NSG 6435 Final Exam Study guide.
Know normal and abnormal findings; know expected risks, complications, signs/symptoms; physical exam findings; how to diagnose, treat, manage, educate patients/guardians, patho, and p
...
NSG 6435 Final Exam Study guide.
Know normal and abnormal findings; know expected risks, complications, signs/symptoms; physical exam findings; how to diagnose, treat, manage, educate patients/guardians, patho, and pharm for the following:
Varicella
Expected risks:
Never had the vaccine, never exposed to Varicella. More severe in adolescents and adults than younger children.
Those at risk include (MayoClinic 2019):
• Newborns of unvaccinated mothers or mother who never had chickenpox
• Adolescents and adults
• Pregnant women who haven’t had chickenpox or the vaccine
• Smokers
• Immunocompromised (chemo, HIV, ect.)
• Long term steroid use (as seen with asthma or COPD)
Complications:
Severe – cerebellar ataxia, encephalitis, viral pneumonia, hemorrhagic conditions (CDC, 2016). Secondary bacterial infections, pneumonia, encephalitis, hepatitis, and Reye syndrome (Hay, Levin, Deterding, Abzug, & Sondheimer, 2014, p.271)
Other – septicemia, toxic shock syndrome, necrotizing fasciitis, osteomyelitis, bacterial pneumonia, septic arthritis (CDC, 2016)
Physical findings (Signs/Symptoms):
Fever, loss of appetite, h/a, malaise (MayoClinic, 2019). Classic triad of low grade fever, malaise, and rash (Papadopoulos, 2018).
“Dew drops on a rose petal”; Rash – classic appearance, starts on scalp, face, or trunk Rash has 3 phases (MayoClinic, 2019):
1) raised pink bumps (papules), which break out over several days;
2) small fluid-filled blisters (vesicles), which form in about one day and then break and leak;
3) Crusts and scabs, which cover the broken blisters and take several more days to heal.
How to Diagnosis; Treatment; Management; Pharma
Diagnosis is based on S/S and presentation. Bloodwork and cultures of lesions can be done to confirm chickenpox (MayoClinic, 2019).
In younger children, symptomatic treatment only (Tylenol/Ibuprofen for fever, etc) (Papadopoulos, 2018).
Adolescents and adults, at increased risk, need a more aggressive treatment that can include PO or IV Acyclovir. Varicella-zoster immunoglobulin can be use in highly susceptible individuals (Papadopoulas, 2018).
Management includes (Cleveland Clinic, 2018):
• Cool, moist rag to rash
• Keep temperature down
• Try to prevent child from scratching (cut fingernails)
• Use lotion with an antihistamine on the rash and/or give OTC antihistamines
• Give cool bath or shower daily (can also give an oatmeal bath).
Education
Child can return to school 7 days after rash appears, does not have to wait until scabs are healed (Cleveland Clinic, 2018).
Chickenpox is contagious for about 2 days before a rash appears and is contagious until the vesicles have crusted over (roughly 1 week) (Nemours, 2019).
Keep child away from those at risk (newborns, pregnant women, elderly, immunocompromised).
Anyone who has had chickenpox has the potential to have shingles later in life (Nemours, 2019).
Someone with shingles can spread chickenpox but not shingles to those that have never had chickenpox or the vaccine (Nemours, 2019).
Patho
Acquired by inhaling airborne droplets from an infected host and infects the conjunctivae and mucosa of upper respiratory tract (Papadopoulos, 2018).
Humans are only known vector for chickenpox.
Viral proliferation in lymph node 2-4 post initial infection followed by primary viremia 4-6 post infection (Papadopoulos, 2018).
Measles
Expected risks:
Has a 90% secondary infection rate (Chen, 2019). Can affect people of all ages, although primarily thought of as a childhood illness (Chen, 2019).
Complications:
Rash can become hemorrhagic and can be fatal due to disseminated intravascular coagulation (DIC) (Hay et al., 2014, p. 515).
Bacterial superinfection and viral complications can manifest as a URI, obstructive laryngitis, otitis, diarrhea, mastoiditis, cervical adenitis, bronchitis, transient hepatitis, and pneumonia (Hay et al., 2014, p. 515).
