*NURSING > EXAM REVIEW > NR 283 Week 3 Examination 1 (Concepts to Review) (All)
NR 283 Week 3 Examination 1 (Concepts to Review)
Document Content and Description Below
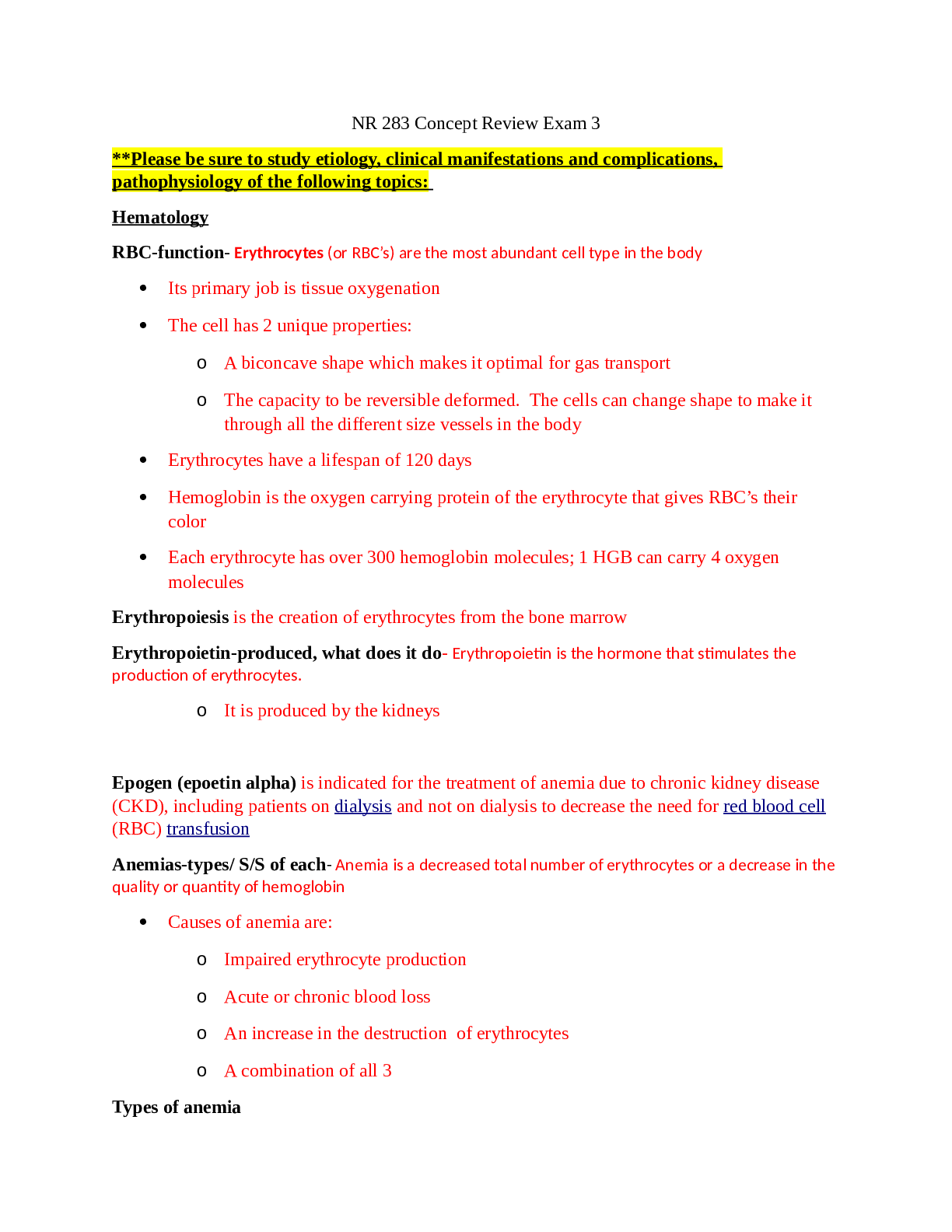
NR 283 Concept Review Exam 3 **Please be sure to study etiology, clinical manifestations and complications, pathophysiology of the following topics: Hematology RBC-function- Erythrocytes (or RBC’... s) are the most abundant cell type in the body • Its primary job is tissue oxygenation • The cell has 2 unique properties: o A biconcave shape which makes it optimal for gas transport o The capacity to be reversible deformed. The cells can change shape to make it through all the different size vessels in the body • Erythrocytes have a lifespan of 120 days • Hemoglobin is the oxygen carrying protein of the erythrocyte that gives RBC’s their color • Each erythrocyte has over 300 hemoglobin molecules; 1 HGB can carry 4 oxygen molecules Erythropoiesis is the creation of erythrocytes from the bone marrow Erythropoietin-produced, what does it do- Erythropoietin is the hormone that stimulates the production of erythrocytes. o It is produced by the kidneys Epogen (epoetin alpha) is indicated for the treatment of anemia due to chronic kidney disease (CKD), including patients on dialysis and not on dialysis to decrease the need for red blood cell (RBC) transfusion Anemias-types/ S/S of each- Anemia is a decreased total number of erythrocytes or a decrease in the quality or quantity of hemoglobin • Causes of anemia are: o Impaired erythrocyte production o Acute or chronic blood loss o An increase in the destruction of erythrocytes o A combination of all 3 Types of anemia • pernicious anemia -It is caused by a vitamin b12 deficiency • The main problem is the absence of intrinsic factor which is an enzyme needed to absorb vitamin b12 in the stomach • Absence of this factor can be genetic or can be related to problems with the stomach • P.A. is most commonly caused by people who have had their stomach or a part of their stomach removed, however a history of alcohol use or smoking can cause it as well • PA takes years to develop so initial symptoms can be very non-specific • When your hemoglobin starts to be affected (when it decreases) symptoms include weakness, fatigue, and paresthesia’s of feet and hands folate deficiency anemia • Folate is another vitamin necessary for DNA synthesis of erythrocytes • Folate deficiency anemia is commonly seen in alcoholics and malnourished people • With this type, there is no enzyme responsible for making sure we absorb the folate. We are strictly lacking an adequate amount • Folate is found in dark, leafy green vegetables, citrus fruits, beans and nuts o Folic acid is a synthesized form of folate • Clinical manifestations include: o Cheilosis - fissures and scales in the mouth o Stomatitis- inflammation of the mouth painful ulcers of the tongue Iron deficiency anemia- is the most common type of anemia • There are many causes, including insufficient iron in the diet, certain medications, excessive menstrual bleeding in females, or ulcer’s • Iron is important because it is used for the production of HGB • The development occurs slowly through 3 stages: o Body’s iron stores are depleted. Normal blood cell production occurs o Now insufficient amounts of iron are transported to the marrow where iron deficit RBC’s are produced with low amounts of HGB o The HGB deficient cells enter circulation to replace the normal aging cells that are getting ready to die • Clinical manifestations start occurring at stage 3 • Early symptoms are non-specific including fatigue, weakness, and SOB • As it become more severe, clinical manifestations can include: o Koilonychias - the fingernails become brittle and concave or spoon shaped o the tongue becomes sore and reddened o the corners of the mouth become dry and sore Sideroblastic anemia -is another type of anemia • It is characterized by a problem with the synthesis or creation of HGB • In SA, there is plenty of iron, but it is not used correctly to make the HGB • The erythrocytes end up with a little bit of HGB and a circle of iron in the RBC itself • SA’s