit or lie on their side and remain NPO until the gag reflex returns.
• The nurse will monitor for respiratory difficulties.
o Needle Biopsy
▪ This test is the next step to take when a thoracentesis does not uncover the cause of a pleural effusion.
▪ The health care provider uses a cutting needle to take a small sample of the pleura for biopsy; often a CT is used for guidance.
o Pulmonary Function Testing (PFT)
▪ PFT measures the lungs' capacity to hold air, move air in and out and to exchange oxygen and carbon dioxide.
▪ Remind your clients to refrain from smoking four hours prior to the test.
▪ They may also be asked to withhold bronchodilator medication.
o Thoracentesis
▪ Fluid from pleural space is removed for diagnostic testing or to relieve shortness of breath.
▪ The nurse will obtain a set of vital signs before the test is performed.
▪ The client will be asked to sit at the side of the bed and lean forward.
▪ A local anesthetic is used prior to the needle insertion.
▪ The client may feel some pain as the lung fills with air and expands against the chest wall.
▪ The client may need to cough, feel light-headed and/or short of breath during and/or after the procedure.
• No more than 1,000 mL should be removed at one time.
▪ The nurse will monitor breath sounds and vital signs frequently.
▪ They should also monitor for leakage of fluid at the puncture site.
▪ A sterile dressing will be applied after the test.
• A chest X-ray may be ordered if complications are suspected.
o Peak Flow Meter for Asthma
▪ move the indicator to the bottom of the numbered scale,
▪ stand up, take a deep breath, place the mouthpiece in mouth and close lips around it, blow out hard and fast with a single blow
▪ record the number achieved on the indicator
▪ The steps should be repeated two more times, for a total of three attempts and the highest peak flow reading of the three is recorded.
Disorder Diagnostic Tests Diagnostic Tests - Sleep
• Nurses may participate in sleep disorder diagnostic tests.
• Sleep studies are used to detect sleep apnea.
o They are usually combined with electroencephalogram (EEG) and pulse oximetry.
• (EEG) + (pulse oximetry) + (sleep study) = polysomnography. Diagnostic Tests
Diagnostic Tests - Neurological
Neurological diagnostic tests are separated into the categories of:
• Scans and X-rays
o Computed Tomography (CT)
▪ CT can be used to detect hemorrhage, fractures, abscesses and tumors.
▪ Informed content must be obtained.
▪ The test is painless, but the client must remain immobile during the exam, which can cause anxiety.
▪ If contrast dye is used, the client may experience a flushed, warm face and/or a metallic taste during the injection.
▪ The nurse will assess for allergic responses to contrast dye such as rash, itching or urticarial.
• The nurse will encourage fluids post-test.
▪ People at higher risk for a reaction include those with past reactions to contrast media, asthma, and a history of heart, kidney and
thyroid diseases.
▪ Individuals taking beta blockers or metformin are also at higher risk.
▪ Clients with poor renal function will not be able to clear the contrast agent from the kidneys
• Cisternography
o Cisternography, also called intrathecal contrast-enhanced CT scan, is used to
detect problems with the spine and spinal nerve roots.
o It is usually performed at an imaging center.
o A small sample of spinal fluid is removed via lumbar puncture.
o The sample is mixed with a contrast dye and injected back into the spinal sac.
o CT is used to obtain two-dimensional images.
o The test may take up to an hour to complete. Clients may experience some discomfort and/or headache following the test. Allergies must be assessed.
• Magnetic Resonance Imaging (MRI)
o An MRI can be used for imaging the brain (soft tissues). Clients may feel
claustrophobic inside the MRI unit.
o They must remove all metal prior to the test. MRI cannot be used on clients with metal implants.
• Positron Emission Tomography (PET)
o A PET provides two- and three-dimensional pictures of brain activity by
measuring radioactive isotopes that are injected into the bloodstream.
o It is used to assess metabolic and physiological function of the brain.
▪ It is used to diagnose stroke, brain tumor, epilepsy, Parkinson's disease
and head injuries.
▪ A PET may be ordered as a follow-up to a CT or MRI.
o The client inhales or is injected with a radioactive substance and then
scanned.
o The client must lie still while overhead sensors detect gamma rays in the body's tissues. The client may also experience dizziness and headaches, during and post-test.
o Before the test begins, the nurse may teach the client relaxation techniques.
▪ The length of the test depends on the body part being scanned.
• Diagnostic Procedures
o Cerebral Angiography
▪ This test is used to detect blockages of the arteries or veins.
• It can diagnose aneurysms, vascular malformations and brain tumors.
▪ This test can take up to three hours, followed by a 6-8 hour resting period.
▪ While the client is awake, a physician anesthetizes a small area of the leg near the groin, inserts and threads a catheter into an artery in the neck.
▪ A small capsule containing a radiopaque dye is passed over the guide wire to the site of release. A series of X-rays are taken. Clients may feel a warm-to-hot sensation or slight discomfort as the dye is released.
o Biopsy
▪ A biopsy is the removal and examination of a small piece of tissue from the body.
▪ Muscle or nerve biopsies are used to diagnose neuromuscular disorders.
▪ Brain biopsies require surgery, involve risk and a recovery period.
▪ Informed consent is necessary.
o Lumbar Puncture (LP)
▪ An LP is the insertion of a needle into the subarachnoid space to obtain a specimen, relieve pressure or inject dye or medication. The spinal fluid can be tested for blood, diagnose infection, measure intracranial pressure or identify other neurological conditions.
▪ The appearance of fluid is normally colorless, clear and almost entirely free of cells.
• Normal pressure is typically 50-180 mm H2O.
▪ Position your client on one side in a fetal position with knees close to the chest, or they may lean forward while sitting on a table or bed.
▪ A local anesthetic is injected in the puncture site.
