Surgery NBME Form 1 - Questions and Answers 42 yo - hospital w/ piece of meat lodged in lower esophagus meat removed by esophagoscopy w/ difficulty evening - 101 F most app dx study? water-soluble contrast upper gastro
...
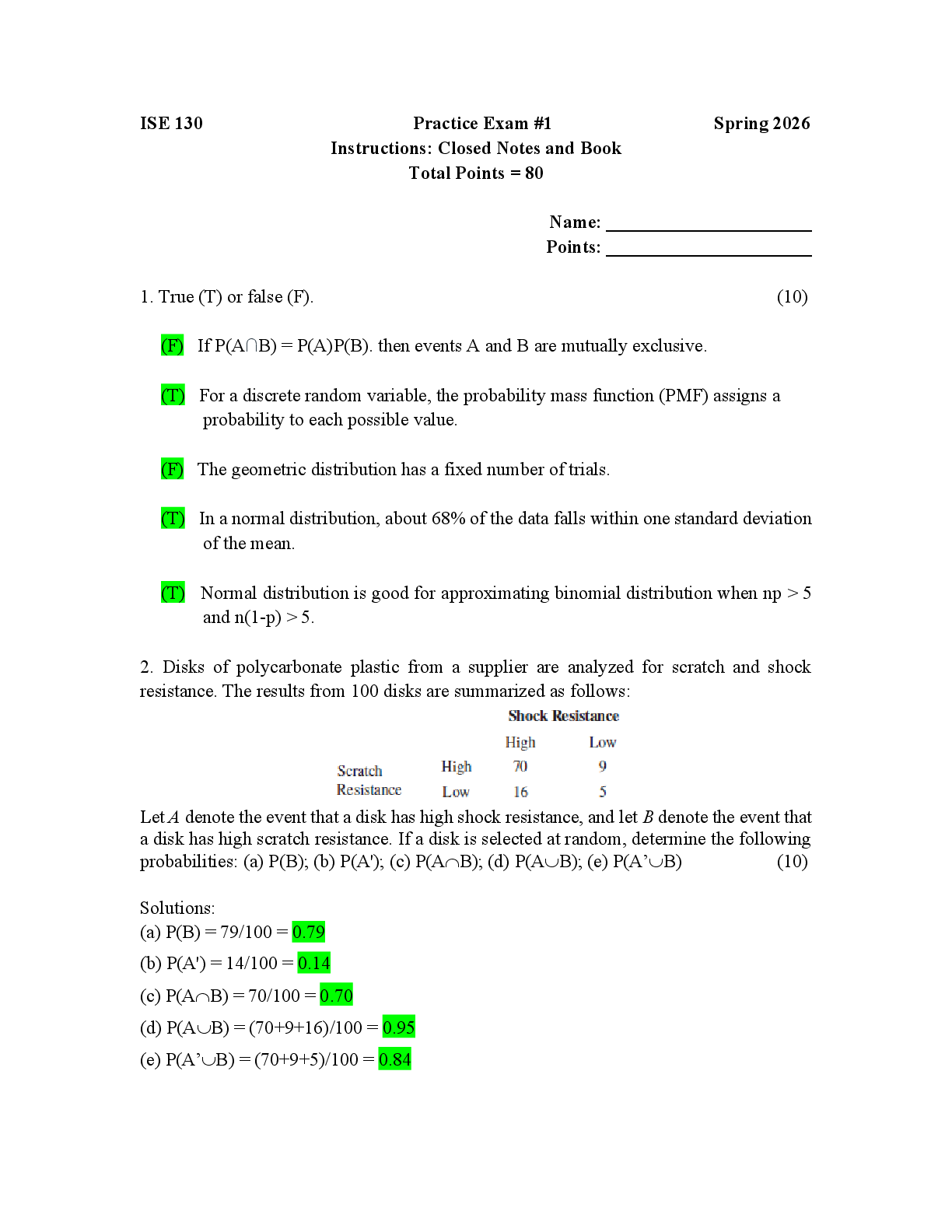
Surgery NBME Form 1 - Questions and Answers 42 yo - hospital w/ piece of meat lodged in lower esophagus meat removed by esophagoscopy w/ difficulty evening - 101 F most app dx study? water-soluble contrast upper gastrointestinal study don't repeat what procedure damaged her esophagus water-soluble aka gastrograffin - dx esophageal rupture neck x-ray - if food/thing stuck in oropharynx upper GI study - if want to look at thorax if this procedure is non-dx > Ba study if perforation confirmed > primary closure of esophagus and drainage of mediastinum PE: Hamman sign - crunching sound on chest ausc 52 yo - ED due to 4 days of progressive back pain and weakness/numbness in legs hasn't urinated in 12 days PMHx: L.mastectomy (for breast cancer) 5 yrs ago PE: CNs intact; muscle strength 3-4/5 in lower ext; DTRs 3+ in knees/ankles; Babinski sign BL; sens to pinprick dec below nipples; sens to vibration absent in lower ext unable to walk MSE: gucci insertion of catheter - 400 mL of urine most likely location of abnormality? thoracic spinal cord breast cancer loves to met to the bone mass compressing on spinal cord dec pinprick sens below T4 = thoracic location *LMN signs at level of lesion UMN signs below level of lesion* early signs: symmetric lower-ext weakness, hypoactive/abs DTRs late signs: BL Babinski reflex, dec rectal sphincter tone, paraparesis/paraplegia w/ inc DTRs, sens loss mgnt: emergency MRI; IV glucocorticoids; rad-onc and neurosurg consultations 37 yo - bruising on arms/abd for 3 wks meds: Ibuprofen (occ HAs) PE: ecchymoses over upper ext/trunk; lungs clear; cardiac/abd - gucci CBC: Hgb, WBC - WNL; dec plt (45,000); inc PT (15), bleeding time (11) bone marrow aspirate: inc megakaryocytes most likely explanation?
