*NURSING > EXAM > NSG 300 Maternal Newborn 1 ATI – Our lady of Holy Cross College / NSG 300 Maternal Newborn 1 ATI (All)
NSG 300 Maternal Newborn 1 ATI – Our lady of Holy Cross College / NSG 300 Maternal Newborn 1 ATI
Document Content and Description Below
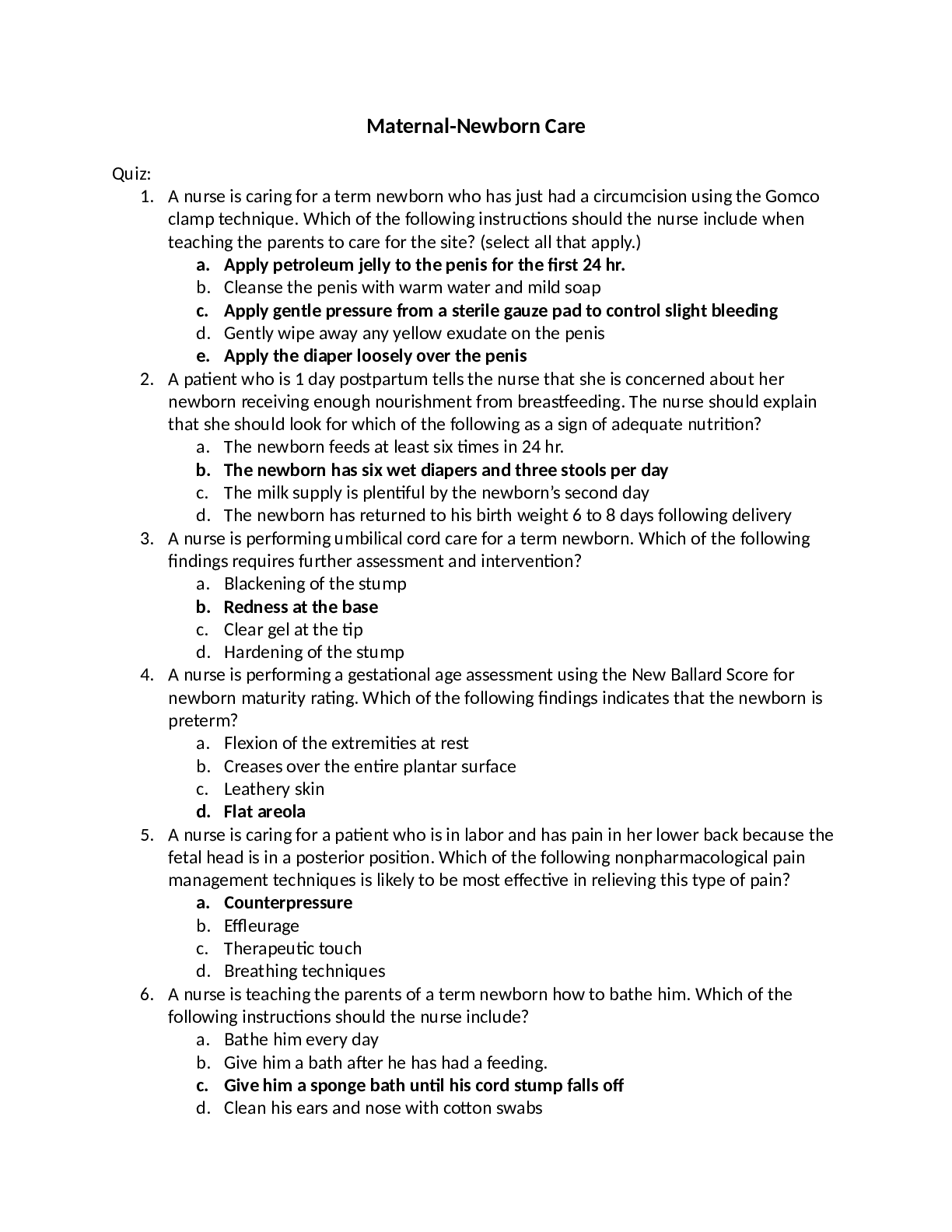
NSG 300 Maternal Newborn 1 ATI – Our lady of Holy Cross College. Maternal-Newborn Care Quiz: 1. A nurse is caring for a term newborn who has just had a circumcision using the Gomco clamp tec... hnique. Which of the following instructions should the nurse include when teaching the parents to care for the site? (select all that apply.) a. Apply petroleum jelly to the penis for the first 24 hr. b. Cleanse the penis with warm water and mild soap c. Apply gentle pressure from a sterile gauze pad to control slight bleeding d. Gently wipe away any yellow exudate on the penis e. Apply the diaper loosely over the penis 2. A patient who is 1 day postpartum tells the nurse that she is concerned about her newborn receiving enough nourishment from breastfeeding. The nurse should explain that she should look for which of the following as a sign of adequate nutrition? a. The newborn feeds at least six times in 24 hr. b. The newborn has six wet diapers and three stools per day c. The milk supply is plentiful by the newborn’s second day d. The newborn has returned to his birth weight 6 to 8 days following delivery 3. A nurse is performing umbilical cord care for a term newborn. Which of the following findings requires further assessment and intervention? a. Blackening of the stump b. Redness at the base c. Clear gel at the tip d. Hardening of the stump 4. A nurse is performing a gestational age assessment using the New Ballard Score for newborn maturity rating. Which of the following findings indicates that the newborn is preterm? a. Flexion of the extremities at rest b. Creases over the entire plantar surface c. Leathery skin d. Flat areola 5. A nurse is caring for a patient who is in labor and has pain in her lower back because the fetal head is in a posterior position. Which of the following nonpharmacological pain management techniques is likely to be most effective in relieving this type of pain? a. Counterpressure b. Effleurage c. Therapeutic touch d. Breathing techniques 6. A nurse is teaching the parents of a term newborn how to bathe him. Which of the following instructions should the nurse include? a. Bathe him every day b. Give him a bath after he has had a feeding. c. Give him a sponge bath until his cord stump falls off d. Clean his ears and nose with cotton swabs 7. A newborn delivered vaginally at term 1 min ago cried loudly at delivery, has a heart rate of 140/min, has well flexed arms and legs, grimaces when the nurse rubs the soles of his feet, and is pink with mild acrocyanosis. What apgar score should the nurse assign to this newborn? a. 8 8. A nurse is assessing a patient at a routine antepartum visit. For a rough estimate of the number of gestational weeks the patient is at, the nurse should measure the number of cm between which two anatomical landmarks? a. The mons pubis and the xiphoid process b. The top of the fundus and the umbilicus c. The symphysis pubis and the top of the fundus d. The mons pubis and the umbilicus 9. A nurse is assessing a patient who is 1 day postpartum and is not breastfeeding. The nurse notes the patient’s breasts are engorged. Which of the following actions is appropriate for the patient to take? a. Applying ice packs b. Wearing a loose-fitting bra c. Pumping her breasts d. Taking a warm shower 10. A nurse is assessing a patient who is at 20 weeks of gestation. She instructs the patient to be sure to report headaches, blurred vision, and swelling of her hands because these are indications of which of the following complications of pregnancy? a. Gestational diabetes b. Preeclampsia c. Hyperemesis gravidarum d. Abruptio placentae Auscultating Fetal Heart Tones • Possible to hear fetal heart tones around the 10th or 11th week of gestation with an ultrasound fetoscope or stethoscope. o Regular fetoscope and stethoscope can transmit fetal heart tones at 18 to 20 weeks • To auscultate fetal heart tones: o Apply conductive gel to the patient’s skin o Position the device midline just above the symphysis pubis o Apply firm pressure o Move the device around slowly until you hear heart tones o Count the fetal rate for 1 minute ♣ Assess the quality and rhythm • The fetal heart typically beats 120 to 160 times a minute Gestational Age Assessment • To determine the approximate age, you will assess six neuromuscular and six physical characteristics • The New Ballard Score o Appropriate for newborns from 20 to 44 weeks of gestation o Each parameter scores from a minus 2 to 5 with the cumulative score correlating with a gestational age between 26 and 44 weeks • For newborns younter than 26 gestational weeks, perform the assessment sooner than 12 hours after birth. • For newborns beyond 26 gestational weeks, perform the examination within 96 hours of birth. (best to perform the examination within 48 hours of birth) • The gestational assessment is important because it relates directly to the likelihood of complications during the newborn period o Lower scores correlate with prematurity o Higher scores correlate with postmaturity. • Neuromuscular assessment components o Posture ♣ Assess posture for the degree of flexion of the extremitites ♣ At term, they are moderately flexed at rest ♣ Preterm show lesser degrees of flexion o