• (Client will feel a stinging sensation.)
▪ Once the anesthetic has taken effect, about three teaspoons of fluid are removed; clients may report a sensation of pressure as the needle is
inserted.
▪ After the LP, instruct your client to lay flat for several hours to minimize headache, which often occurs post-test.
▪ Analgesics can be administered as ordered for the headache pain.
▪ The nurse will apply a sterile dressing to the site, preform a neurological assessment every 15-30 minutes until the client is stable
and push fluids.
o Electroencephalography (EEG)
▪ An EEG is a painless test that measures electrical activity in the brain.
▪ Clients should avoid caffeine intake and prescription medications that affect the nervous system prior to the test.
▪ A series of cup-like electrodes are attached to the scalp.
• Clients are exposed to a variety of external stimuli, i.e., bright or flashing light or noise, and are asked to open and close their
eyes or to change breathing patterns.
▪ Clients usually recline in a chair or on a bed during the test and it may take up to an hour; if it is used during sleep, it can take around three hours. After the test, the nurse will remove paste from the scalp and hair, administer any medications that were held and observe for seizure activity in seizure-prone clients.
o Electromyography (EMG)
▪ An EMG records electrical activity from the brain and/or spinal column to diagnose nerve and muscle dysfunction and spinal cord disease.
▪ Very fine electrodes are inserted into a muscle. Testing usually lasts about an hour.
▪ Most clients report it is an uncomfortable procedure.
▪ An EMB is usually done in conjunction with a nerve conduction velocity test.
o Electronystagmography (ENG)
▪ ENG is a group of tests used to diagnose involuntary eye movement, dizziness and balance disorders.
▪ Small electrodes are taped around the eyes to record eye movements.
▪ The test is painless.
o Myelogram
▪ A myelogram is used to visualize the spinal column and subarachnoid space. An informed consent form should be signed once the procedure has been explained. Clients will be NPO 4-6 hours prior to the test. Instruct your client to discontinue phenothiazine, CNS depressants and stimulants for 48 hours prior to the test. The nurse will screen the client for an allergy to the dye.
▪ If a metrizamide water-soluble dye is used, the client's head should be raised 30-45 degrees for three hours. A neurological assessment should be done every 2-4 hours, increased fluids should be encouraged, analgesics for a headache can be administered and an assessment of the bladder for distention should be made.
o Echoencephalography
▪ Echoencephalography is used to evaluate brain structures through sound waves. A hand-held transducer is used to record sound waves.
o Intracranial Pressure Monitoring (ICP)
Diagnostic Tests
▪ ICP monitoring is an invasive placement of a monitoring device located in a ventricle, subarachnoid space, subarachnoid bolt or in the epidural.
▪ Changes in intracranial pressure are converted to an electrical impulse by a transducer and displayed on the screen.
• A normal ICP reading is 10-15 mmg/Hg.
▪ The nurse must maintain strict sterile technique and maintain the
patency of the monitoring device.
• Observe for cerebral spinal fluid leaks (CSF) or signs of infection and report any pressure deviations.
Diagnostic Tests - Musculoskeletal
Musculoskeletal diagnostic tests may be separated into the categories of:
▪ Laboratory Tests
o Antinuclear Antibodies (ANA)
▪ ANA is used to screen for certain autoimmune disorders, such as systemic lupus erythematosus (SLE), Sjogren's syndrome and scleroderma. It is a blood draw and no client preparation is needed. The ANA is often ordered with an ESR and CRP.
▪ ANA tests are performed using different assays (indirect immunofluorescence microscopy or by enzyme-linked immunosorbent assay-ELISA) and results are reported as a titer.
o Alkaline Phosphatase
▪ Alkaline phosphatase measurement is used in the management of Paget's disease and osteoporosis.
▪ The test is a blood draw and fasting is preferred but not required. The test is usually is part of a routine liver panel.
o Calcium
▪ A calcium test can be done via a blood draw but can also be part of a urine collection (where a timed collection is best, e.g., 24-hour urine sample). Blood and urine results are not interchangeable.
o C-reactive Protein (CRP)
▪ CRP is produced by the liver; levels rise with inflammation throughout the body.
• Normal CRP levels are below 3.0 mg/dL.
o Creatinine Kinase (CK)
▪ A creatinine kinase test is a blood draw and no special preparation is required. Levels of creatinine kinase are increased when there is widespread ongoing destruction of muscle.
▪ The normal value for CK-MB is 3-5% of total CK, but peak CK-MB level can range from 15-30% of total CK in post-myocardial
infarction
Levels of 24-hour urine creatinine are evaluated with blood levels as part of a creatinine clearance test.
o Erythrocyte Sedimentation Rate (ESR)
▪ ESR is increased when inflammation is present. It is a blood draw and no special preparation is required.
• The normal range is 0-22 mm/hour for men
• 0-29 mm/hour for women.
o Phosphorus
▪ This test is a blood draw and no special preparation is needed. A timed (24-hour) urine sample may also be ordered.
▪ A normal range for adults is generally 2.5-4.5 mg/dL. The normal range varies slightly depending on your age.
▪ Related tests: calcium, electrolyte panel, PTH and magnesium.
o Potassium
▪ This test is a blood draw and no special preparation is needed.
▪ The normal potassium level in the blood is 3.5-5.0 milliEquivalents per liter (mEq/L).
▪ Related tests: chloride, sodium, bicarbonate (or total CO2), electrolyte panel, BMP, CMP, aldosterone and renin.
o Rheumatoid Arthritis (RA) Factor
▪ This test detects the level of rheumatoid factor (RF) antibody.
▪ It is a blood draw and no special preparation is required.
• The normal reference range for RF is less than 15 IU/mL.
