NURSING > QUESTIONS & ANSWERS > TNCC - Trauma Nursing Core Course Exam 2022 Study Guide (All)
TNCC - Trauma Nursing Core Course Exam 2022 Study Guide
Document Content and Description Below
Last updated: 3 years ago
Preview 1 out of 13 pages
Instant download
.png)
Buy this Document to get the Full Access Instantly
Provided by Students Who Aced it
We Verify Document Content to Gurantee Accuracy
Also available in bundle (1)
Click Below to Access Bundle(s)
.png)
BUNDLE, LATEST GRADED A COMPILATION. ALL TNCC IN ONE
TNCC Physical Assessments 2022/23 TNCC Written Exam 2022 (92 Questions with 100% Correct Answers) TNCC 8th edition exam with complete solution 2022 TNCC 8th Edition Questions and Answers (Updated 2...
By bundleHub Solution guider 4 years ago
$30
9
Reviews( 0 )
Document information
Connected school, study & course
About the document
Uploaded On
Jul 13, 2022
Number of pages
13
Written in
All
Seller

Reviews Received
Additional information
This document has been written for:
Uploaded
Jul 13, 2022
Downloads
0
Views
158
Document Keyword Tags
Recommended For You
Get more on QUESTIONS & ANSWERS »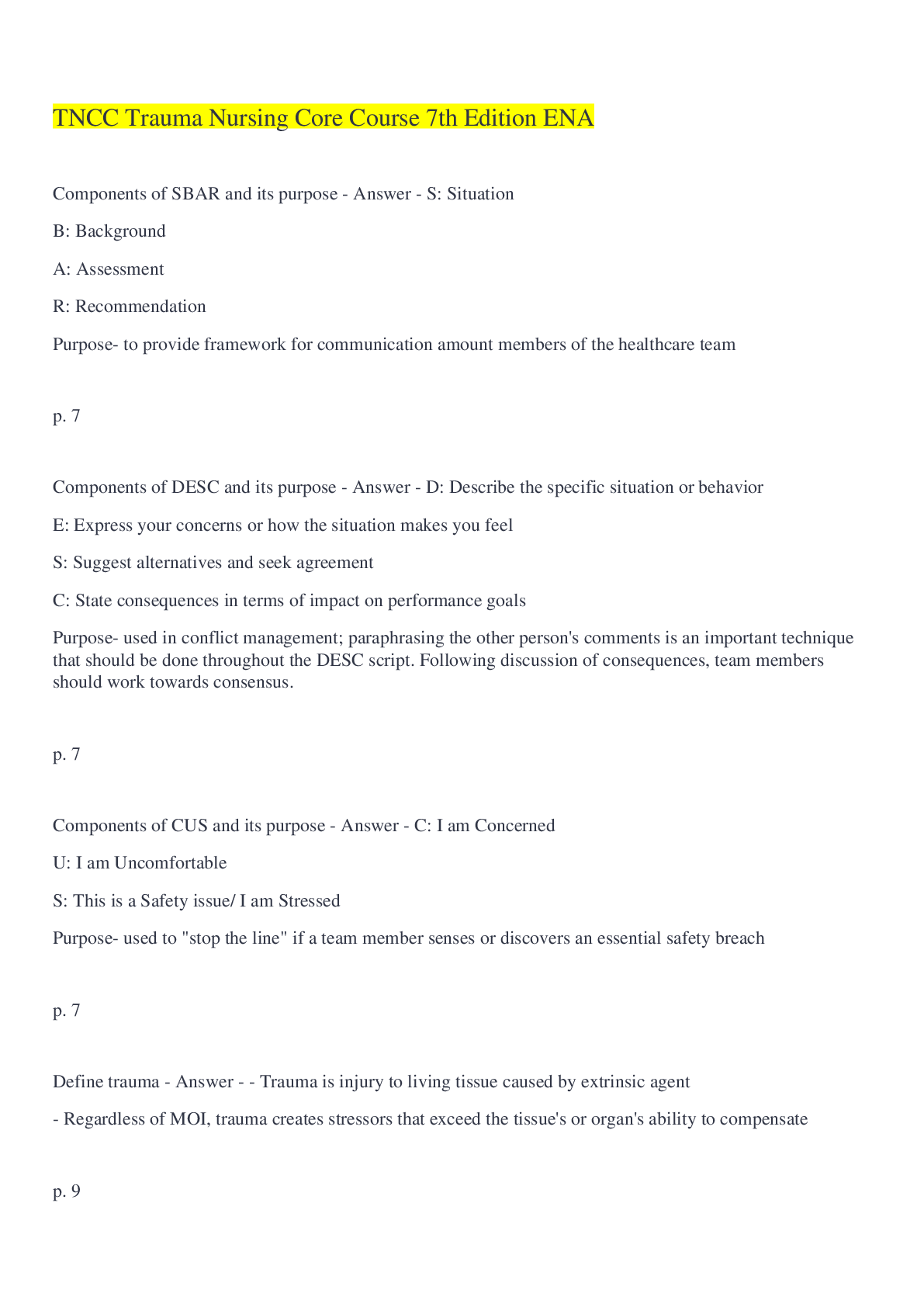
TNCC Trauma Nursing Core Course 7th Edition ENA. Questions and...


TNCC(Trauma Nursing Core Course) 8TH QUESTIONS AND VERIFIED AN...
Trauma Nursing Core Course|TNCC|Trauma Assessment|Questions wi...

Trauma Nursing Core Course|TNCC|Questions with 100% Correct A...
Trauma Nursing Core Course(TNCC)|Questions with 100% Correct A...
TNCC-Trauma Nursing Core Course Final Questions with Verified...
.png)
TNCC - Trauma Nursing Core Course Exam Latest Updated 2022 Stu...

Test Bank Trauma Nursing Core Course Provider Manual (TNCC) 7t...
TNCC Trauma Nursing Core Course Preparation Packet and Pre-Tes...

TEST BANK for Davis Advantage for Psychiatric Mental Health Nu...

Test Bank For Fundamentals of Nursing 11th Edition Potter Perr...

TEST BANK for Essentials of Psychiatric Mental Health Nursing:...