ACRP CP Exam (GRADED A) Questions and Answers | 2023 | 100% Verified Answers
$ 10

California Permit Test Practice
$ 10

WISCONSIN PESTICIDE APPLICATOR PRACTICE TEST SOLUTION NEW UPDATE 2022
$ 10

Missouri Permit Practice Test | 30 Questions with 100% Correct Answers | Verified
$ 7

FAA Private Pilot Knowledge Test ACTUAL EXAM QUESTIONS AND ANSWERS 2022
$ 7.5

NY Learner's Permit Test (For Real) 2022 ( Questions with complete solution)
$ 10
.png)
NREMT Practice Exam Questions and Answers Already Passed
$ 10

DMV Written Test Class C-California-Complete Set- Multiple Choice
$ 10
.png)
NY Learner's Permit Test (For Real) 2022
$ 8

Missouri Driver Permit Test | 70 Questions with 100% Correct Answers | Verified
$ 6
PN Children Practice 2020 B - Questions, Answers and Rationale
$ 16

Contracting Officer Unlimited Warrant Board exam 2022/2023
$ 10
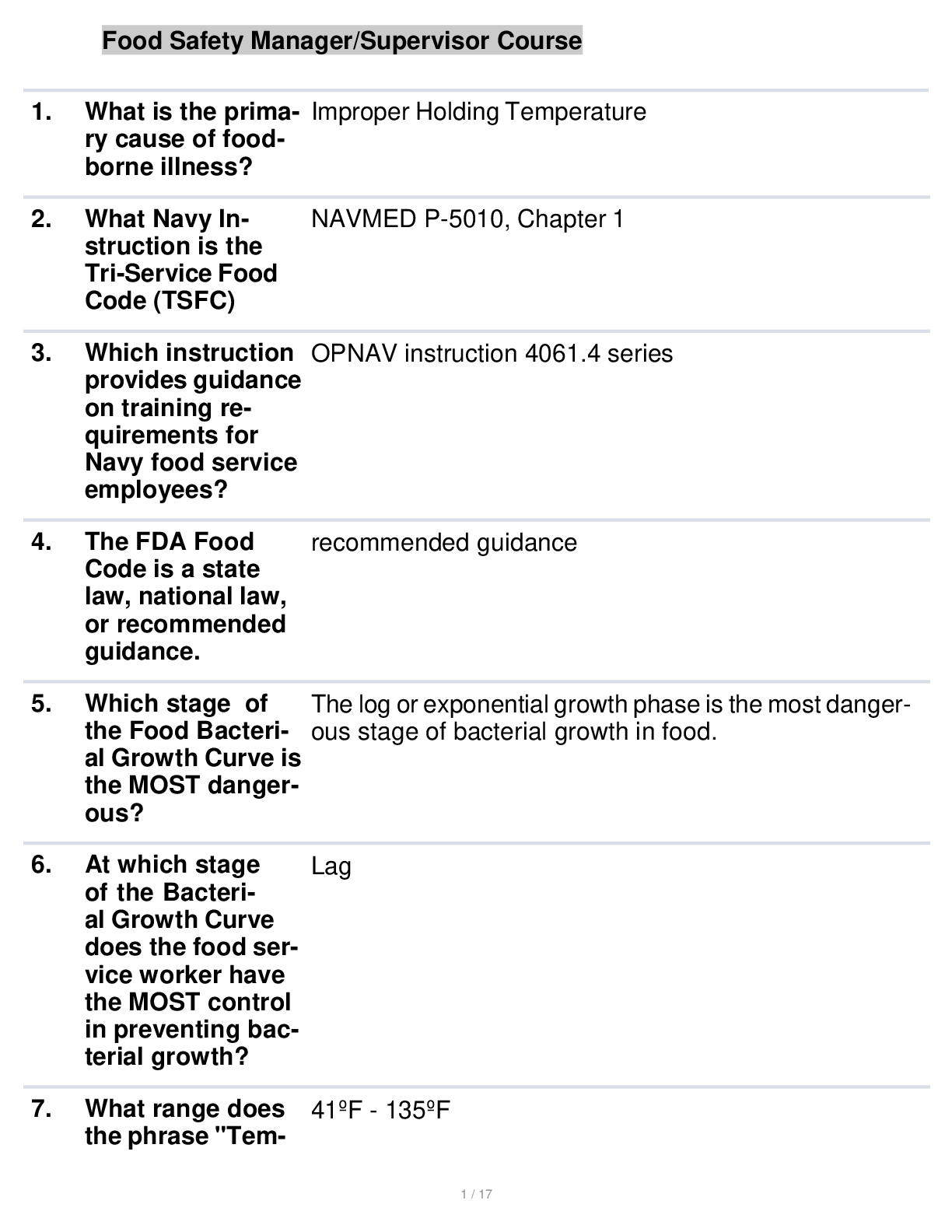
Questions And Answers Food Safety Manager/Supervisor Course
$ 11