Square window ♣ Assess square window by grasping the newborn’s forearm and gently flexing the wrist toward the inner arm. ♣ Do not allow rotation of the wrist ♣ Measure the angle that forms where the hand meets the wrist • At term, the hand should touch the wrist ♣ Preterm newborns show greater angles of flexion • Very preterm newborns have an angle of wrist flexion of 90 degrees or more o Arm recoil ♣ Measure arm recoil by first flexing and holding both forearms for 5 seconds, then extending the arms and hands fully at the newborn’s side. ♣ Release the hands and allow the arms to recoil (return to flexion) ♣ Term newborns demonstrate full recoil to a position of flexion while preterm newborns show less flexion ♣ Measure the arm at the elbow to determine the arm recoil score o Popliteal angle ♣ Press the newborns thigh against his abdomen, measure the popliteal angle by moving the foot gently toward the head until you meet resistance. ♣ Measure the angle behind the knee in the popliteal area ♣ Term newborns are less flexible with about a 90-degree angle. ♣ Very preterm newborns, the leg straightens to a 180-degree angle o Scarf sign ♣ Assess the scarf sign by grasping the newborn’s hand and attempting to cross the arm over his body at the neck. ♣ The arms of term newborns meet resistance before crossing midline, while preterm newborns cross the elbow past midline o Heal to ear ♣ Assess heel to ear by raising the newborn’s heel toward his head in an attempt to bring the foot to the ear. ♣ Do not raise the newborns buttocks off the examination surface. ♣ Stop when you meet resistance and measure the degree of extension of the leg ♣ With preterm newborns, you’ll come close to touching the heel to ear, while you’ll meet resistance almost immediately with term newborns o Perform all of these assessments with the newborn lying supine o Refer to the scoring sheet for specific scores based on your findings • Physical Maturity o Components of physical maturity: ♣ Skin • Ranges from translucent and friable in preterm newborns • Leathery, cracked, and wrinkled in post-term newborns ♣ Lanugo • Very fine body hair • Extremely premature newborns have none • During the third trimester, most fetuses have plentiful lanugo • Term newborns have very little, and it is nearly absent in post-term newborns ♣ Plantar surface • Inspect for creases • Term newborns have creases over the entire plantar surface • Preterm newborn range from absent to faint red markings ♣ Breast • Inspect the breast to assess the size of the breast bud in millimeters and the development of the areola. • Preterm newborns lack developed breast tissue • Term newborns have a raised to full areola with breast buds that are 3 to 10 millimeters in diameter ♣ Eye/ear • Analysis of the ear cartilage and shape of the pinna • Pinna is less curved in preterm newborns • Term newborns have a well-curved pinna with firm cartilage • Ear recoil o Fold the pinna down and assess how quickly it returns to its previous position. • Very preterm newborns may have fused eyelids ♣ Genitals • Observe the genitals for physical maturity • Males o Testes usually descent near term and rugae (ridges or folds) are visible on the scrotum o Palpate the testes to determine if they have descended and note the rugae o With extreme prematurity, the scrotum is flat and smooth. • Females o At term, the labia majora are larger than the clitoris and the labia minora o Preterm newborns have a prominent clitoris and small labia minora Leopold Maneuvers • Comprise a stepwise method of abdominal palpation you can use to determine the number of fetuses, the presenting part, the fetal lie, the fetal attitude, the fetal position, the degree of the descent into the pelvis, and the best location for auscultating fetal heart tones. • Four Leopold maneuvers: o Identifying the fetal part in the uterine fundus to determine fetal lie and the presenting part ♣ Place both hands on her abdomen, cupping your hands around the fundus or the top of the uterus. ♣ Palpate for the fetal part that occupies the fundus to help identify fetal lie and presentation ♣ Feel for shape, consistency, and mobility ♣ The fetal head will feel firm and round ♣ The breech with feel softer and less defined o Palpating the fetal back to identify fetal presentation ♣ Position palms of your hands on the side of the patient’s abdomen. ♣ Use the palmar surface of one hand to locate the fetal back and the various irregularities to identify hands, feet, and elbows ♣ The fetal back will feel smooth and hard ♣ The smaller fetal parts, such as the hands, feet, and elbows will feel like irregular nodules when you palpate them ♣ This also helps determine the fetal presentation o Determining which fetal part lies over the pelvic inlet to identify fetal attitude ♣ Use your left hand to grasp the lower section of the patient’s abdomen between your index finger and thumb and press inward over the inlet to the true pelvis. ♣ Note any movement and determine whether the presenting part is soft or firm • No movement means the presenting part is not engaged ♣ If the head is the presenting part, determine fetal attitude • Whether the head is flexed or extended o Locating the fetal cephalic prominence to identify the attitude of the head ♣ Face the patient’s feet and place both hands on both sides of her uterus. ♣ Outline the fetal head with your fingertips. ♣ Palpate both sides of her abdomen to determine the cephalic prominence, or brow. ♣ Note that this maneuver applies only to cephalic