can be classified as: o Acquired: the most common and are idiopathic (no known cause) o Hereditary: this is rare and is almost always found in men o Reversible: this is associated with alcoholism because the alcohol impairs heme synthesis • CM’s include those commonly seen with anemia • These people will also have signs of a syndrome called hemosiderosis or iron overload Enlarged liver/spleen, deposits of iron in heart affecting its function Polycythemia Vera- polycythemia which is the term for an excess production of RBC’s • There are many forms of Polycythemia • The main one I will focus on is primary absolute polycythemia, also known as Polycythemia Vera. • The main cause is unknown but thought to be due to a genetic alteration of the erythrocyte receptor o So the receptor is not sensing that there are enough circulating erythrocytes and just keeps producing them • The clinical manifestations of PV are due to an increase in the viscosity or thickness of the blood o The number of blood cells increase in the vessel but the amount of plasma or fluid does not so you have an overcrowded vessel which makes the blood very thick • This can cause clogging and occlusion of blood vessels (think congested highways) • Tissue injury and death are common as well as a high risk of developing blood clots • Another CM is plethora which is a ruddy, red coloring to the face, hands, and mucous membranes • A unique CM of PV is a very intense painful itching that only gets worse with exposure to heat or water • We mentioned that people with PV also have splenomegaly. Why? What is the spleen’s job? o Remember the spleen’s job is to filter and clean the blood. The more blood you have the harder the spleen has to work, so it grows bigger. o Remember cellular adaptations? Would this be atrophy or hypertrophy? Pathologic or physiologic? Pathologic because it is getting bigger due to an abnormal increase in erythrocytes • Secondary polycythemia is another form and results from an increased secretion of erythropoietin from chronic hypoxia (such as people who live at high altitudes where there is less oxygen or patient’s with COPD) • We said that if your body senses that you are hypoxic, it will secrete more erythropoietin to create more RBC’s to get more oxygen to the tissues. This is the same thing WBC-quantitative and qualitative-causes- Quantitative alterations refers to an increase or decrease in the amount of leukocytes . Quantitative disorders include: • Leukocytosis is an increase in the amount of circulating leukocytes • This is a normal response to infection, medications, stress, and medications • Neutrophilia is an increase in the number of neutrophils specifically • It is seen in the early signs of infection or inflammation • Lymphocytosis is an increase in the number of lymphocytes • Typically seen in viral infections • Leukopenia is a lower than normal amount of circulating leukocytes • This can occur in relation to autoimmune diseases or cancer treatments. • This is not normal and put someone at a high risk for developing infections • Neutropenia is a decrease in the number of neutrophils • This can be associated with long term infections in which the body runs out of neutrophils • Lymphycytopenia is a decrease in the number of lymphocytes • Is associated with immune deficiencies • Can also be related to destruction of the cells from a virus or drug Qualitative alterations affect the ability of the cell itself to function correctly • qualitative disorders of leukocytes, starting with leukemia • Which is a malignant (cancer) disorder of the blood and the blood forming organs • The common feature of leukemia is an uncontrolled growth of malignant leukocytes (leukemic cells) that cause an overcrowding of cells in the bone marrow • Because of the overcrowding, pancytopenia (decreased production of all cells) can occur • The exact cause of leukemia is unknown but there are risk factors and genetic alterations that are associated with it • Leukemia tends to appear in families • It also is common in someone who already has a genetic alteration like: o Down’s Syndrome o Gene translocations ▪ When two chromosomes break and switch