[eBook‑PDF] Professional Issues in Speech‑Language Pathology and Audiology, 5th Edition by Melanie W. Hudson & Mark DeRuiter ISBN13: 9781635502206
$ 37.5
.png)
Official Permit Test DMV New York State 2022 with All Answers 100% Correct
$ 5

2025 Pearson Edexcel Level 3 GCE 8EL0/02 English Language and Literature Advanced Subsidiary PAPER 2: Varieties in Language and Literature Question Paper + Mark Scheme
$ 15
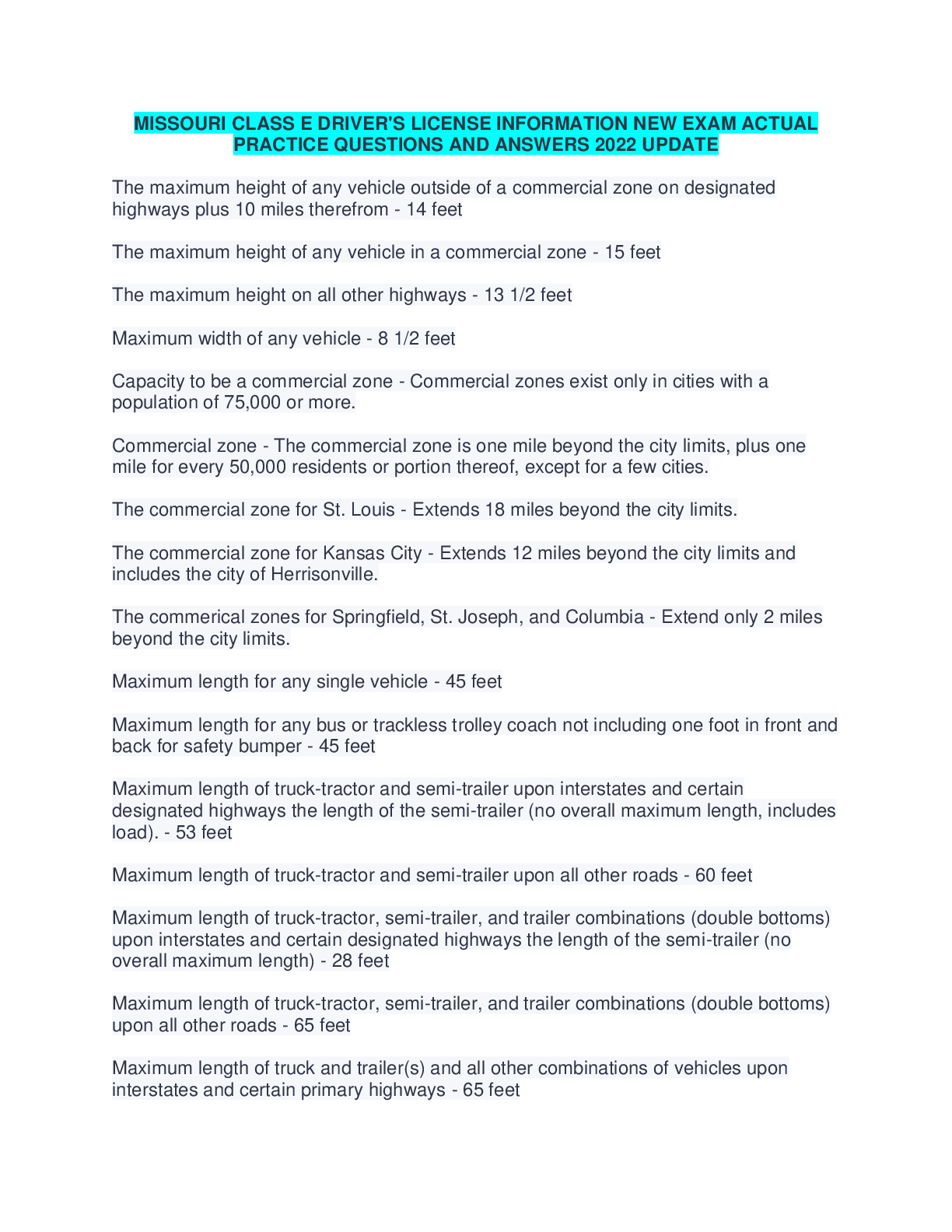