presentations ♣ If you find the cephalic prominence on the same side as the feet, hands, and elbows, the head is flexed and vertex is presenting. ♣ If you find the cephalic prominence on the same side as the back, then the head is extended and the face is presenting • Procedure o Begin by asking the patient to empty her bladder so she won’t feel any discomfort o Position a small rolled towel under one hip to shift her uterus away from large blood vessels and thus prevent supine hypotensive syndrome. o Stand on patient’s left side (right side if right handed) facing her. o Use the flat palmar surface of your fingers to perform Leopold maneuvers • After Procedure o Assess the patient’s response and then assess the fetal well-being. ♣ Do this by checking the fetal heart tones and by noticing any changes in fetal position. Measuring Fundal Height • During the second trimester, the uterus becomes part of the abdomen, a development that makes it easy to assess fundal height. • From weeks 18 to 32, the number of centimeters of fundal height is just about equivalent to the weeks of gestation • Make sure the patient has emptied her bladder because it can change the measurement by 3 cm • Procedure: o Have her lie supine with her head slightly elevated on a pillow, or her knees in a flexed position, or both. o Make sure the position is the same for each measurement o Using a disposable metric tape measure, note the distance from the symphysis pubis to the top of the fundus. o The result in centimeters is a rough estimate of gestational age • Fundal heights below the estimated gestational age might suggest a miscalculation in due dates, intrauterine growth restriction, or a fetal anomaly. • Measurements above the patient’s gestational age might indicate hydramnios, a large for gestational age fetus, a miscalculation in due dates, or a multiple pregnancy Newborn Care • When a patient and her newborn are ready to leave the facility varies with their physiologic status, type of delivery, feeding success, safety, and various other factors. • Federal legislation ensures that all health plans allow for a minimum of 48 hours of hospitalization after vaginal birth and 96 hours after cesarean birth. • Parents must learn the skills of feeding, clothing, bathing, and protecting their infant before they leave. • Umbilical Cord Care o Teach parents to keep the umbilical cord clean and dry. o Remove the cord clamp when the cord is dry, usually about 24 hours of age o Assure them that they can clean the stump with water as long as they allow it to dry afterward. o Parents should watch for swelling, redness at the base of the stump, purulent drainage, and foul odor from the stump at each diaper change. o Show them how to fold the upper edge of the front of the diaper down below the umbilicus so the stump remains exposed and dry. o The stump will probably fall off between 10 to 14 days after birth • Circumcision Care o Apply petroleum jelly for the first 24 hours to keep the diaper from adhering to the circumcision site o Plastibell method: ♣ Petroleum jelly is unnecessary o Administer acetaminophen (Tylenol) as needed for pain. o Observe the penis for adequate urination. o Cleanse the penis with warm water o Apply the diaper loosely o Caution the parents about the yellow exudate they may see on the glans after 24 hours and for the next 2 to 3 days. (do not remove it) o They may control minor bleeding with gental pressure from a sterile gauze. • Bathing o Opportunity for interaction and bonding o Have parents start with a simple sponge bath ♣ Should practice this method until the umbilical cord stump falls off o Daily bathing is unnecessary o A good time for a bath is when the newborn awakes and before a feeding o To prevent heat loss: ♣ Perform the bath quickly in a warm room, exposing only a portion of the body at one time. o Use soft clean washcloths o Begin by washing the face with plain water. o Cleanse the eyes from in to out o Use mild, unscented, pH-neutral soap o Wash the creases in the neck and under the arms and legs and in the groin as well as the rest of the body with soap and water o Clean the diaper area with each change. o For girls, gently separate the labia and carefully wash from the pubic area toward the anus. o For uncircumcised boys, gently retract the foreskin until you feel resistance. o Wash the tip with warm soap and water and replace the foreskin. o Do not use creams, lotions, powders, or ointments routinely. • Diaper Rash o Clean the area after each urination and bowel movement o Bacteria that cause diaper dermatitis thrive in moist dark areas. To treat diaper rash, clean the area after each urination and bowel movement. Exposing the buttocks to air helps prevent bacterial growth. For infants prone to diaper rash or to help heal a rash, apply zinc oxide ointment to protect the skin. A fungal rash from Candida albicans requires treatment with an antifungal ointment and possibly oral medication. Signs of this type of diaper rash include severe erythema in the perianal area, inguinal folds, and lower abdomen. • Nail Care o It is not necessary to trim a newborn’s nails until they have grown long enough to extend beyond the skin of the tip of the fingers and toes. Then, parents should use manicure scissors or clippers to trim them straight across or use an emery board to file them and keep them short. The best time to trim the nails is while the infant is sleeping. • Clothing o Parents should dress the infant for comfort and security. A cap