▪ Related tests: ANA.
o Uric Acid
▪ This test is used to detect gout, a form of arthritis.
▪ It is a blood draw and no special preparation is required.
▪ Normal uric acid levels are 2.4-6.0 mg/dL for women and 3.4-7.0 mg/dL for men
▪ Scans and X-Rays
o Bone Scans
▪ Bone scans are used to detect fractures not visible on X-rays; also to
detect bone infection or metastasis.
▪ It involves the use of a radioactive substance (technetium-99m-labelled pyrophosphate) that is absorbed by any healing bone.
▪ It is administered via IV and creates an image that can be viewed on a computer screen.
o Computed Tomography (CT)
▪ This is a non-invasive, painless process that produces two-dimensional images of organs, bones and tissues.
▪ It is used to detect fractures not visible on an X-ray.
▪ This test takes about 20 minutes.
▪ Occasionally a contrast dye is used and, although very little radiation is used, pregnant women should avoid the test.
o Dual-energy X-Ray Absorptiometry (DXA)
▪ DXA is used to screen for or diagnose osteoporosis. Low-dose X-rays are used to examine bone density at the lower spine, hip and wrist.
o Magnetic Resonance Imaging (MRI)
▪ MRI is used for imaging muscles, ligaments and tendons (soft tissues). Clients may feel claustrophobic inside the MRI unit.
▪ Clients must remove all metal prior to the test.
• MRI cannot be used on clients with metal implants.
o Radiographs (X-Rays)
▪ X-rays are used for detecting abnormalities in bones, including fractures, bone pathology and bone density (in advanced cases of osteoporosis).
▪ X-rays may be used to confirm the type of arthritis.
▪ Diagnostic Procedures
o Arthroscopy
▪ During this procedure, a fiber optic scope is inserted into a joint space
and an image is projected on a screen for evaluation.
▪ Either a local, spinal or general anesthetic is used, depending on the
location of the joint.
▪ Tissue can be removed for a biopsy.
▪ This test is usually done in an outpatient setting.
o Joint Aspiration & Analysis
▪ During this procedure, synovial fluid is examined for bacteria or crystals.
▪ It can be performed in a health care provider's office and is usually quick, easy and relatively painless.
▪ There is minimal risk of joint infection post-test.
o Nerve Conduction Studies
▪ Nerve conduction studies measure the speed of impulses that travel through a nerve.
▪ These studies help indicate whether the problem is with the muscles (muscular dystrophy), the nervous system (stroke) or with the neuromuscular junction (myasthenia gravis).
▪ Clients may be startled by the suddenness of the stimulation, but it is not painful.
• The sensation may be similar to the sensation received when one touches a doorknob after walking across carpeting.
Diagnostic Tests
Diagnostic Tests - Endocrine/Reproductive
Endocrine and reproductive tests are separated into the categories of:
• Laboratory Tests
• Fasting ACTH (Adrenocorticotropic Hormone)
o ACTH is used to detect, diagnose and monitor conditions associated with cortisol
in the body, e.g., Cushing's disease (excess ACTH), Addison's disease, ectopic tumor producing ACTH or pituitary insufficiency.
o Clients usually fast the night before and blood sample is usually drawn by or before 8 am. Clients may need to stop taking steroids prior to test. Special handling of blood sample is required.
• ACTH (cosyntropin) Stimulation Test (Test of Adrenal Reserve)
o ACTH stimulation test, also called a test of adrenal reserve, measures how well
the adrenal glands respond to ACTH, which is produced in the pituitary gland. ACTH stimulates the adrenal gland to release cortisol. This test is useful for determining if there are pituitary tumors, low pituitary function, Addison's disease or acute adrenal crisis.
o Draw blood to measure cortisol levels 60 minutes after an ACTH injection. Clients should limit activities prior to the test and eat a high-carbohydrate diet 12- 24 hours before the test. Client may be asked to fast for six hours before the test.
• Aldosterone
o Aldosterone is a hormone released by the adrenal glands and is tested via a blood
draw.
o This test is often used to with other tests to diagnose over- or under-production of aldosterone:
▪ ACTH infusion test
▪ Captopril test
▪ Intravenous saline infusion test
▪ Plasma renin activity
• Cortisol
o Cushing's disease or Addison's disease can affect cortisol levels. A blood sample
is usually drawn at 8 am. (Cortisol levels are highest in the morning.)
o Estrogen and synthetic glucocorticoids (such as prednisone) can affect cortisol levels.
• (Oral) Glucose Tolerance Test (GTT)
o This test is taken while fasting. Clients should be NPO after midnight or 12 hours
prior to the test. Test results may be affected by medications, acute stress and/or vigorous exercise.
o To administer the test:
▪ Blood draw
▪ The client drinks a liquid containing glucose
▪ Blood draw every 30-60 minutes
▪ The test takes up to three hours
• Estrogens: Estrone (E1), Estradiol (E2), Estriol (E3) & Others
o This test is a blood draw and no special preparation is needed. The test can also be part of a urine collection. Blood and urine results are not interchangeable.
o Illnesses such as hypertension, anemia and impaired liver and kidney function can affect estrogen levels. Many medications also affect estrogen levels.
• FSH (Follicle-stimulating Hormone)
o A FSH test is used to determine reason for cessation of menstrual period, loss of
sex drive or infertility. This test is a blood draw. It is often ordered with tests for LH, testosterone, estradiol and progesterone. Results can be affected by medications and the radioisotopes used in a nuclear scan.
• GH (Growth Hormone)
o This test is ordered on clients with symptoms of growth hormone abnormalities,
e.g., precocious puberty, Kallman syndrome; and to evaluate pituitary function.
o The blood sample is either drawn at timed intervals or a single sample of blood is drawn following a fast or after a period of strenuous exercise.
o During timed-intervals testing, either a GH-suppression or -stimulation test is also done:
▪ GH suppression: client drinks standard glucose solution; blood samples are then drawn at timed intervals.