Causative organism can be the measles virus or group A beta-hemolytic streptococci (Hay et al., 2014, p. 515).
Complications most likely in <5 and 20+
Physical findings (Signs/Symptoms):
Onset of 7-14 days post exposure with first s/s around 4-5 days (Hay et al., 2014, p. 515). There are 3 “C” of measles (Hay et al., 2014, p. 515):
1) Cough
2) Coryza – head cold, fever, sneezing
3) Conjunctivitis – pink eye
Koplik spots can be found on the oral mucosa opposite the lower molars and are pathognomonic of measles. They are bluish-white granules on an erythematous background.
Fever typically starts low to moderate (greater than 101 F) (Hay et al., 2014, p. 515).
A maculopapular rash generally appears at day 3-4, first appearing behind the ears and on the forehead, and the fever can rise to 105 at that point.
The rash moves down the body, engulfing the face, neck, and arms over 24 hours and to the back, abdomen, and thighs by 48 hours.
The more severe the rash, the more severe the illness.
How to Diagnosis; Treatment; Management; Pharma
To diagnose, the virus can be isolated in the urine, blood, throat, and/or nasopharyngeal secretions.
Serial IgG antibody titers that compare acute and convalescent serum specimens can also be done.
MEASLES IS A REPORTABLE DISEASE IN THE US WITHIN 24 HOURS OF DIAGNOSIS (Hay et al., 2014, p. 515).
Management/Care for exposed individuals includes receiving the vaccine within the first 72 hours of exposure (if eligible).
Can be given to infants between 6-11 months.
Immune globulin given within 6 days of exposure can prevent or modify the disease susceptible regardless of vaccination status.
Treatment is essentially supportive care – hydrate, keeping the fever under control, and Vit A supplements
Education
Keep infected child away from those very young, very old, pregnant, and immunocompromised (Nemours, 2019).
Keep them well hydrated, IV rehydration may be necessary.
The best way to keep a child safe from measles is to get the vaccine when they are 12 months old (Nemours, 2019).
Measles can be spread from 4 days before the rash is present to 4 days after the rash is present.
Patients are most contagious while they have a fever, runny nose, and cough (Nemours, 2019).
Patho
Measles has a peak incidence in late winter and spring (Chen, 2019).
It is transmitted via respiratory droplets and can remain active/contagious for about 2 hours on a surface.
2-4 days postinfection the virus infects local lymphatic tissues (Chen, 2019).
Mumps
Expected risks:
Complications:
Complications include:
• Meningoencephalitis
• Orchitis
• Oophoritis
• Pancreatitis
• Transverse myelitis
• Cerebellar ataxia
• Myocarditis
• Sensorineural hearing loss
Rare complications include nephritis, arthritis, thrombocytopenic purpura, mastitis, thyroiditis, and keratouvetis
Physical findings (Signs/Symptoms):
2 stages; prodromal and swelling.
Prodromal stage is rare in children but includes low-grade fever, h/a, anorexia, neck or other muscular pain, and malaise.
Swelling stage occurs about 24 hours after the prodromal stage and the patient will have painful selling of one or both parotid glands (Hays et al., 2014, p. 516).
Swelling can take a few hours or a few days and typically return to normal size in 3-7 days. RARELY will a maculopapular rash appear on the trunk.
When swelling is present the earlobes are pushed upward and outward (Ruiz, 2019). The opening of the Stensen duct can be edematous and erythematous (Ruiz, 2019). Submandibular and sublingual glands may also be swollen (Ruiz, 2019).
How to Diagnosis; Treatment; Management; Pharma
Can be diagnosed via a swab of the Stensen duct, throat washing, saliva, or spinal fluid through RT-PCR and serologic tests (Hay et al., 2014, p. 516)
Leukopenia with relative lymphocytosis and an elevated amylase are typical.
Test results are more reliable for diagnosis when specimens are obtained within 1-3 days after symptoms present (Hay et al., 2014).
Treatment includes plenty of fluids and soft food that don’t need chewing, or much chewing (Nemours, 2019).