MISSOURI CLASS E DRIVER'S LICENSE INFORMATION NEW EXAM ACTUAL PRACTICE QUESTIONS AND ANSWERS 2022 UPDATE
$ 9
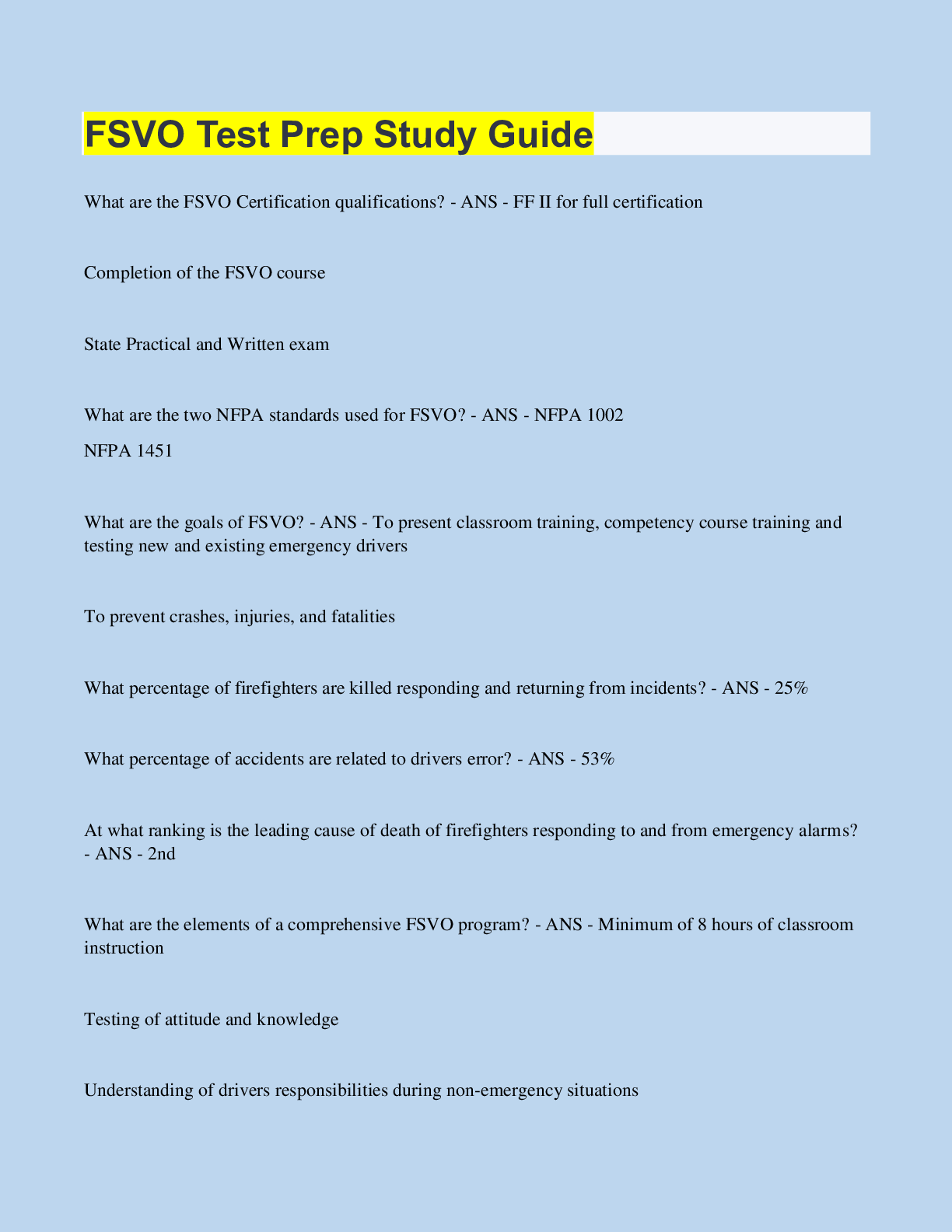
FSVO Test Prep Study Guide
$ 9
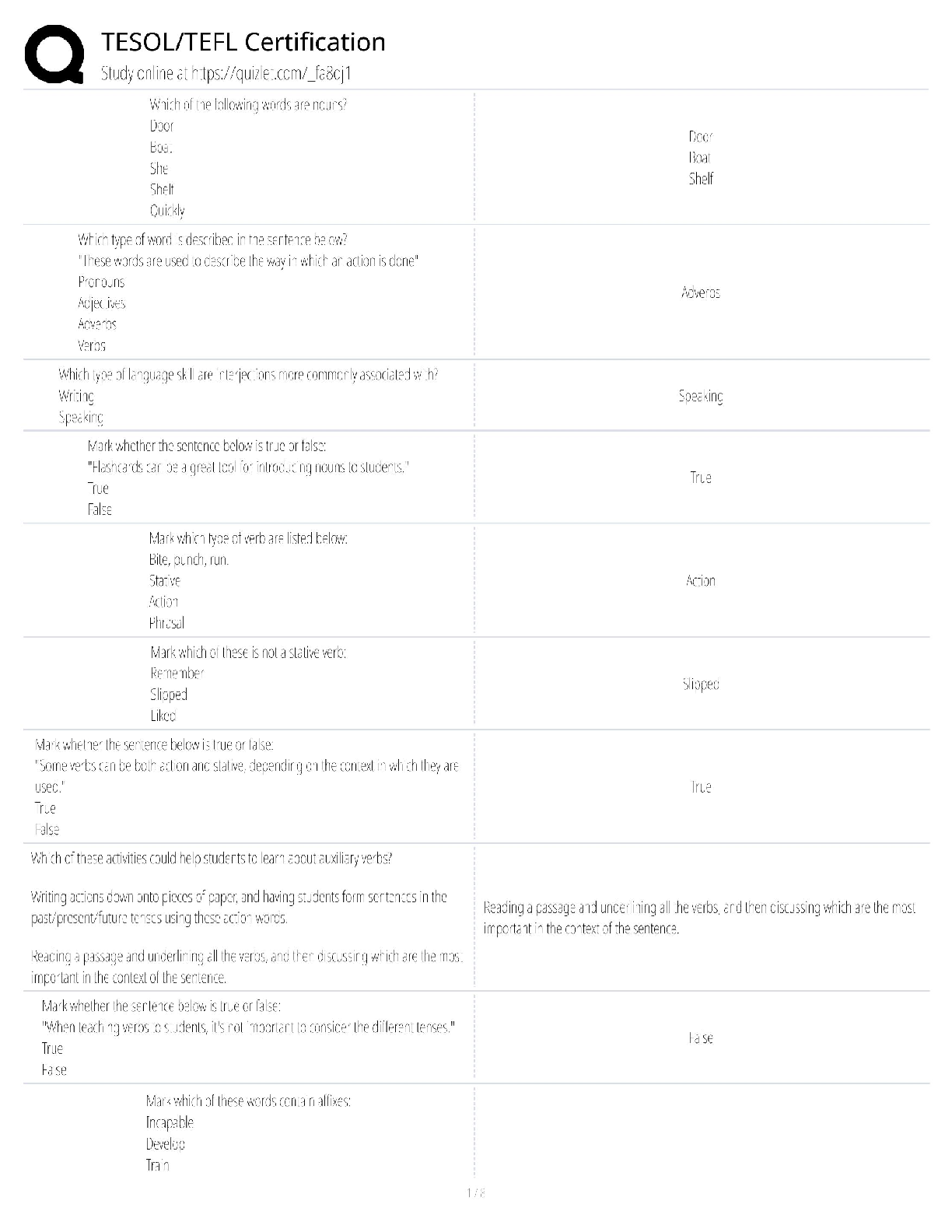