▪ GH stimulation: the client is given an IV solution of insulin or arginine; blood samples are then drawn at timed intervals.
• hCG (Human Chorionic Gonadotropin)
o hCG levels rise rapidly during the first trimester of pregnancy and then slightly
decline. Increased levels may indicate cancer (in both males and females) or the presence of more than one fetus. Decreased levels may indicate fetal death, miscarriage or ectopic pregnancy.
o This test is a blood draw and no special preparation is needed.
• HbA1c
o This test measures the amount of glycated hemoglobin in the blood and provides a
good estimate of how well diabetes has been managed over the past 2-3 months. This test is a blood draw and no special preparation is needed.
o HbA1c level of 6% or less is normal; diabetics should try to keep their HbA1c at or below 7%.
• LH (Luteinizing Hormone)
o This test is used to help determine the reason for loss of menstrual period, loss of
sex drive and infertility. This test is a blood draw.
o For women of childbearing age, the test may need to be done midway through the menstrual cycle, when LH levels peak.
• Progesterone
o This test is used to diagnose infertility, ectopic pregnancy, cancer and multiple
pregnancies. Multiple (serial) measurements are taken to diagnose infertility. Taking estrogen and progesterone supplements can affect test results.
o Other associated tests: FSH, LH, hCG and thyroid tests.
• Prolactin
o Prolactin is usually measured to check for pituitary tumors and the cause of
impotence, infertility, irregular or absent menstrual periods or breast milk. Prolactin production is not related to childbirth.
o This test is a blood draw and no special preparation is needed.
• Parathyroid Hormone (PTH)
o The parathyroid hormone test is used to diagnose the reason for low or high
calcium levels and to help distinguish between parathyroid-related and non- parathyroid-related causes. This test is a blood draw.
o PTH is composed of 84 amino acids (sometimes called PTH 1-84); tests for PTH may measure one or more of the fragments. PTH levels vary during the day, peaking at about 2 am; specimens are usually drawn around 8 am.
o Medications that affect PTH levels include: steroids, isoniazid, lithium, rifampin, anticonvulsants and phosphates.
o Related tests: calcium, phosphate and magnesium.
• Testosterone
o Testosterone is tested to diagnose several conditions in boys (delayed or
precocious puberty), men (change in sex drive, infertility, tumors and erectile dysfunction) and women (hirsutism, infertility and decreased sex drive).
o This test is a blood draw and no special preparation is needed.
o In males, the test is ordered with FSH and LH.
• Thyroid Levels: TSH, T3 (Triiodothyronine), T4 (Thyroxine), Free T4 (FT4) or Free T4 Index (FT4I)
o TSH is produced by the pituitary gland and tells the thyroid gland to make and release the hormones thyroxine and triiodothyronine. TSH can be used to diagnose hyperthydroidism or hypothyroidism, TSH deficiency. Results are impacted by the use of certain medications.
o T3 can be used to diagnose hyperthydroidism or hypothyroidism (Hashimoto's disease) and starvation.
o T4 and Free T4 can also be used to diagnose hyperthydroidism or hypothyroidism, early Hashimoto's disease, Graves disease, tumors, goiters or malnutrition/fasting.
o This test is a blood draw and no special preparation is needed.
o Some medications can affect the tests. The health care provider may discontinue these medications prior to the test.
o Pregnancy and liver disease will falsely raise T3 levels. The free T3 level or T3RU should be ordered if client is pregnant.
• Pregnancy Test or Human Chorionic Gonadotropin (HCG)
o HCG is used to confirm or monitor pregnancy or to help diagnose and monitor
trophoblastic disease or germ cell tumors.
o This test is a blood draw and no special preparation is needed. A urine test can also be performed.
• Progesterone Levels
o This test is used to help determine the cause of infertility, track ovulation, help
diagnose an ectopic or failing pregnancy, monitor the health of a pregnancy or identify the cause of abnormal uterine bleeding.
o This test is a blood draw and no special preparation is needed. Some labs can perform this test on saliva.
• Prostate-specific Antigen (PSA)
o PSA tests screen asymptomatic and symptomatic men for prostate cancer. This
test is a blood draw. It should be done prior to a digital rectal exam or biopsy, or six weeks after manipulation of the prostate.
• Scans and X-rays
o Aldosterone
▪ This test requires a 24-hour urine sample. This test may be preferred by health care providers since plasma aldosterone levels vary throughout the day and are affected by the client's position.
o Catecholamines (see blood test above)
▪ This test is used to diagnose or assess treatment for neuroblastoma and pheochromocytoma (an adrenal gland tumor). This test is taken on a urine sample. Blood and urine results are not interchangeable.
o Glucose Test –- Urine
▪ Glucose is not normally found in the urine. Greater than normal levels may indicate diabetes mellitus or pregnancy. It is taken via urine sample (clean catch) but may also be part of a blood draw. Blood and urine results are not interchangeable.
o Osmolality
▪ This test is performed to determine concentration of particles in urine (particles/kg water). It is taken via urine sample (clean catch).
▪ Drugs that interfere with specific gravity measurements include dextran and sucrose. Clients should eat a normal, balanced diet for several days before the test.
o 17-Hydroxycorticosteroids (17-OHCS)
▪ 17-OHCS is an inactive product formed when the liver and other body tissues break down the steroid hormone, cortisol. Greater-than-normal levels may indicate Cushing syndrome; lower-than-normal levels may indicate adrenal insufficiency or hypopituitarism. A 24-hour urine sample is needed.
o 17-Beta Hydroxysteroid
▪ This test is used to detect congenital adrenal hyperplasia (CAH), a group of inherited disorders caused by specific gene mutations, resulting in ambiguous genitalia, virilization, acne or pubic hair.