Tylenol and Ibuprofen for the fever, NEVER aspirin.
Education
Patient is contagious from 3 days before the onset and up to 4 days after the start of active parotitis (Ruiz, 2019).
Drink plenty of fluids, avoid foods that need to be chewed.
Avoid tart or sour foods and drinks like orange juice or lemonade (Nemours, 2019). Use Tylenol or Ibuprofen to keep fever down (Nemours, 2019).
DO NOT GIVE ASPIRIN AS THIS HAS BEEN LINKED TO RYE SYNDROME (Nemours, 2019).
Mumps typically lasts about 2 weeks (Nemours, 2019).
Patho
The mumps virus is transmitted via respiratory droplets, direct contact, or contaminated fomites (Ruiz, 2019).
There is an incubation period of 14-18 days, the prodromal stage lasts 3-5 days after the incubation period, and the swelling stage last 3-7 days.
Rubella
Expected risks:
Complications:
Physical findings (Signs/Symptoms):
How to Diagnosis; Treatment; Management; Pharma
Education
Patho
Kawasaki disease
Expected risks:
Complications:
Physical findings (Signs/Symptoms):
How to Diagnosis; Treatment; Management; Pharma
Education
Patho
Hand-mouth-foot-disease
Expected risks:
Complications:
Physical findings (Signs/Symptoms):
How to Diagnosis; Treatment; Management; Pharma
Education
Patho
Fifth disease
Expected risks:
Complications:
Physical findings (Signs/Symptoms):
How to Diagnosis; Treatment; Management; Pharma
Education
Patho
Splenomegaly
Expected risks:
Complications:
Physical findings (Signs/Symptoms):
How to Diagnosis; Treatment; Management; Pharma
Education
Patho
Pancreatitis
Expected risks:
Complications:
Physical findings (Signs/Symptoms):
How to Diagnosis; Treatment; Management; Pharma
Education
Patho
Depression
Expected risks:
Complications:
Physical findings (Signs/Symptoms):
How to Diagnosis; Treatment; Management; Pharma
Education
Patho
Anxiety
Expected risks:
Complications:
Physical findings (Signs/Symptoms):
How to Diagnosis; Treatment; Management; Pharma
Education
Patho
Milestones – infant, toddler, school-aged, and adolescents