TESOL TEFL Certification / Teaching English Abroad / Study Guide / 2025 Update / Score 100%
$ 17
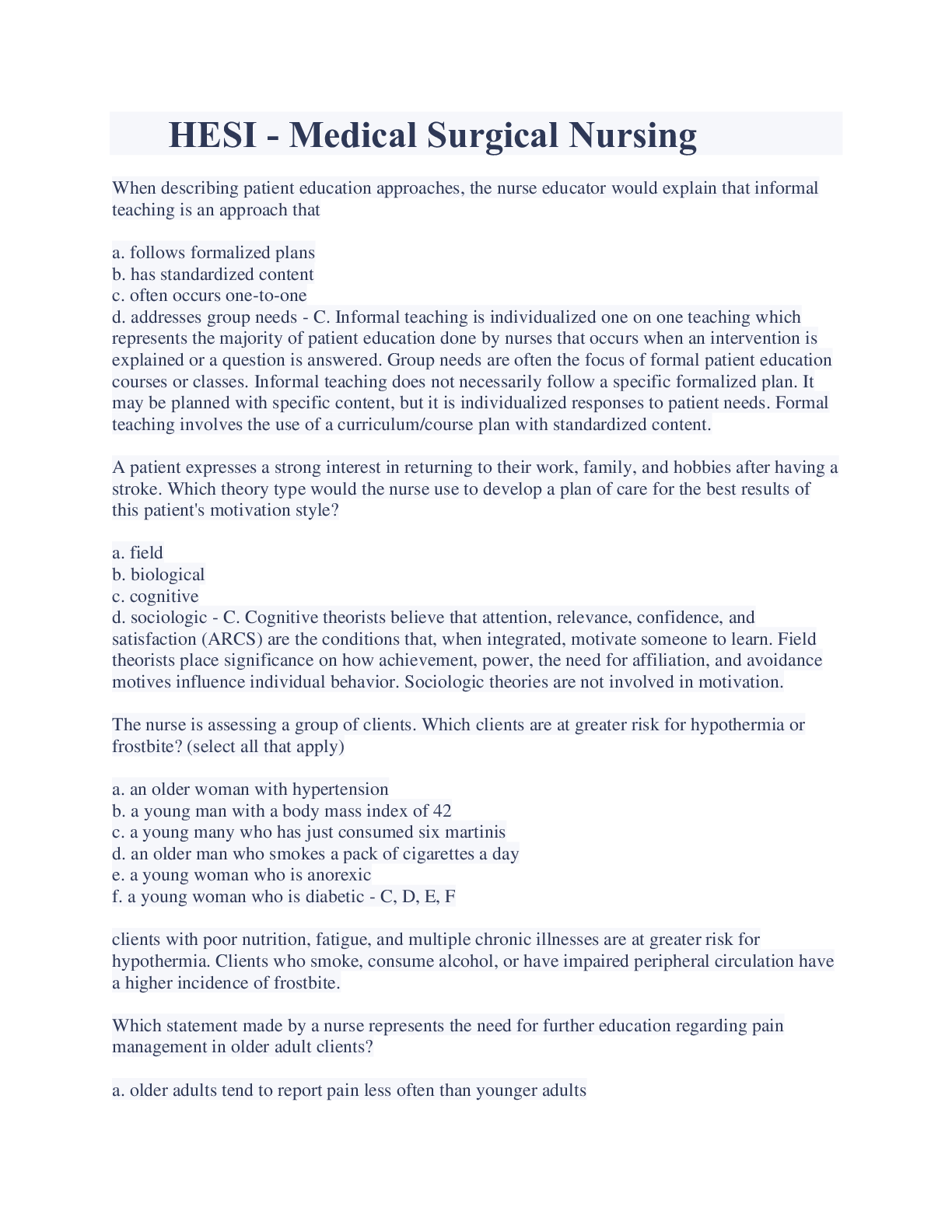
HESI - Medical Surgical Nursing Exam Verified A + Latest Updates
$ 15