▪ It is ordered as part of a newborn screen. It may be used to rule out CAH in older people, particularly girls and women with symptoms such as hirsutism and irregular periods.
• Diagnostic Procedures
o Radioactive Iodine Uptake (RAIU)
▪ RAIU tests thyroid function by measuring how much radioactive iodine is taken up by the thyroid gland in a given time period. The client swallows a liquid or capsule containing radioactive iodine and 6-24 hours later a gamma probe is placed over the thyroid gland. The test takes about 30 minutes.
o Culdoscopy
▪ This test enables the visualization of ovaries, fallopian tubes and uterus via a lighted tube inserted into the vagina. A local anesthetic and/or light sedation is given and the client is in a knee-chest position during the test. The client will be placed on her abdomen after test and the nurse will monitor for vaginal bleeding. The client will not douche or have intercourse for two weeks.
o Colposcopy
▪ This test is similar to a pelvic exam and performed between menstrual periods. A colposcope is used to closely examine the client's cervix, vagina and vulva for signs of disease. A sample of tissue can be collected for diagnostic testing. It is recommend that the client does not have vaginal intercourse, use tampons or use vaginal medications a day or two before the colposcopy. The client can use an over the counter analgesic prior to the procedure.
o Laparoscopy
▪ A laparoscopy is used to visualize the pelvic cavity through an incision beneath the umbilicus to view structures. Carbon dioxide is introduced to enhance visualization. A general anesthetic is used and a Foley catheter is inserted to distend the bladder.
o Cultures & Smears (Pelvic Exam)
▪ Samples of tissues are taken to identify infectious processes or identify abnormal cells. A chlamydia smear does need a media preparation done by the laboratory.
o Cervical Biopsy
▪ A sample is taken to identify unusual cells. No anesthesia is needed; however the client may feel a cramping sensation during or after the test. The client should wait three days to have intercourse, douche or go swimming.
o Breast Biopsy
▪ A small piece of tissue is collected via needle aspiration or surgery. Additional Laboratory Tests
Diagnostic Tests - Additional Diagnostic Tests
The following section is about additional diagnostic tests. The tests are separated into the categories of:
• Laboratory tests
o Activated Partial Thromboplastin Time
▪ This test is used to investigate a bleeding or thrombotic episode or monitor unfractionated (standard) heparin anticoagulant therapy.
▪ This test is a blood draw.
o Basic Metabolic Panel (BMP or Chemistry Panel)
▪ Standard BMP includes eight specific tests: glucose, calcium, electrolytes (sodium potassium, carbon dioxide, chloride and bicarbonate), kidney tests, BUN and creatinine.
▪ This test is a blood draw and may be collected on a random basis or drawn after fasting 10-12 hours prior to the blood draw. When more information is needed, a complete metabolic panel (CMP) may be ordered.
o Normal Values:
▪ BUN: 7-20 mg/dL
▪ CO2 (carbon dioxide): 20-29 mmol/L
▪ Creatinine: 0.8-1.4 mg/dL
▪ Glucose: 64-128 mg/dL
▪ Serum chloride: 101-111 mmol/L
▪ Serum potassium: 3.7-5.2 mEq/L
▪ Serum sodium: 136-144 mEq/L
o Red Blood Cell Count (RBC), White Blood Cell Count (WBC)
▪ RBC determines the actual number of cells in relation to the volume. Normal level should be 4.6-6.2 million/mm3 for men and 4.2-5.4 million/mm3 for women.
▪ WBC establishes the amount and maturity of the WBC. 4,5000-11,000 is the normal level for a healthy adult.
o Complete Blood Count (CBC)
▪ Typically there are no specific pre-testing restrictions for a CBC, although the client should avoid eating a fatty meal prior to the test.
▪ Normal CBC Levels:
• Red blood cell count:
o Male: 4.32-5.72 trillion cells/L* (4.32-5.72 million cells/mcL**)
o Female: 3.90-5.03 trillion cells/L (3.90-5.03 million cells/mcL)
• Hemoglobin:
o Male: 13.5-17.5 grams/dL*** (135-175 grams/L)
o Female: 12.0-15.5 grams/dL (120-155 grams/L)
• Hematocrit:
o Male: 38.8%-50.0%
o Female: 34.9%-44.5%
• White blood cell count 3.5-10.5 billion cells/L (3,500 to 10,500 cells/mcL)
• Platelet count 150-450 billion/L (150,000 to 450,000/mcL**)
o D-dimer
▪ This test is ordered to help diagnose or rule out thrombotic diseases and conditions.
▪ This test is a blood draw and no special preparation is needed.
▪ An increased D-dimer test following a partial abruption raises the concern of disseminated intravascular coagulation
o Hemoglobin
▪ This test determines the amount of hemoglobin/100 mL of blood.
▪ Normal levels for men are 13-18 g/dL and 12-16 g/dL for women (130-180g/L for men and 120-160g/L for women).
o Hematocrit
▪ This test measures percentage of RBC per fluid volume of blood. Normal levels for men are 42-52% and 35-47% for women (0.42-0.52 for men and 0.35-0.47 for women)
o Bleeding Time
▪ This test measures the duration of bleeding after a standardized skin incision. It can be used for preoperative screening.
▪ A normal bleed time is 1.5-9.5 minutes.
o Platelet Count
▪ This test is used to diagnose hemorrhagic diseases and thrombocytopenia.
▪ Normal levels are 150,000-450,000/mm3.
o Prothrombin Time (PT)
▪ This test monitors the effectiveness of warfarin therapy and detects coagulation disorders.