can help minimize heat loss and protect the infant from the sun. Swaddling in a blanket provides a secure feeling and helps maintain body temperature. Avoid overdressing the newborn. A general guideline is to dress the newborn as warmly as the parents would dress themselves. Make sure all clothing is flame-retardant. • Safety o Parents may not be aware of many potential dangers for their newborn. Provide instructions such as these to promote safety. ♣ Do not leave an infant alone on a bed, table, or other furniture. ♣ Place infant carriers on the floor, never on high places such as counters and beds. ♣ Set the water heater to 49° C (120° F) or less. Test bath water temperature with a bath thermometer. ♣ Pick an infant up gently and never swing, throw, or shake him. ♣ To prevent respiratory illnesses, never expose an infant to tobacco smoke. ♣ Make sure crib slats are no more than 6 cm (2.375 inches) apart and the mattress fits snugly against the sides. A mattress is too small if two adult fingers fit between it and the sides of the crib. ♣ Position the crib on interior walls to prevent drafts. ♣ Keep window cords out of reach. ♣ Keep the crib away from heaters to prevent fire. ♣ To prevent suffocation, do not place pillows, stuffed animals, or loose bedding in the crib with an infant. ♣ Use a sleep sack to keep the infant warm instead of loose bedding or comforters. ♣ Do not leave a bib or a pacifier with a string around an infant’s neck during sleep. ♣ Use a firm mattress covered with a sheet. ♣ Position the infant supine to reduce the risk of sudden infant death syndrome. ♣ Do not put an infant to sleep on a waterbed or in the same bed with sleeping adults. ♣ Install smoke detectors and replace their batteries regularly. ♣ Learn infant cardiopulmonary resuscitation. ♣ Never leave an infant in a parked car. • Car Seats o Use only a federally approved, rear-facing car seat and secure it in the rear seat of the vehicle. Make sure the harness is snug and the clip is at axillary level and not across the infant’s neck or abdomen. Follow federal and state regulations for age and weight parameters for car seat types and positions. Many local agencies offer car seat information and actual installation and verification of adherence to safety regulations. • Comforting Techniques o Newborns use nonnutritive sucking to self-soothe. They suck on their own fingers and some use a pacifier. Instruct parents who give their newborn a pacifier to clean it and replace it regularly and not to coat it with sweet solutions. Advise women who breastfeed to delay the use of a pacifier until breastfeeding is well established (generally about 1 month). Caution parents to use only safety-tested commercial pacifiers. o Infants cry to communicate hunger, discomfort, illness, and boredom. They may cry only a few minutes or for 2 hours or more. Encourage parents to interpret what a cry means and respond accordingly. A fussy period each day, usually in the late afternoon or evening, is quite common. During these times comforting measures may not help. It is likely that the infant will fuss until he releases enough energy to fall asleep. o Provide parents with education about techniques to quiet their infant. These include swaddling, soothing noise, skin-to-skin contact, patting, back rubbing, or other mild rhythmic movement such as with a cradle or a rocking chair. Outings in a stroller or a motor-vehicle often help. • Sensory Stimulation o Sensory stimulation promotes development. Encourage parents to hold their infant close while face to face, to provide toys and mobiles with black and white contrasting designs, and to incorporate singing, playing music, massaging, and walking using a stroller into their daily routines. • Signs of Illness o Make sure parents know when to contact their provider, for example, for significantly high or low axillary temperatures, frequent vomiting, poor feeding, diarrhea, decreased urination or bowel movements, cyanosis, breathing difficulties, lethargy, inconsolable crying, eye drainage, or bleeding from the umbilical cord or circumcision. Nonpharmacological Pain Management • Many patients base their perception of the birth experience not so much on the amount of pain they feel but on how well they achieve their goals for managing it. Most expect some pain and will count on you to help minimize it. Nonpharmacologic methods of pain management are ideal for this purpose. They are simple, safe, and easy for you to teach to your patients and their support people. For those who have learned and practiced these strategies prior to labor, you can remind them to use them. • Breathing techniques o Breathing techniques promote relaxation, provide distraction, and improve coping during uterine contractions. They begin and end with a cleansing or focused breath – a slow, relaxing breath in through the nose and gently out through the mouth. Slow-paced breathing is exactly that – the patient inhales slowly through the nose and exhales slowly through the mouth – usually six to nine times per minute and no fewer than three to four. With modified-paced breathing, the patient breathes slowly in and out through her mouth, and, as each contraction reaches its peak, she breathes faster – usually 32 to 40 breaths per minute. As the contraction subsides, the patient returns to slow breathing. Pattern-paced breathing requires more concentration as the patient sets up a pattern of breathing to help her through the final centimeters of cervical dilation. Breathing