APhA Immunization Exam Questions And Answers Latest Update With Complete Solution/ Download
$ 11.5
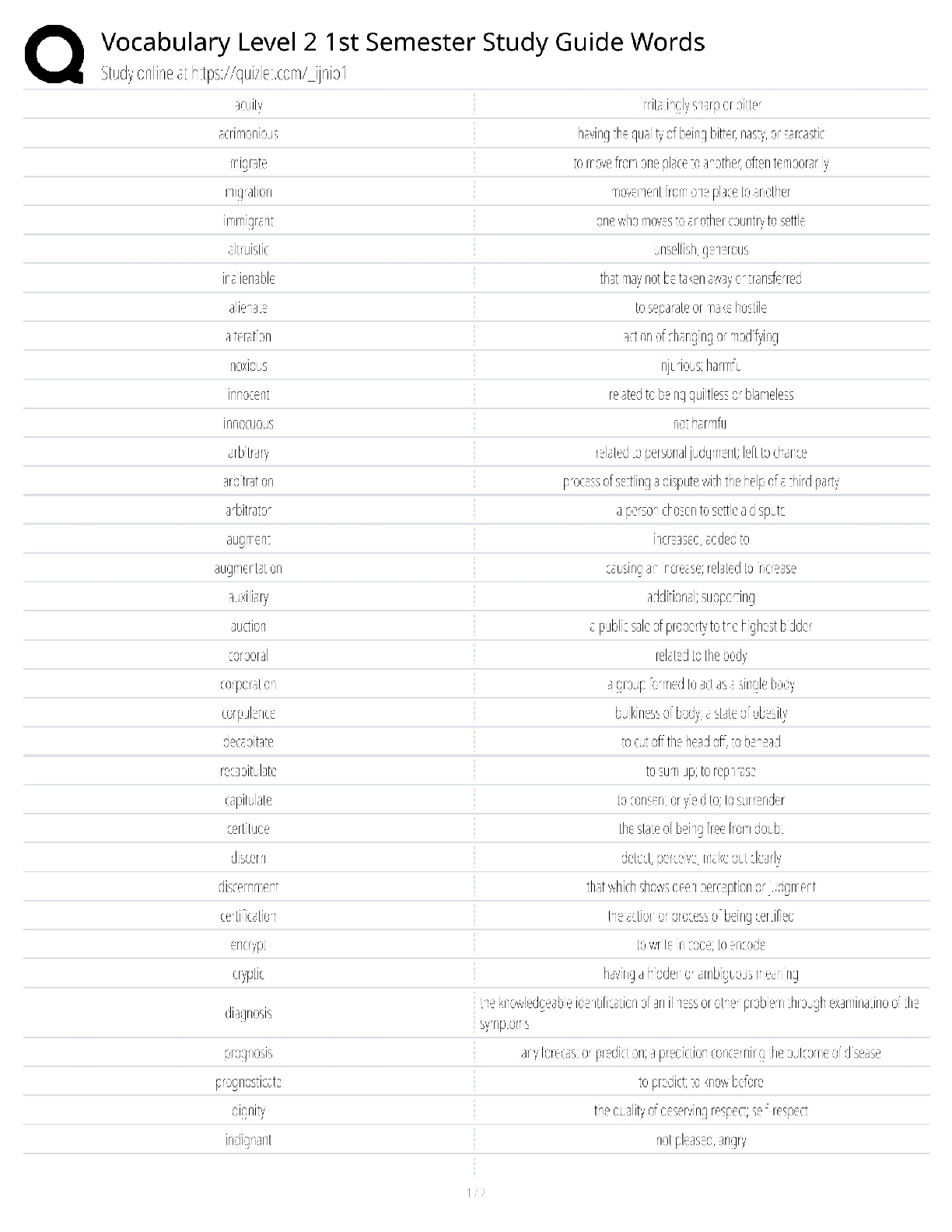
Vocabulary Level 2 1st Semester / Complete Study Guide & Word Mastery / Test Bank & Flashcards / Score 100% / 2025 Update
$ 18