▪ Normal levels are between 9.5-12.0 seconds.
o International Normalized Ratio (INR)
▪ This test monitors the effectiveness of anticoagulation therapy.
▪ A normal level is 1.0 in healthy adults.
▪ An expected level is 2-3 for clients with atrial fibrillation, deep venous thrombosis and pulmonary embolism. The expected level is 2.5-3.5 for clients
with prosthetic heart values.
o Platelet Aggregation (Platelet Function Assay)
▪ This test is used to help determine the cause of or potential for excessive bleeding, to monitor and evaluate platelet function and monitor presence and effectiveness of antiplatelet medication.
▪ This test is a blood draw. The client should not take medications that could interfere with the test, e.g., aspirin and other NSAIDs.
o Sedimentation Rate (ESR)
▪ This test evaluates the speed at which the RBCs settle in well-mixed venous blood. High levels indicates inflammation.
▪ In men aged 49 or younger, normal values are at or below 15 mm/h.
▪ In men aged 50 or older, normal values are at or below 20 mm/hr.
▪ In women aged 49 or younger, normal values are at or below 25 mm/h.
▪ In women aged 50 or older, normal values are at or below 30 mm/h.
o Comprehensive Metabolic Panel (CMP)
▪ A CMP gives information about the status of the client's kidneys, liver, electrolyte and acid/base balance, blood sugar and blood proteins. Clients should be NPO 10-12 hours prior to the blood draw.
▪ Standard CMP includes a group of 14 tests: albumin, alkaline phosphatase, alanine transaminase (ALT), aspartate aminotransferase (AST), BUN, (serum) calcium, (serum) chloride, CO2, creatinine, direct bilirubin, gamma-glutamyl transpeptidase (gamma-GT), glucose test, lactate dehydrogenase (LDH), (serum) phosphorus, potassium, (serum) sodium, total bilirubin, total cholesterol and uric acid.
• Venous tests
o Phlebography
▪ Thrombi can be identified as radiolucent areas in opaque-filled veins.
o Venous Pressure Measurements
▪ This test is used in early stages of thrombophlebitis. Venous occlusion in one leg causes venous pressure to be higher in the other leg.
o Isotope Studies
▪ This is used to diagnosis early formation of thrombi. Radioactive iodine molecules counts are increased over thrombi.
o Doppler Studies
▪ This indicates obstruction in blood flow. An electronic stethoscope detects the sound of the blood flow.
Perioperative Care
Perioperative care is the care that is given before, during and after surgery. This period is used to prepare the client both physically and psychologically for the surgical procedure and what to expect after surgery. Information obtained during preoperative assessment is used as a basis for the care plan for the client.
Preoperative care begins with the decision to perform surgery and ends when the client enters the operating room.
Fears of Surgery at Different Developmental Stages
• Newborn
o Be sure to include parents as much as possible as you prepare the newborn for a procedure. Be aware that newborns startle easily from loud noises and sudden movements. A mummy restraint is most effective and creates security for the newborn as well.
• Toddler
o Toddlers have separation fears. The nurse will teach the parents to expect
regression. Simple explanations and distractions are effective when preparing a toddler for a procedure.
• Preschooler
o Preschoolers fear both mutilation and separation. The nurse will allow the client
to play with models of equipment and encourage clients to express how they feel. They respond well to puppets and dolls when explaining a procedure. Be sure to talk at the client's eye level.
• School-age
o School-age clients fear of losing control, death and being alone. Explain all
procedures in simple terms and allow choices when possible.
• Adolescent
o Adolescent clients fear losing their independence and being different from their
peers (including alterations in body image). The nurse will involve the adolescent by discussing procedures and therapies ahead of time, and by providing privacy whenever possible. Expect resistance from adolescent clients. Empathy and understanding their concerns is key in building trust.
Preparation for Surgery
• Preoperative Checklist (Organization-specific)
o The nurse will verify that the informed consent form is signed prior to the
surgical/procedure preparation. The client will remove dentures, jewelry and nail polish. The client will be NPO 12 hours prior to surgery and all supplements will be discontinued. Many organizations require a 2-3 -week discontinuation of certain medications such as anticoagulants.
o Nursing interventions for the preoperative client will include verification that lab tests, chest X-ray and EKG are complete and up to date. Also, ensure that IVs are in place and, if a bowel or skin preparation is necessary, make sure it has been completed. The nurse will provide preoperative medications, sedation and/or antibiotics.
• Preoperative Teaching
o The nurse will address any client concerns and provide information to clear up
any miscommunications or misunderstandings. Discuss what preoperative procedures the client can expect such as needle sticks, medications or skin preparations.
o It is also important to teach the client what to expect postoperatively. Make sure your client understands postoperative recovery needs such as deep breathing, leg
exercises, movement expectations, incentive spirometer and any equipment the client may see or use. Review pain management and the importance of reporting pain.
Pre-anesthetic Medications
• Sedatives/hypnotics — calming effect
• Anticholinergics — to decrease secretions, prevent bradycardia, e.g., atropine
• Tranquilizers/antianxiety agents — to decrease nervousness, promote relaxation, e.g., diazepam (Valium)
• H1-receptor antagonists — to prevent nausea and vomiting, e.g., promethazine (Phenergan)
• Proton pump inhibitors — to decrease acid production in stomach
• Analgesics — for pain relief
• Antibiotic — to decrease risk of infection
Intraoperative Period Perioperative Care
The intraoperative period takes place in the procedure or surgical suite.
• General Anesthesia
o General anesthesia is a drug-induced analgesia that initiates amnesia, muscle
relaxation, and unconsciousness. General anesthesia may be administered just prior to entering the procedure/surgical suite.