in and out of her mouth, she takes quick panting breaths and then exhales or blows forcefully. One method is to make a “hee” or “hoo” sound in a pattern. The pattern may vary, but typically after the cleansing breath, the patient breathes in a 3-to-1 pattern – “pant-pant-pant-blow” or “hee-hee-hee-hoo” throughout the entire contraction and ends with a cleansing or focused breath. The rate is usually the same as with modified-paced breathing. The nurse and the support person can coach her by breathing with her, counting the breaths, reminding her to use the cleansing breaths, and making sure she takes even breaths to avoid hyperventilation. • Touch o Massage is an effective technique for enhancing relaxation and comfort. Massaging the patient’s head, hands, feet, and back provides comfort and communicates caring. Counterpressure is steady pressure a support person applies to the sacral area of the patient’s back. This is especially helpful for patients who have pain and internal pressure in the lower back because the fetal head is in a posterior position. The coach or the nurse uses the heel of the hand or a fist to achieve adequate counterpressure. Effleurage is light massage or stroking, usually on the patient’s abdomen in rhythm with breathing during contractions. The support person uses the fingertips with enough pressure to avoid tickling sensations. For patients who have a monitoring belt across the abdomen, the chest and the thigh are appropriate alternatives. Energy work, such as healing or therapeutic touch, involves manipulating energy fields to help reduce anxiety and pain during labor. Certified practitioners perform these techniques. • Positioning o Frequent position changes enhance comfort and relaxation and promote more effective contractions. Upright positions such as walking, sitting, or squatting take advantage of gravity to encourage fetal descent. Combining positions and activities like rocking and slow dancing with relaxation can help reduce pain perception. • Water therapy o Showering, bathing, and sitting in a whirlpool bath can improve comfort, provide a relaxing atmosphere, improve circulation and oxygenation, soften perineal tissues, and make it easier for women in labor to cope with pain. Facility policies vary, but as long as a patient in active labor has no contraindications for these techniques, she can generally stay in the bath for as long as she wishes. Recommendations for jet hydrotherapy are usually for 30 to 60 minutes. Warm water can cause dizziness, however, so it is important to assist patients in and out of the shower or tub. Also be sure to provide a shower stool, so they can sit down easily during showering. o Other therapies vary with the practice setting, the provider, and the patient’s preferences. Some, such as biofeedback, hypnosis, acupressure, acupuncture, and transcutaneous electrical nerve stimulation, require trained practitioners and sometimes specialized equipment. Others such as aromatherapy, imagery, heat and cold applications, and music therapy are easy to implement, require no special certification, and can provide some unique benefits for patients in labor. Nutritional Needs of Newborns • Optimal nutrition during the neonatal period supports newborn growth and development. Feeding also provides an opportunity for parents to bond with their newborn. Current recommendations are for exclusive breastfeeding for the first 6 months of life, followed by a combination of solid foods and human milk until 12 months of age. Parents may also choose to feed their newborn commercially prepared formula. To help parents make an informed decision, offer them evidence-based information about the nutritional needs of newborns, the benefits of breast milk, and the potential risks of formula feeding. • Fluid and calories o For their first 2 days, newborns need 60 to 80 mL of fluid per kilogram (kg) of body weight per day. For the next 4 days, they need 100 to 150 mL/kg/day. For the remainder of their first month, they need 120 to 180 mL/kg/day. They lose fluid through urination and respiration. It is essential to monitor their intake and output carefully, as they have little tolerance for fluctuations in fluid balance. o Caloric intake, measured in kilocalories (kcal), provides energy for growth, physical activity, and metabolic function. For the first 3 months of life, infants require 110 kcal/kg/day. Each ounce of breast milk and of formula contains about 20 kcal. o Increases in a newborn’s appetite generally correlate with growth spurts. Parents usually notice these changes at 10 days, 3 weeks, 6 weeks, 3 months, and 6 months of age. During these times, they should increase the frequency or duration of feedings to accommodate their infant’s nutritional needs. • Breastfeeding o Human milk offers many health benefits for newborns, including enhanced immunity, maturation of the gastrointestinal tract, and reduced risks of diabetes mellitus and childhood obesity. Advantages for the mother include reduced risks of ovarian and breast cancer, promotion of postpartum weight loss, convenience, and minimal cost. o When helping a patient get started with breastfeeding, assess the newborn for feeding-readiness cues, including rooting, sucking motions, and hand-to-hand or hand-to-mouth movements. It is important to initiate breastfeeding when the newborn demonstrates these cues rather than waiting until he is sleeping or crying. The optimal time for initiating breastfeeding is immediately after an