Basic Life Support Exam A (Verified Answers)
$ 9
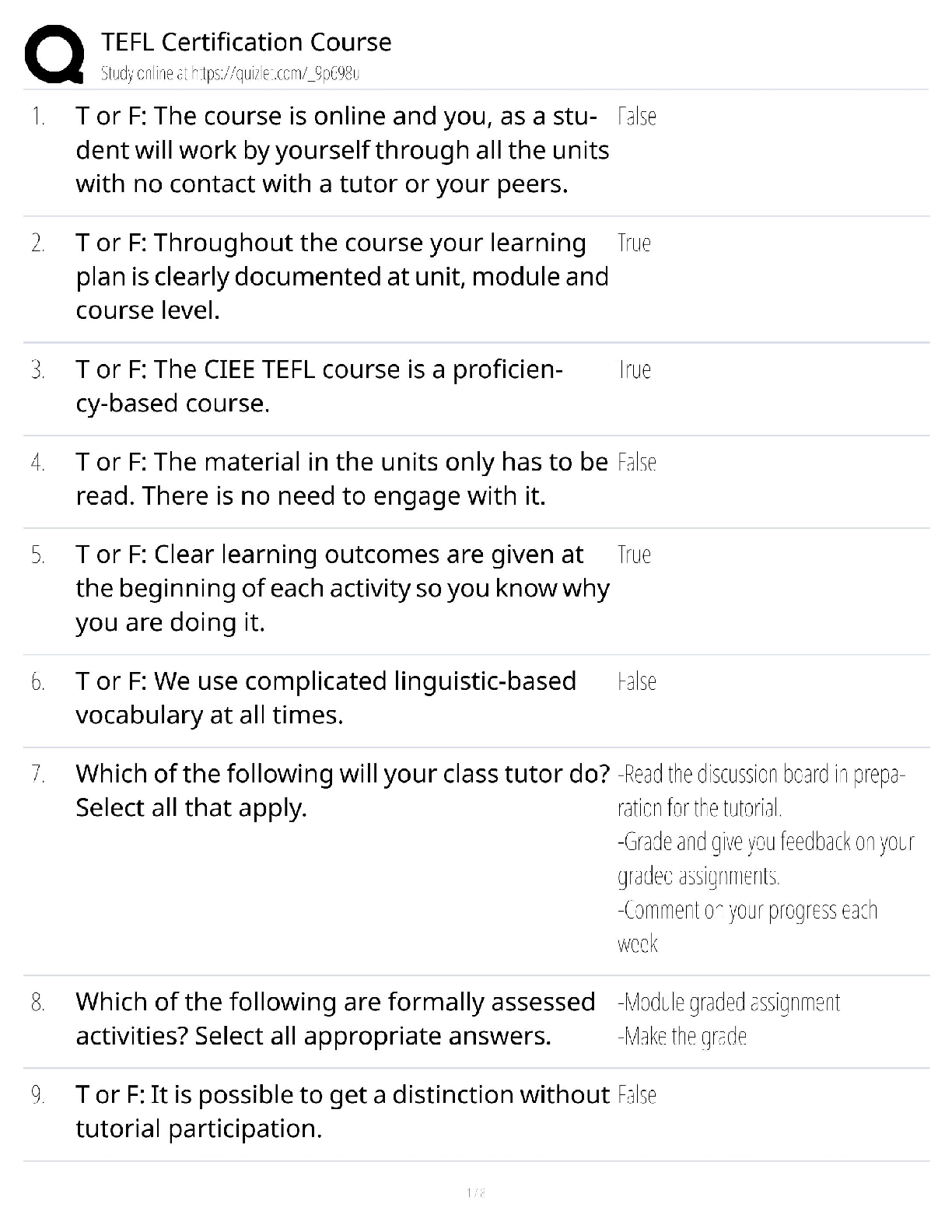
TEFL Certification Course & Exam Prep / 2025 Study Guide & Practice Test / Teach English Abroad
$ 21
TEFL Certification Course / Teaching English as a Foreign Language / Study Guide & Test Bank / Score 100% / 2025 Update



![Preview of [eBook] [PDF] Clinical Nursing Calculations 3rd Edition By Susan Sienkiewicz, Sandra Meg](https://browseimages.nyc3.digitaloceanspaces.com/paper-images/2025/Jul/04/4jF14r9I2025-07-04-05-586867ec3011731.png)