• Types of Anesthetic Agents
o Inhalation (gas and liquid): nitrous oxide, cyclopropane halothane, enflurane,
ether, methoxyflurane
o Intravenous agents: methohexital, sodium thiopental
o Dissociative agents: (no loss of consciousness) ketamine
o Neuroleptics: fentanyl citrate with droperidol
• Anesthesia Adjuncts
Description Use/Effect
Regional Regional anesthetic renders a specific body area insensitive to pain The nerve block allows for targeted anesthesia,
while the client remains conscious.
Spinal Anesthetic is injected into subarachnoid space (lower end of spinal cord). Blocks nerve transmission through spinal nerve roots, while the client
remains conscious.
Epidural Local anesthetic is injected into epidural
space. Common in obstetrics and the client remains
conscious.
Peripheral Nerve Block Local anesthetic is
injected around a Provides anesthesia of
area served by that
peripheral nerve. nerve, while the client
remains conscious.
Local A local anesthetic can be topical or infiltrated. Provides anesthesia to local area and is commonly used to suture
wounds.
• Complications
o Potential complications during the intraoperative period include:
▪ History of muscle cramps and/or unexplained death of a relative who experienced a febrile condition during surgery are both indicators of the inherited muscle disorder that is induced by many general anesthetic agents and leads to malignant hyperthermia
▪ Nausea and vomiting
▪ Hypoxia
▪ Hypothermia
▪ Hypothermia
▪ Malignant hyperthermia:
• A rapid rise in body temperature, tachycardia, tachypnea, unstable blood pressure, diaphoresis and muscle rigidity. Can be fatal if not
treated quickly. It is an inherited muscle disorder that is induced by anesthesia.
• Treated with 100% oxygen, skeletal muscle relaxant, and sodium bicarbonate.
• Nursing Considerations
o The nurse will be sure to verify the right site protocol is in use. Providing
emotional support during anesthesia induction and ensuring client safety is critical. The nurse will maintain surgical asepsis.
o The client will be positioned as needed. Monitor for any environmental hazards (i.e. electrical hazards) and assess client heat loss during the surgery. Additionally, the nurse will monitor vital signs, fluid balance and perform a sponge/instrument count. Once the surgical drapes are removed, warm blankets should be applied.
Asepsis - Surgical
• Practices
o Surgical asepsis includes the practices that destroy all microorganisms and their
spores:
▪ Steam under pressure
▪ Gas
▪ Radiation
▪ Chemicals
• Procedures
o Sterile technique involves procedures that keep an object or area free from living organisms:
▪ A sterile object remains sterile only when touched by another sterile object, or, in other words, sterile touching sterile remains sterile
▪ The skin cannot be sterilized and is, therefore, non-sterile
• Uses
o Surgical asepsis is used for many procedures, including:
▪ Care of surgical wounds, i.e., dressing changes
▪ Catheterizations
▪ Tracheostomy care
▪ Suctioning
▪ Surgery
• Principles
o Only sterile objects may be placed on a sterile field
o Always hold your hands above the level of your elbows
o Do not reach over the sterile field
o The edges of a sterile field or container are considered contaminated (depending on the resource, this is approximately 1-2 inches surrounding the border)
• Contamination
o A sterile object becomes contaminated under the following conditions:
▪ Sterile touching clean becomes... contaminated
▪ Sterile touching contaminated becomes... contaminated
▪ Sterile touching questionable is... contaminated
▪ A sterile object or sterile field that is not in the range of vision is... contaminated
▪ An object held below a person's waist is... contaminated
▪ When a sterile object comes in contact with a wet, contaminated surface, it is considered contaminated (through capillary action)
▪ A sterile object becomes contaminated with prolonged exposure to air Postoperative Care (PACU)
Perioperative Care
Postoperative care takes place while the client recovers from anesthesia and the surgical procedure. The time required may range from an hour to several hours.
Assessment
• Neuro-psychosocial
o The nurse will stimulate the client post-anesthesia and monitor the level of
consciousness.
• Cardiovascular
o Monitor vital signs every 15 minutes until stable.
o Monitor I/O and CVP as well as potassium level.
• Respiratory & Pain
o The nurse will turn the client and have the client cough and take deep breaths,
unless contraindicated.
o Teach the client how to use an incentive spirometer and client-controlled analgesia (PCA) if applicable.
o The nurse will assess the client's level of pain and offer analgesia if needed. The client should become mobile as soon as possible if warranted.
• Gastrointestinal
o Check the bowel sounds (high-pitched tympany is abnormal). The client will
remain NPO until bowel sounds are present and normal. If the client remains NPO, provide good oral care.
o Provide antiemetics for nausea and vomiting and check for abdominal distention. Monitor the client for the passage of flatus and/or stool.
• Genitourinary
o Monitor I/O and encourage the client to void. Notify the health care provider if
the client has not voided within eight hours.
• Extremities
o Check extremity pulses and assess color, edema and temperature. Assess for any
pain, swelling and warmth to the distal extremities. Apply anti-embolic stockings or pneumatic compression devices if needed. Have the client keep legs straight; do not use pillows behind the knees.
• Wounds
o Document the amount and character of the drainage and provide dressing changes
per postoperative orders. Use aseptic technique and note surgical drains if present.
o If applicable, assess the wound site, note any drainage and document the type of sutures. Evaluate wound edges and provide debridement if ordered. Anticipate infection and change dressing as ordered to prevent bacterial growth.
Complications
• Hemorrhage
o Monitor for a decrease in the client's blood pressure, an increase in the client's
pulse, and for cold clammy skin. If a hemorrhage occurs, the nurse will replace blood volume and monitor the vital signs as ordered.
• Shock
o Monitor for a decrease in blood pressure, an increase in pulse, or for cold clammy
skin. The nurse will treat the cause of shock, provide oxygen and IV fluids as ordered.
