Social Sciences > QUESTIONS & ANSWERS > ACCS Exam Questions and Answers Rated A+ (All)
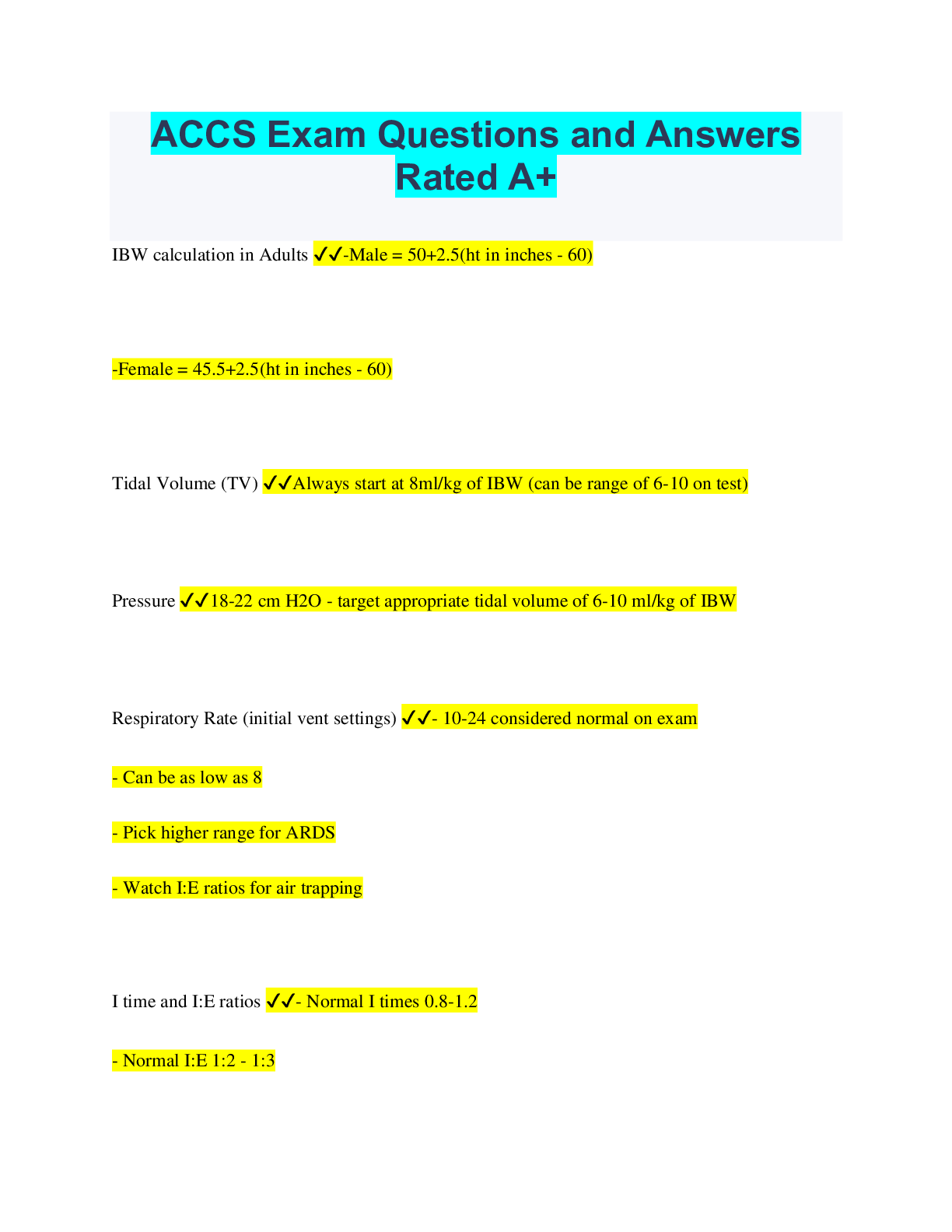
ACCS Exam Questions and Answers Rated A+
Document Content and Description Below
Last updated: 3 years ago
Preview 1 out of 5 pages
Instant download
Buy this Document to get the Full Access Instantly
Provided by Students Who Aced it
We Verify Document Content to Gurantee Accuracy
Reviews( 0 )
Document information
Connected school, study & course
About the document
Uploaded On
Jun 17, 2023
Number of pages
5
Written in
All