information Other risk factors seen with leukemia include smoking, exposure to radiation, and certain drugs and infections Hodgkin- In Hodgkin Lymphoma a group of B lymphocytes become mutated and grow into abnormally large cells that spread throughout the lymphatic system causing systemic problems • Specifically it is the B lymphocyte that is mutated • The abnormal B cells, known as Reed Sternberg cells, are the characteristic sign of HL • The exact mutation that occurs and why is still unknown • However there are some known risk factors for HL that include a history of Mono from the Epstein Barr virus, Family history, male gender, people who are immunocompromised, and age (common 15-35, and 55+) • Clinical manifestations of H.L. typically involve NONPAINFUL enlarged lymph nodes that typically start in the neck and are the first sign of H.L. • Other CM’s include fever without signs of infection, pruritus, and fatigue and Non- Hodgkin lymphoma, differences Non-Hodgkin’s lymphoma is actually a general term used to describe lymphomas of other types of lymphocytes (B, T, and NK lymphocytes) • They are different from H.L. in that they : • don’t have the reed-Sternberg cells • their cellular changes are different • But they are both cancers of the lymphocytes of the lymph system • Like other cancers, NHL come from gene mutations, specifically gene translocations • Risk factors for NHL include family history, exposure to chemicals, certain viruses, and immunosuppression • NHL is more common than HL, and typically does not show up until later in life • CM’s usually start with painless swelling of lymph nodes other than the neck. The swelling can occur over months to years. Other CM’s can include abdominal or bone pain • One specific type of NHL is Multiple myeloma Infectious Mononucleosis- Infectious mononucleosis is an infection of a specific type of lymphocyte called a B lymphocytes by the Epstein Barr virus • This is known as the kissing disease and is common in colleges because it is transmitted through saliva from close personal contact • The infection starts when the EBV attacks some of the B lymphocytes and damage and destroy them • Unaffected B cells will produce antibodies against the EBV and then attack it. • This is why the disease is self-limiting because it can stop it itself • Initial CM’s include flu-like symptoms such as fever, fatigue, and joint pain As mono progresses, lymph nodes can get bigger Multiple Myeloma- is the growth of malignant plasma cells (type of WBC) that invade bone marrow and form into tumors inside of bones • The cells have been mutated by chromosome translocations or deletions • Once a large enough group of cells aggregate together, they enter the bone and activate osteoclasts that break down the bone and release the calcium into the circulation. • These malignant plasma cells also like to circulate through the blood and make their way into other bones o So you can have these myelomas throughout your body breaking down bone and tissue • Also, normally our plasma cells produce antibodies that help us fight infections • These myeloma cells produce antibodies but they are ineffective and cause the individual to have problems fighting infections • The most common CM is an increased level of calcium in the blood • Other CM’s seen are pain and renal failure as a result of protein in the urine and bone fractures from the destruction of the bone ALTERATIONS IN PLATELETS • Thrombocytopenia is a decreased platelet count • It can be caused by a decreased production or an increase in consumption of platelets There are 3 types of thrombocytopenia • HIT or Heparin Induced Thrombocytopenia- Heparin is a medication known as an anti-coagulant. It thins the blood enough to prevent the production of blood clots • HIT is actually a severe drug reaction that is mediated by the immune system • In HIT, the body creates antibodies against the heparin • These antibodies bind to a protein found on the platelet. • The antibody will tell the platelets to aggregate, form a thrombus or clot, and decrease platelet count • Often this does not show up until days after the heparin has been given • The hallmark