uncomplicated birth. Putting the newborn and the mother in direct skin-to-skin contact (kangaroo care) facilitates the first breastfeeding experience for the mother-infant pair. o Common positions for breastfeeding are the cradle, the modified cradle or across-the-lap, the football or clutch hold, and the side lying position. Encourage your patient to use a position she finds comfortable and easily achieves latch, that is, a seal between the newborn’s mouth over the nipple, areola, and breast that creates enough suction to remove breast milk. o Encourage the patient to express colostrum to spread over her nipple. Then, have her support the breast with one hand while bringing the baby’s mouth to it with the other hand. Suggest that she gently stimulate the newborn’s lower lip with her nipple to prompt him to open his mouth. As he does this and his tongue moves down, have her position him on her breast. Be sure his mouth covers the nipple and an area about 2 to 3 cm (1 inch) around the nipple. When the newborn has latched on and is sucking effectively, his chin, cheeks, and tip of the nose all touch the breast; his cheeks are rounded and not dimpled; and you can hear him swallow. His mother should feel a tugging sensation, not pain. The newborn’s jaw should also move smoothly when he sucks. o Breastfeeding patterns vary among newborns, but in general, they should breastfeed eight to 12 times in each 24 hour period. Although newborns are often sleepy during the first few days, parents should attempt feedings every 3 to 4 hours. After this initial period, when their newborn is feeding regularly and gaining weight, it is appropriate for them to shift to on-demand feedings. o The duration of feedings also varies. Also, some newborns feed from one breast per feeding, while others switch easily during a feeding. For those who do not resume sucking when moved to the other breast, make sure your patient alternates breasts from feeding to feeding. Teach parents how to determine when the newborn is finished feeding. The breast(s) will feel softer, the newborn will suck slowly or release the breast, and he will appear content or will fall asleep. These cues help parents determine the appropriate duration of feedings. o For parents who need to wake their newborn for feedings or during feedings, suggest these strategies. ♣ Unwrap the newborn’s blanket. ♣ Massage his chest or back. ♣ Stroke the soles of his feet and the palms of his hands. ♣ Change his diaper. ♣ Sit him upright. ♣ Speak to him. o Parents are often concerned that their infant isn’t receiving enough nourishment from breastfeeding. Tell them to look for the following signs of adequate nutrition. ♣ Periods of contentment after feedings alternate with periods of wakefulness. ♣ The newborn feeds eight to 12 times in 24 hours. ♣ The newborn latches on easily and swallows audibly. ♣ The newborn has at least one wet diaper and one stool per day for the first 3 days, then six to eight wet diapers and at least three stools every 24 hours. ♣ The milk supply is “in” by the newborn’s third or fourth day. Breasts are full before feedings, and the mother feels the let-down, or milk ejection, sensation during feedings. ♣ The newborn has returned to his birth weight by 10 to 14 days. o Tell the parents not to feed their newborn formula or water unless there is some medical indication for it. They should also avoid the use of pacifiers for at least 1 month, when breastfeeding is well established. • Expressing and storing breast milk o Some patients wish to pump and store breast milk because of engorgement, to prepare feedings for others to give the newborn, or because they will be away from the newborn. This is also appropriate when the infant is premature or unstable and must remain in a neonatal intensive or special care unit after the mother goes home. Mothers can express breast milk by hand, with a manual pump, or with an electric pump. o Instruct these patients to store their breast milk in glass containers or plastic containers or bags free of bisphenol A (a chemical that hardens plastics) with the collection date on the label. To prevent waste, they should store only 60 to 120 mL (2 to 4 oz) in each container and should use the oldest milk first. They may keep freshly expressed breast milk at room temperature for up to 8 hours and in a refrigerator up to 8 days. They may store breast milk in the freezer of a two-door refrigerator for up to 6 months and in a separate freezer up to 12 months. Tell them to place breast milk containers in the middle or the rear of the refrigerator or freezer, and to thaw frozen breast milk in running water or in their refrigerator, never in a microwave oven. • Bottle feeding o Instruct parents to wash bottles in warm soapy water using a bottle and nipple brush and then to rinse them thoroughly. They do not need to boil them unless there are environmental risks, such as an issue with safety of the water supply. Postpartum Assessment • During postpartum, the time between delivery and the return of the reproductive system to its pre-pregnancy state, you’ll assess your patient’s vital signs, breasts, fundus, bladder, lochia, perineum, legs, and any incisions. • Measure vital signs with the frequency your facility’s policies specify or according to the provider’s prescription. Include temperature, heart rate, respiration, blood pressure, and pain level. Temperature may rise due to the dehydration that can accompany labor and sometimes as a result of epidural anesthesia. After