Additional information
This document has been written for:
Uploaded
Jun 17, 2023
Downloads
0
Views
111
Document Keyword Tags
Recommended For You
Get more on QUESTIONS & ANSWERS »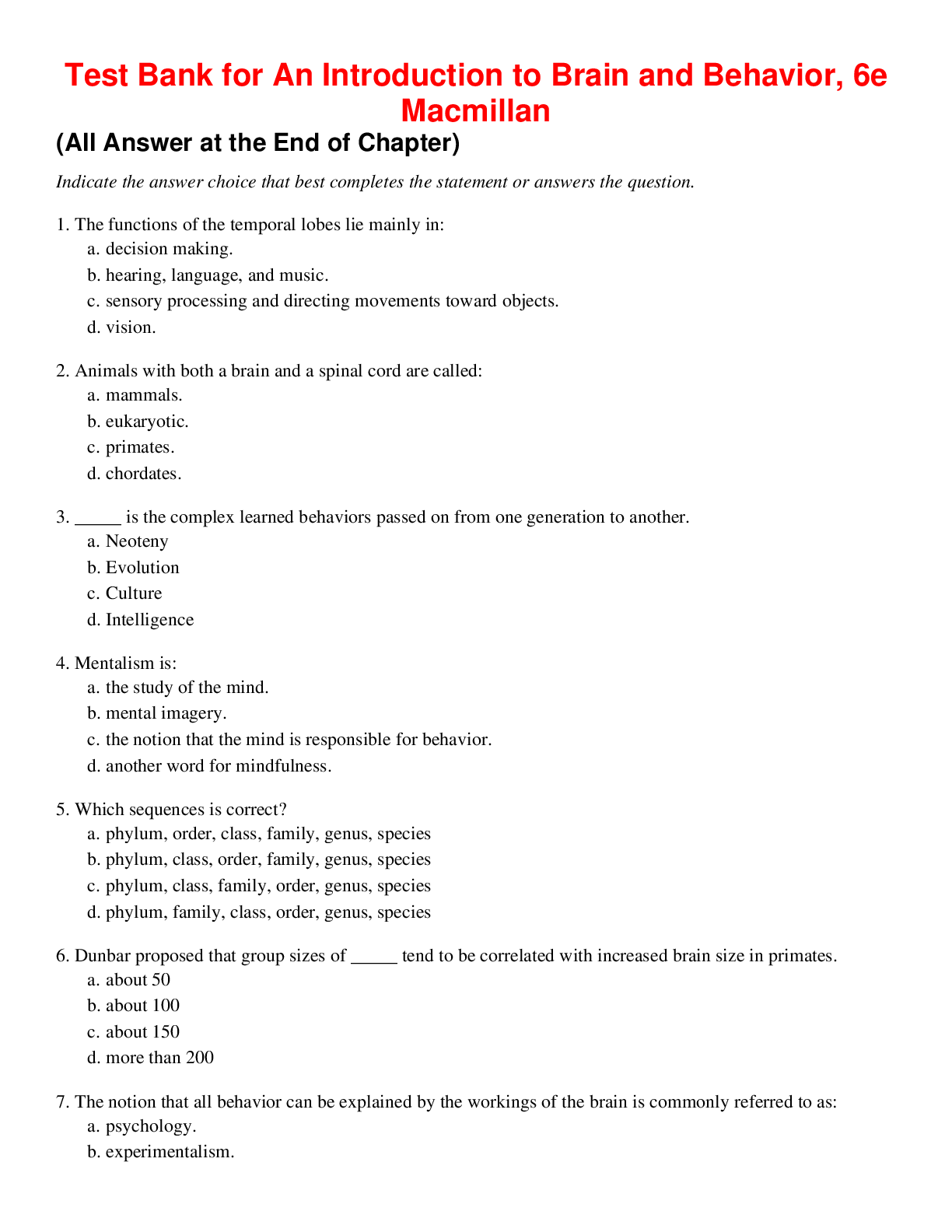
An Introduction to Brain and Behavior, 6e Macmillan (Test Bank...

Archaeology and Humanity's Story A Brief Introduction to World...

Introduction to Family Processes Diverse Families, Common Ties...

Solutions Manual for Mental Health in Social Work A Casebook...


Canadian Families Today 4th Edition by Patrizia Albanese | TES...

Intimate Relationships, 3e Thomas Bradbury, Benjamin Karney (T...