sign of HIT is thrombocytopenia that occurs gradually over a matter of days • If HIT is not treated right away it can cause people to rapidly develop multiple thrombi which will put them at risk for DVT’s, PE’s, strokes or heart attacks ITP-cause, S/S- ITP or idiopathic thrombocytopenic purpura is another type • The cause of ITP is unknown, but it is some kind of abnormality with our immune response • For some reason a large amount of antibodies are produced in the blood against thrombocytes • These antibodies will bind to antigens on the surface of the platelet • These specific antibody bound platelets are removed from the circulation and destroyed by the spleen • CM’s range from minor bleeding issues (purpura and petechiae) to major hemorrhage in a matter of days. • Purpura are purple bruises. Petechiae are pinpoint sized red/purple dots on the skin TTP-cause, S/S- TTP or thrombotic thrombocytopenia purpura is a third type of thrombocytopenia • This one specifically is a life threatening disorder • It is either a genetically inherited disease, or it can be acquired from either an unknown trigger, or such things as lupus or pregnancy • It is characterized by thrombotic microangiography which is a disorder of clot formation in capillaries and arteries due to tissue injury o Platelets will spontaneously aggregate o Form micro-thrombi or mini blood clots that rest in arteries and capillaries o And stop blood flow to a specific area of the body • A decrease in circulating platelets has occurred because they are all being used to create mini clots throughout the body • These mini clots can also prematurely destroy erythrocytes resulting in anemia • CM’s are characterized by a set of 5 specific symptoms otherwise known as a pentad o Extreme thrombocytopenia o Intravascular hemolytic anemia o Ischemic signs and symptoms involving mainly the CNS o Kidney failure o Fever ALTERATION IN COAGULATION. • DIC-cause, S/S-DIC or disseminated intravascular coagulation is a condition in which the body clots and bleeds at the same time • Normally our coagulation and fibrinolytic systems maintain a balance • But in DIC, there is a widespread imbalance • The most common cause of DIC is a bacterial infection or sepsis o However it can also be caused by trauma, cancer, or severe hypoxia • What happens is there is an extensive amount of something called tissue factor • Tissue factor is released from cells after some kind of tissue injury (hence bacterial infections being the major cause) • Tissue factor normally activates the extrinsic pathway of the coagulation cascade • Because there is an extensive amount of it, the coagulation cascade is continuously activated • This causes small blood clots to be formed all over the body • And because the coagulation cascade is constantly being activated and clots being made, eventually the body will use up all of its platelets, clotting factors, and coagulation proteins • Now normal coagulation is affected, which causes the bleeding to occur • And because the coagulation factors are gone, bleeding cannot stop Cardiovascular Hypertension- Hypertension is increased arterial blood pressure • It is the most commonly diagnosed disease in the US • Most common in adults but starting to occur in kids • Primary hypertension is the most common type of hypertension • The specific cause is unknown • However there seems to be a combination of genetic and environmental factors that may lead to the development of HTN • Risk factors include family history, increased age, gender, black race, high sodium intake, smoking, obesity, etc. • HTN results from a sustained increase in : o Peripheral resistance (aka arterial vasoconstriction), +/or o an increase in the volume of circulating blood Pathologically, there are many mechanisms and factors that combined result in hypertension • Secondary hypertension is caused by another underlying disease process or medication that increased peripheral vascular resistance • If the cause is identified and removed before damage occurs, the HTN will resolve itself • Complicated hypertension occurs when HTN becomes chronic and more severe over time and can cause tissue damage in