the first 24 hours, however, elevations in temperature warrant further investigation as they suggest infection. Pulse rates may be somewhat elevated but should return to their pre-pregnant status gradually. A sustained rapid pulse can indicate hemorrhage. Respiratory rates may be low after epidural anesthesia and after a cesarean birth but should gradually return to the expected range. Orthostatic hypotension is common after delivery. Hypotension can indicate hemorrhage, and hypertension may persist in women who have had pre-eclampsia. • Assess your patient’s pain, including location, type, quality, and severity. Administer pain medication to keep the patient’s pain at a manageable level. For perineal pain, apply cold during the first 24 hours, including cool sitz baths. This helps reduce swelling and irritation. After the first 24 hours, warmth is helpful for promoting circulation and healing. To help reduce pain from sitting down, suggest that your patient compress or tighten her buttocks just before sitting. This reduces pressure on healing perineal tissues. • Encourage your patient to urinate prior to assessing her fundus. Assist her to a supine position. • First, inspect and gently palpate her breasts for redness, pain, and engorgement. Inspect the nipples for redness, cracks, and bleeding. If she is breastfeeding and her breasts are engorged, suggest warm compresses or a warm shower before breastfeeding to stimulate milk flow. Or, if her newborn isn’t emptying both breasts, suggest she pump her breasts to relieve discomfort. If she is not breastfeeding, suggest ice packs to help suppress milk production and reduce discomfort. • Next, check your patient’s fundus. Assess uterine height, location, and consistency. Determine the fundal height by placing one hand at the base of the uterus and the other at the umbilicus. Measure how many fingerbreadths, which are roughly equivalent to centimeters, you can place between the fundus and the umbilicus above or below it. If none, then the fundus is at the umbilical level. At 12 hours after delivery, the fundus is typically 1 cm above the umbilicus, but this does vary. The uterus descends into the pelvis approximately 1 to 2 cm per day. About a week after delivery, the fundus should be halfway between the umbilicus and the symphysis pubis. Also, assess whether the fundus is boggy or firm. If the fundus is boggy, gently massage the uterus with a rotating motion while supporting the lower uterine segment until it feels firm. Without stabilization of the lower segment, the uterus could invert, and severe hemorrhaging could result. • Assess and palpate the bladder at this time as well. Determine whether the fundus is at midline in the pelvis or displaced laterally due to a full bladder. If the bladder is full, encourage the patient to urinate and monitor her fluid intake and output. For some patients, insertion of a straight urinary catheter may become necessary. • Examine the patient’s perineal pad for bleeding, noting the character, quantity, presence of clots, and odor. Lochia rubra is typical 1 to 3 days following delivery, and small clots are common. Determine the amount of saturation as scant, light, moderate, heavy, or excessive. Be sure to check under the patient’s buttocks to be sure blood is not pooling beneath her. Lochia typically increases with breastfeeding and ambulation. If bleeding is excessive, the patient will soak an entire perineal pad within 15 minutes or so. For that finding as well as for numerous large clots or a foul odor, notify the provider immediately. • If the patient has had a cesarean delivery, examine the incision for redness, edema, ecchymosis, drainage, and approximation of its edges. If the patient has had an episiotomy, have her lie on her side and assess the episiotomy incision for approximation, edema, and ecchymosis. Also check her rectum for hemorrhoids and assess bowel function by auscultating bowel sounds. • Assess for thrombophlebitis by checking the patient’s calves for pain, tenderness, or redness. Notify the provider immediately if you find any of these. Check for edema of the hands, the face, and the lower extremities. • Finally, assess your patient’s comfort level and emotional status. Pregnancy • Pregnancy is a time of profound physiological and emotional change. It is beyond the scope of this skills module to present a comprehensive review of pregnancy. However, to meet your patient’s learning needs during its various trimesters, it is essential have to basic understanding of what she might experience during each of these phases. • The first trimester o When you first encounter a patient in her early weeks of pregnancy, she has probably just found out that she is pregnant. She may have any of a wide range of emotional responses and might not be prepared to take in a lot of information about pregnancy and childbirth at this time. Besides answering any questions she might have, your priority will be to point out any danger signs – indications she must report to her provider because they might warrant intervention. o Your patient’s first question is likely to be about when her baby will arrive. To calculate this, use Nӓgele’s rule. Take the first day of the woman’s last menstrual cycle, subtract 3 months, and then add 7 days and adjust the year as needed to make it a future date. So, if the first day of her last menstruation was November 20 of the current year, subtracting 3 months takes you to August, and adding 7 days and one year makes her “due