By 3 months – infant can raise head and roll to sides
By 4-6 mon – infant can roll back to side, and abd to back 8 mon – can sit up unsupported
8-10 mon – develop pincher grasp and may crawl/creep 10-12 mon – can say mama/dada/byebye
15 mon – should have a 15 word vocab By 2 yrs – should have 200 word vocab
Musculoskeletal disorders from school-age child to the adolescent
Tanner staging
Female:
Tanner stage 1 – No glandular breast tissue palpable
Tanner stage 2 – Breast bud palpable under areola (1st pubertal sign in females) Tanner stage 3 – Breast tissue palpable outside areola; no areolar development
Tanner stage 4 – Areola elevated above contour of the breast, forming “douple scoop” appearance
Male:
Tanner stage 1 -prepubertal; testicular size less than 4 cc and 2.5 cm is that longest dimension
Tanner stage 2 – enlargement of scrotum and testes; scrotal skin reddens and schanges in texture; growth of testes to 4 cc or larger
Tanner stage 3 – enlargement of penis (length at first); further growth of testes
Tanner stage 4 – increased size of penis with growth in breadth and development of glans, testes and scrotum larger, scrotal skin darker
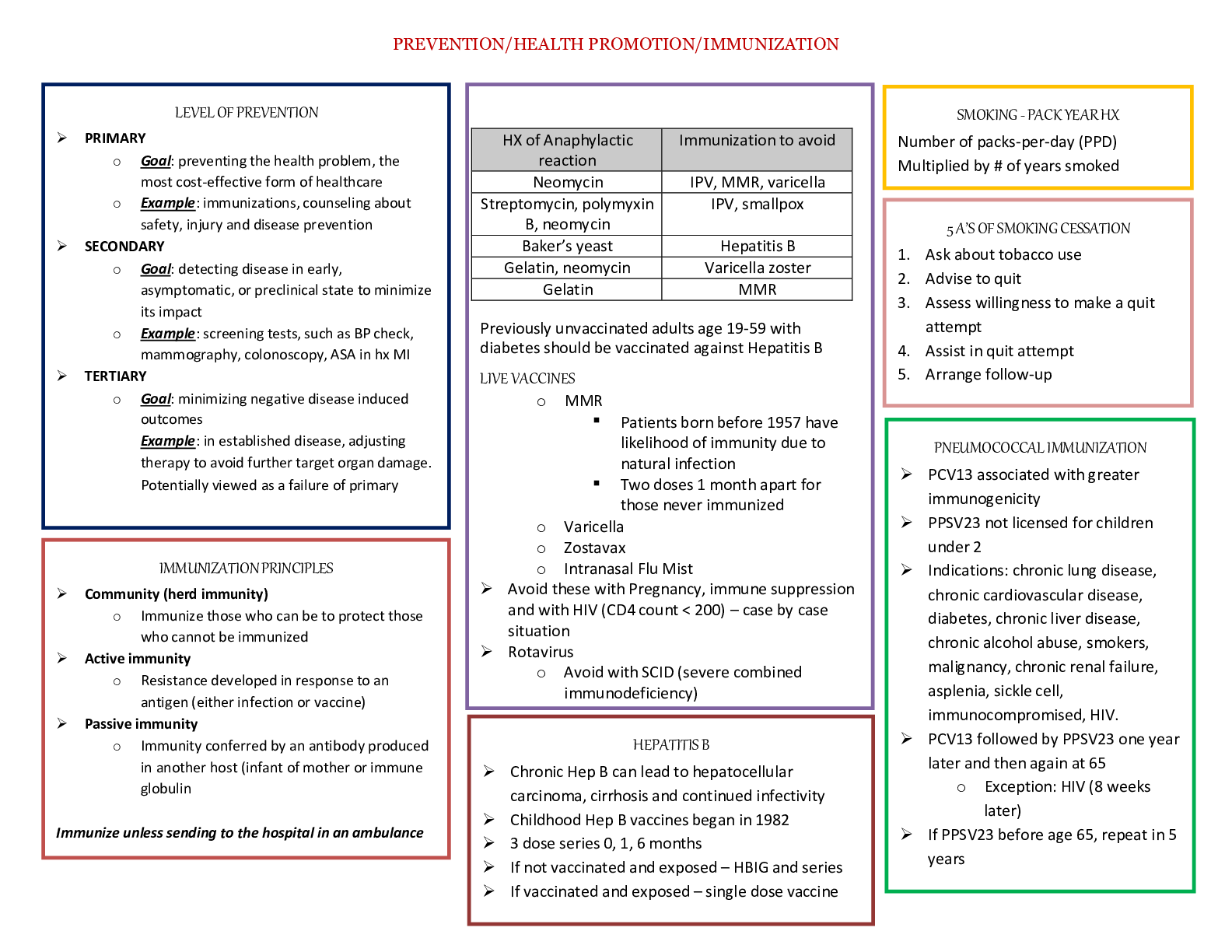
Immunizations/Vaccinations – when, why they should be administered
Hep-B – First dose at birth, second dose at 1-2 months, 3rd dose at 6 months (CDC, 2020). To prevent Hep-B in child and adulthood (Nemours, 2019).
Pneumococcal – 1st dose at 2 mon, 2nd at 4 mon, 3rd at 6 mon, and 4th at 12 mons (CDC, 2020). Used to prevent pneumonia and some incidence of AOM.
HiB – 1st dose 2 mons, 2nd dose 4 mons, 3rd/4th dose 12 mons. To prevent AOM, meningitis, pneumonia, pericarditis, and infections of the blood, bones, and joints by bacteria (Nemours, 2019).
DTaP – 1st dose at 2 mon, 2nd at 4 mon, 3rd at 6 mon, and 4th at 15 mons (CDC, 2020). To eliminate diphtheria and tetanus in childhood and reduce the number of pertussis cases (Nemours, 2019).