formation of antiplatelet antibodies homegirl has ITP AI dz - dx of exclusion IgG Abs coat/damage plts > removed by splenic macrophages most acute cases preceded by viral infection chronic: mostly women 20-40 yo symptoms: petechiae and ecchymoses on skin; bleeding of mucous membranes bone marrow aspiration: inc megakaryocytes peripheral smear: dec plts inc plt-ass IgG tx: steroids; IVIg started acutely to get plts up faster; splenectomy if steroids fail; romiplostim and eltrombopag - for splenectomy-res pts 67 yo - operative formation of AV conduit in L.forearm for vasc access performed under axillary block anesthesia PMHx: end-stage renal dz, atherosclerotic CAD, T2DM 24 hrs later - SOB P: 129/min RR: 38/min, shallow BP: 100/55 mmHg PE: JVD; crackles BL bases; S1/S2 normal; S3 and S4 present; no edema of sacrum/ext begin 300 mL of fluids most likely dx? high-output congestive heart failure AV fistulas - blood takes path of least resistance into venous system lots of arterial blood going into venous system > inc preload > inc CO > CHF crackles in lungs, JVD, S3/S4 - due to fluid buildup in CHF 46 yo - ED due to 12 hrs of N/V and mid abd that radiates to the back PMHx: chronic alcoholism P: 120/min RR: 20/min BP: 110/60 mmHg abd exam: tenderness to palp over upper quadrants; bowel sounds absent CBC: dec Hgb (10.1); inc WBC; WNL plt CMP: inc amylase (1842), glucose (248); dec Ca; WNL albumin next step is IV administration of ? lactated Ringer solution supportive care for acute pancreatitis MC causes: alcohol abuse and gallstones recurrences common in alcoholic pancreatitis symptoms: abd pain (epigastric > back); N/V; anorexia dec/absent bowel sounds = partial ileus labs: lipase > amylase tx: bowel rest (NPO); IVF; pain control (fentanyl and meperidine) 27 yo - ED 4 hrs after onset of bloody diarrhea > int nonbloody diarrhea - 6 months > 4 days of and cramps > last week: dec appetite > 15 lb weight loss PMHx: HIV+; 2 hospitalizations for PCP during last yr meds: didanosine, indinavir, stavudine, TMP-SMX 103 F P: 130/min RR: 24/min BP: 80/60 mmHg PE: diffuse crackles BL; rigid, tympanic, distended abd w/ diffuse rebound tenderness; dec bowel sounds; DRE - gross blood CBC: dec Hgb (8), Hct (24%), WBC (3500) fluid resuscitation w/ 0.9% saline and transfusion of 2 units of pRBCs > total and colectomy w/ ileostomy for perforated cecum path: diffuse mucosal inf w/ nuclear inclusion bodies most likely causal org? Cytomegalovirus symptoms: freq, small volume diarrhea; hematochezia; abd pain; low-grade fever; weight loss nuclear inclusion bodies = virus PNA symptoms + diarrhea > if immunosup - CMV > if immunocomp - legionella MC causes of diarrhea in pts w/ AIDS: crypto-/micro-/iso-sporidium; MAC; CMV 47 yo - 2 wks of fatigue and prog abd swelling abd exam: shifting dullness and distention; bowel sounds normal; no tenderness/ masses/ organomegaly dx paracentesis - 50 mL of milky chylous fluid most likely cause? lymphoma chylous acites > look for malignancy obstructing lymphatic flow MC cause of chylous ascites: > in the U.S.= lymphoma > in the developing world = TB intra-abd malignancy can invade or externally compress retroperitoneal lymph vessels > obstruction of lymph flow into the thoracic duct > lymphedema = leakage of lymph into the peritoneal cavity
[Show More]