date” August 27 of the following year. o Many women develop “morning sickness” during early pregnancy; indeed, your patient might tell you that she does feel nauseated from time to time. Make sure she knows to report severe vomiting, as it could be hyperemesis gravidarum, a serious complication that involves weight loss, fluid and electrolyte imbalances, and nutritional deficits. o Tell your patient to report abdominal cramping and any vaginal bleeding at all. In the first trimester, these could indicate miscarriage or ectopic pregnancy. o Another major consideration during the first trimester is infection. Burning with urination could mean a urinary tract infection. Diarrhea could mean a gastrointestinal infection. And fever and chills could indicate a systemic infection. All require prompt reporting and intervention. o Also instruct your patient to avoid taking any prescription or over-the-counter medications or supplements without first checking with her provider. Be sure she is aware of the dangers to her fetus from her ingestion of alcohol or other dangerous substances. • The second trimester o During the second trimester, many women undergo an ultrasound examination and find out their baby’s gender. It can be an exciting time, particularly as women feel their baby’s movement, or quickening, for the first time. Your patient may also look to you for help with some of the common discomforts of pregnancy that develop from her ever-expanding uterus. o The danger signs from the first trimester still apply; however, in this trimester, vaginal bleeding can also indicate placental problems such as placenta previa and abruptio placentae. Abdominal pain or cramping can mean preterm labor, and a sudden gush of clear fluid from the vagina indicates a rupture of the amniotic membranes – a serious complication this early in pregnancy. o Once a woman is accustomed to the pattern and frequency of fetal movement, she must report any significant increase or decrease. Either could be a fetal response to inadequate oxygenation. o At this time, be sure to instruct your patient to report any indications that her blood pressure has risen and she has developed pre-eclampsia. Classic manifestations include headache, vision changes, epigastric or abdominal pain, and edema, especially of the face and hands. o Gestational diabetes is another complication of pregnancy that manifests with specific warning signs. Instruct your patient to report the concurrent occurrence of flushed dry skin, fruity breath, rapid breathing, increased thirst and urination, and headache. These are manifestations of hyperglycemia. Clammy pale skin, weakness, tremors, irritability, and lightheadedness are manifestations of hypoglycemia. o It is also important at this time to teach your patient about the benefits of breastfeeding and of taking childbirth preparation classes. • The third trimester o During the third trimester, when women are preparing for the birth of their baby, they will want to know how they can tell the difference between “true” and “false” labor. o During true labor, your patient will have regular contractions that gradually become stronger and closer together. She will feel the pain of true labor in her lower back, and it will move forward across her lower abdomen. Her cervix will dilate and efface, and as the cervix dilates, she will pass what is called a bloody show vaginally and feel the baby moving down into the birth canal. o With false labor, contractions are usually irregular, although they can be regular for short periods. Walking and other activities will stop false labor, as will comfort measures and hydration. (These do not stop true labor.) And of course, with false labor, the cervix does not dilate and it does not efface. o The previous danger signs still apply, although after 37 weeks, ruptured membranes are likely to signal an imminent onset of term labor and not a danger sign of preterm labor. Apgar Scoring Apgar scoring is an assessment of five indications of a newborn’s physiologic state: heart rate, respiratory effort, muscle tone, reflex irritability, and color at 1 and at 5 min following birth. For heart rate, 0 means absent, 1 is slow (below 100/min), and 2 means above 100/min. This newborn scores 2 for a heart rate of 140/min. For respiratory effort, 0 means absent, 1 means slow or weak, and 2 reflects a good cry. This newborn scores 2 for crying loudly at delivery. For muscle tone, 0 is flaccid, 1 indicates some flexion of the extremities, and 2 is well flexed. This newborn scores 2 for well-flexed extremities. For reflex irritability, 0 means no response, 1 is a grimace, and 2 is a cry. This newborn scores 1 for grimacing when the nurse rubs the soles of his feet. For color, 0 is pale or blue, 1 reflects a pink body with blue extremities, and 2 means completely pink. This newborn scores 1 for being pink with mild acrocyanosis. Adding the newborn’s scores of 2, 2, 2, 1, and 1, this infant’s Apgar score at 1 min is 8. • [Show More]
Last updated: 2 years ago
Preview 1 out of 26 pages
Buy this document to get the full access instantly
Instant Download Access after purchase
Buy NowInstant download
We Accept:

Reviews( 0 )
$12.00
Can't find what you want? Try our AI powered Search
Document information
Connected school, study & course
About the document
Uploaded On
May 26, 2020
Number of pages
26
Written in

Additional information
This document has been written for:
Uploaded
May 26, 2020
Downloads
0
Views
92






 – University of the People.png)