Approaches to Social Research 6e Singleton Straits (Test Bank)
Aging as a Social Process Canada and Beyond 7th Edition By And...

Advanced Public Speaking A Leader's Guide, 2e Michael Hostetl...

Bioethics Principles, Issues, and Case, 4th Edition By Lewis V...

Worlds Together, Worlds Apart, 5e Jeremy Adelman, Stephen Aron...

An Introduction to the Policy Process Theories, Concepts, and...

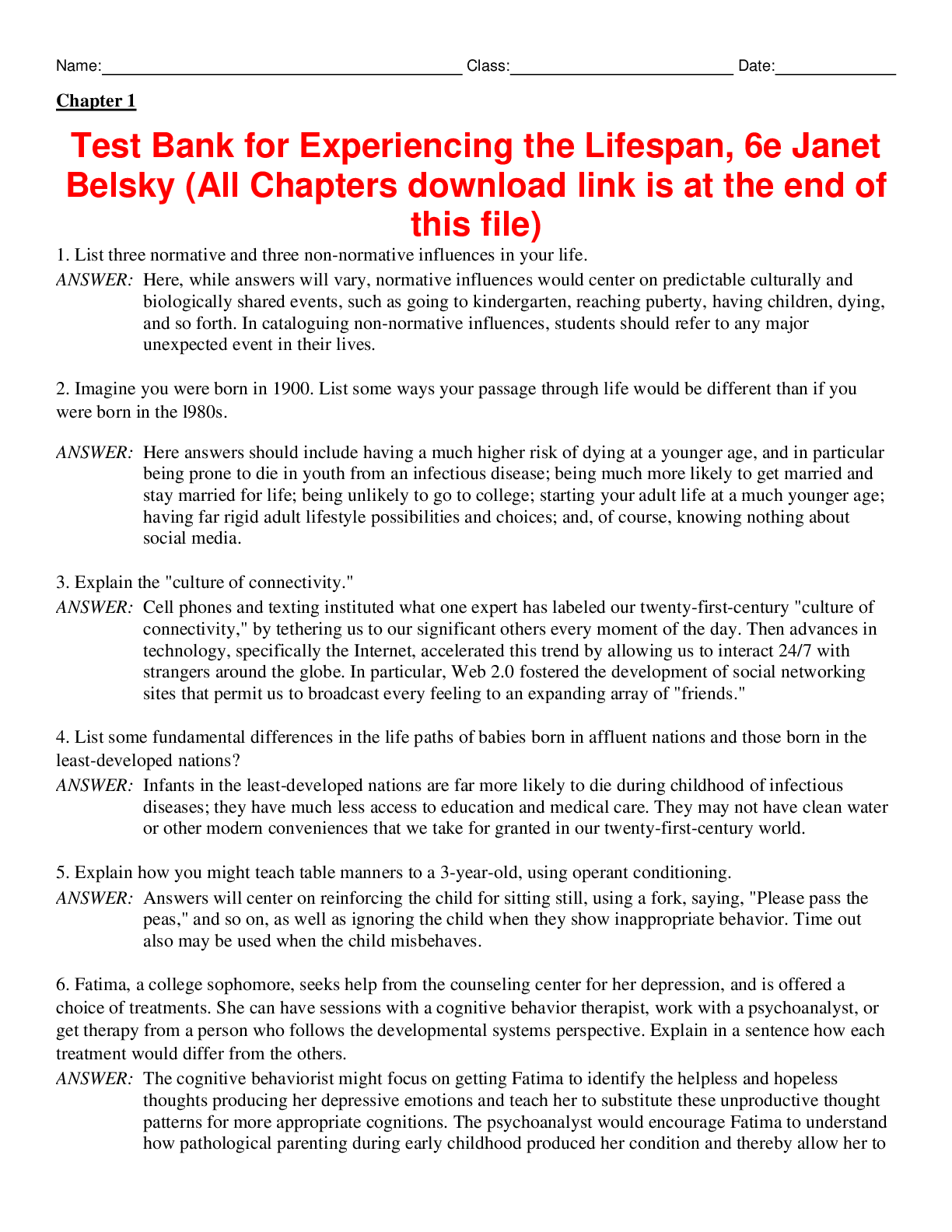
Test Bank for A Topical Approach to the Developing Person Thro...
Persuasion in Society, 4e by Jean Jones, Andi McClanahan, Jose...
An Introduction to Native North America 6th Edition By Mark Su...