• Atelectasis & Pneumonia
o Monitor the client for dyspnea, cyanosis, cough and tachycardia. The client will
also have a fever and may have pain. This can happen on the second day postoperative. If it occurs, the nurse will provide suctioning, and antibiotics and will have the client cough and turn frequently as ordered.
• Embolism
o Monitor the client for shortness of breath, pain, hemoptysis and restlessness.
ABGs will confirm whether the oxygen level is low and the carbon dioxide is high.
• Venous Thromboembolism
o A venous thromboembolism will be verified by a positive ultrasound. This can
occur from six days to one year after surgery. Anti-coagulation therapy will be necessary.
• Paralytic Ileus
o Monitor the client for absent bowel sounds, flatus or stool. The nurse will provide
nasogastric suctioning, IV fluids and decompression tubes as ordered.
• Wound Infection
o Monitor the client for elevated temperature, inflammation and pain at the wound
site. Positive cultures will verify that an infection is present. Infection can happen 3-5 days postoperative. Antibiotics will be administered as ordered. Aseptic technique and good nutrition are key to recovery.
• Dehiscence
o Dehiscence is a surgical complication in which the wound ruptures along a
surgical incision. This can be experienced 3-5 days postoperative. The health care provider will be notified and the client will be placed on NPO. Place the client in a low Fowler's position and discourage coughing.
• Evisceration
o Evisceration is a protrusion of wound contents. This can be experienced 5-6 days
postoperative. The health care provider will be notified immediately. The client will be placed in a low Fowler's position and coughing will be discouraged. The nurse will cover viscera with sterile saline dressing.
• Urinary Retention
o If the client is unable to void after surgery due to bladder distention, the client will
have to be catheterized.
• Urinary Infection
o The client may experience burning, frequency and urgency with urination or, if
catheterized, foul-smelling urine may be prevalent. Urinalysis will confirm infection and antibiotics will be administered as ordered.
• Psychosis
o A client experiencing psychosis will display an inappropriate affect. Therapeutic
communication and possibly medication will be necessary.
[Show More]




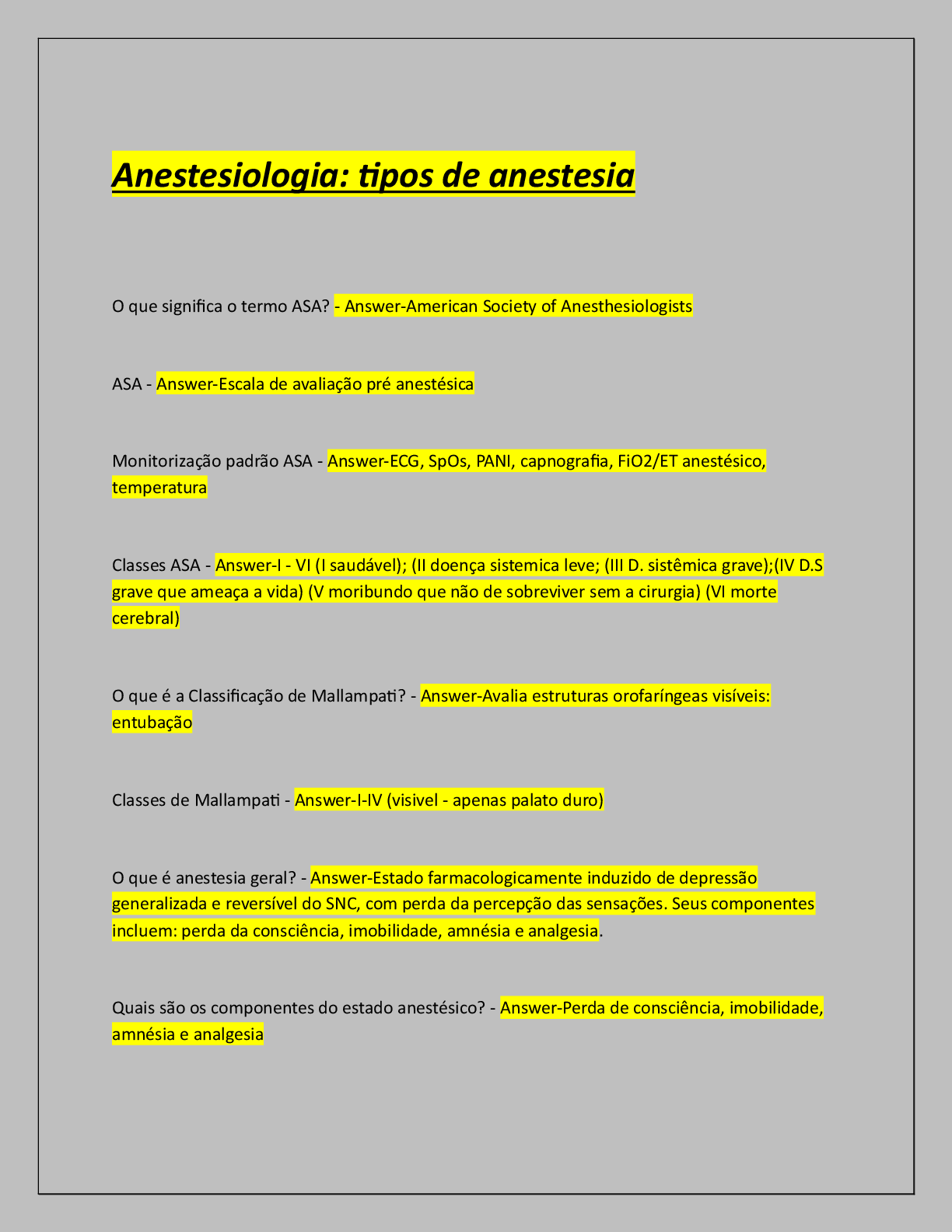

.png)