Rotavirus – 1st dose at 2 mon and 2nd at 4 mon (CDC, 2020). To decrease severe dehydration with GI virus (Nemours, 2019).
Inactivated poliovirus – 1st dose at 2 mons, 2nd dose at 4 mons, and 3rd dose at 6 mons (CDC, 2020). To prevent paralysis and death from poliovirus (Nemours, 2019).
Varicella – given at 12 months; is a live attenuated virus; used to prevent severe varicella; a second dose is needed at 18 months or 4-6 years (Hay, Levin, Deterding, Abzug, & Sondheimer, 2014, p.271).
MMR (measles, mumps, rubella) – first dose at 12 months, second dose at 4-6 years (can be given 4 weeks apart) (CDC, 2020). Used to prevent MMR and reduce spread of the diseases, prevent hearing loss.
Anticipatory guidance and safety from infancy to adolescence
HEENT disorders
Otitis media
Otitis externa
Allergies
Conjunctivitis
Pharyngitis
strep throat – and complications
Meningitis
Genetic conditions of X and Y chromosome-combinations Sports Physicals
References
DTaP
Nemours. (2019). Your child's immunizations: Diphtheria, Tetanus & Pertussis Vaccine (DTaP). Retrieved from: https://kidshealth.org/en/parents/dtap-vaccine.html
Hep-B
Nemours. (2019). Your Child's Immunizations: Hepatitis B Vaccine (HepB). Retrieved from: https://kidshealth.org/en/parents/hepb-vaccine.html
Hib
Nemours. (2019). Your child’s immunizations: Hib vaccine. Retrieved from: https://kidshealth.org/en/parents/hib-vaccine.html
Measles
Chen, S.S.P. (2019). Measles. Retrieved from: https://emedicine.medscape.com/article/966220- overview
Hay, W., Levin, M., Deterding, R. Abzug, M. & Sondheimer, J. (2014). Current Diagnosis and Treatment: Pediatrics, (23rd ed.). Mc-Graw Hill.
Nemours. (2019). Measles. Retrieved from: https://kidshealth.org/en/parents/measles.html
Meningitis
Mumps
Hay, W., Levin, M., Deterding, R. Abzug, M. & Sondheimer, J. (2014). Current Diagnosis and Treatment: Pediatrics, (23rd ed.). Mc-Graw Hill.
Nemours. (2019). Mumps. Retrieved from: https://kidshealth.org/en/parents/mumps.html
Ruiz, C.C. (2019). Acute mumps. Retrieved from: https://emedicine.medscape.com/article/784603-overview#showall
Poliovirus
Nemours. (2019). Your child’s immunizations: Polio vaccine (IPV). Retrieved from: https://kidshealth.org/en/parents/polio-vaccine.html
Rubella
Splenomegaly
Varicella
CDC. (2018). Chickenpox (Varicella). Retrieved from: https://www.cdc.gov/chickenpox/hcp/index.html?CDC_AA_refVal=https%3A%2F
%2Fwww.cdc.gov%2Fchickenpox%2Fhcp%2Fclinical-overview.html
CDC. (2020). Immunization schedule. Retrieved from: https://www.cdc.gov/vaccines/schedules/hcp/imz/child-adolescent.html
Cleveland Clinic. (2018). Chickenpox: Management and treatment. Retrieved from: https://my.clevelandclinic.org/health/diseases/4017-chickenpox/management-and-treatment
Hay, W., Levin, M., Deterding, R. Abzug, M. & Sondheimer, J. (2014). Current Diagnosis and Treatment: Pediatrics, (23rd ed.). Mc-Graw Hill.
MayoClinic. (2019). Chickenpox. Retrieved from: https://www.mayoclinic.org/diseases- conditions/chickenpox/symptoms-causes/syc-20351282
Nemours. (2019). Chickenpox. Retrieved from: https://kidshealth.org/en/parents/chicken- pox.html
Papadopoulos, A.J. (2018). Chickenpox. Retrieved from: https://emedicine.medscape.com/article/1131785-clinical
[Show More]





.png)