WGU Secure Software Design (D487, KEO1) Exam questions and answers 2026 latest update
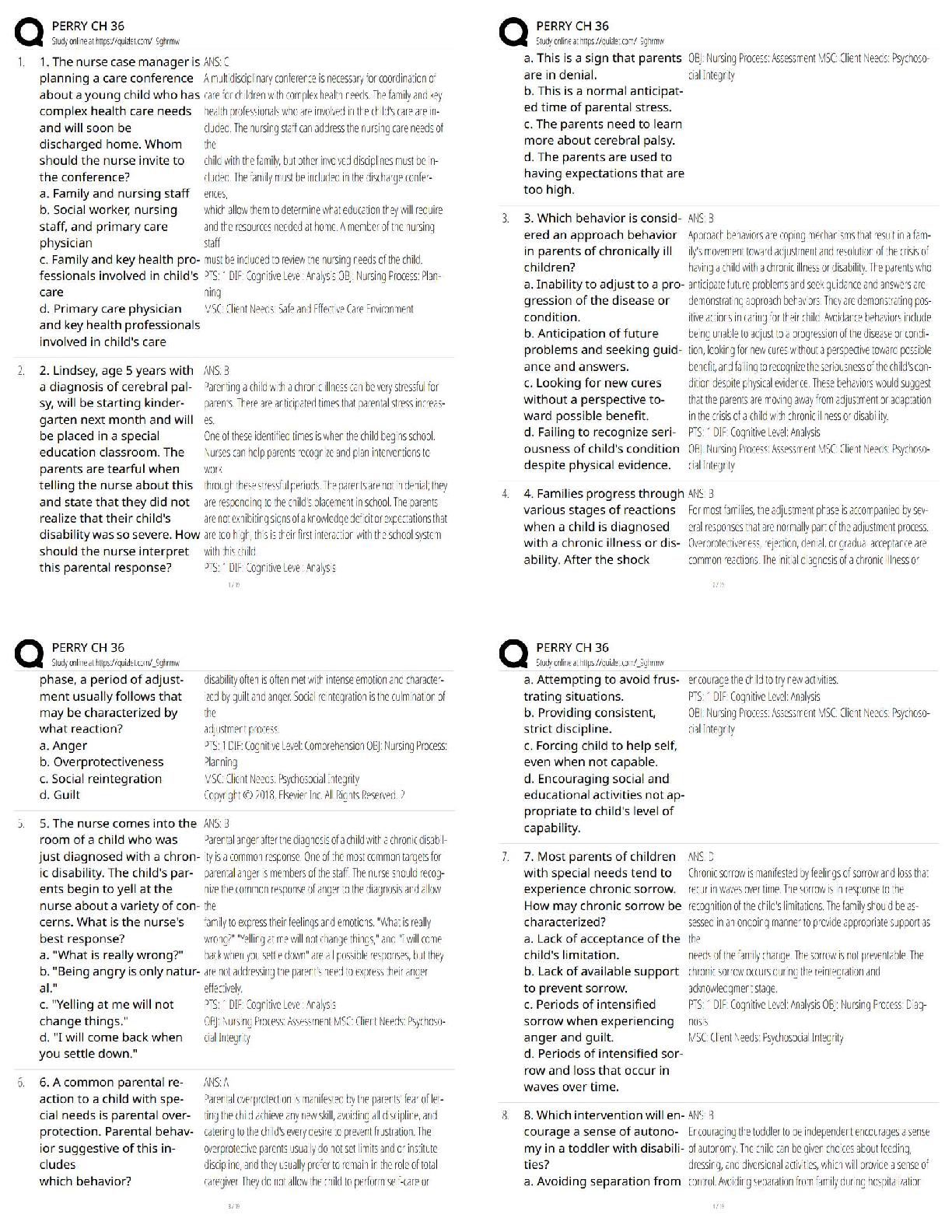
NURSING > STUDY GUIDE > Chapter 36 Pulmonary alterations in children (All)
Last updated: 3 years ago
Preview 1 out of 73 pages
Instant download

Buy this Document to get the Full Access Instantly
Provided by Students Who Aced it
We Verify Document Content to Gurantee Accuracy
Connected school, study & course
About the document
Uploaded On
Jul 17, 2021
Number of pages
73
Written in
All
This document has been written for:
Uploaded
Jul 17, 2021
Downloads
0
Views
119




.png)
 (1).png)

.png)
 Med Surg test Latest Verified Questions and all Correct Answers with Explanations Chapter 36 Management of Patients with Immune Deficiency.png)
 Med Surg test Latest Verified Questions and all Correct Answers with Explanations Chapter 36 Management of Patients with Immune Deficiency Disorders.png)


Scholarfriends.com Online Platform by Browsegrades Inc. 651N South Broad St, Middletown DE. United States.
We're available through e-mail, Twitter, and live chat.
FAQ
Questions? Leave a message!
Copyright © Scholarfriends · High quality services·






.png)
.png)