the heart, kidneys, brain and eyes • Malignant hypertension is a rapidly progressing hypertension • If BP is not decreased ASAP, it can lead to organ dysfunction and death • Clinical manifestations o Typically only a high blood pressure o CM of organ damage – organ specific o Death o Due to the lack of CM’s, HTN is known as the silent disease or the silent killer • In order to diagnose someone with hypertension, they have to have multiple episodes of high blood pressure not R/T other things Atherosclerosis- Atherosclerosis is characterized by hardening + thickening of the vessel wall • This is caused by a collection of lipid laden cells on the inner wall of an artery which leads to the formation of a lesion called a plaque • Atherosclerosis is not a disease, but a progressive process that can affect vessels anywhere in the body resulting in ischemia • Atherosclerosis is the leading cause of CAD and cerebrovascular diseases • Risk factors for the development of atherosclerosis include: o Smoking o HTN o DM Orthostatic Hypotension- Orthostatic hypotension is a decrease in the systolic or the diastolic blood pressure upon standing • The cause is unknown • Normally when you stand, mechanisms like the muscle pump and an increase in HR will compensate for the change in gravity • In orthostatic hypotension, there is something wrong with the body’s ability to compensate for the change in position • This causes blood to pool and the BP to drop • CM include dizziness, loss of vision, and syncope Thromboembolus- A thrombus is a blood clot that remains attached to a vessel wall. A detached thrombus is a thromboembolus. DVT ( deep venous thrombosis)- A DVT is a blood clot that obstructs the flow of blood • When we are looking at risk factors for the formation of a DVT, we use something called Virchow’s Triad, which is a group of 3 factors that promote the formation of DVT: o Venous stasis (slow blood flow in the legs) (immobility, age) o Venous endothelial damage (trauma) o Hypercoagulable states (pregnancy, malignancy, hormone replacement) • Clot formation is caused by the accumulation of platelets and clotting factors • Inflammation around the thrombus increases its growth • The inflammation may cause redness and pain which a patient may C/O • However, your patient may not always have symptoms because the clot is in a deep vein. • Sometimes the DVT has not made itself known until it has become big enough to occlude blood flow to an extremity and those S/S are what bring your patient into the hospital. PE- Pulmonary embolism is occlusion of a portion of the pulmonary vascular bed by an embolus. PE most commonly results from embolization of a clot from deep venous thrombosis involving the lower leg. A pericardial effusion- is the accumulation of fluid in the pericardial cavity, often seen along with pericarditis • Remember I said that there is normally some fluid in the pericardial cavity. In this instance, there is more than normal • The fluid can be transudative if the cause is related to heart failure or overhydration • In most instances, though, the fluid is transudative, and caused by infections, chemotherapy, or heart surgery • If the fluid develops slowly the heart can accommodate for it • However, if it occurs quickly it can compress the heart causing a serious condition called tamponade • Tamponade is so dangerous because it affects the ability of the heart to fully fill with blood • Because there is less blood and oxygen being pushed out, this will lead to a decrease in cardiac output and circulatory collapse due to a lack of blood in the system • The hallmark sign of tamponade is pulsus paradoxus Significant drop (greater than normal) in SBP during inspiration Raynaud’s Phenomenon Varicose Veins- A varicose vein is a vein in which blood has pooled, producing distended, tortuous and palpable veins • Risk factors include age, female gender, family history, obesity, pregnancy, and previous leg injury • They can be caused by trauma to a vein that damages one of the valves o When the valve is damaged that part of the vein is susceptible to larger volumes of blood pooling because of gravity • Varicose veins can also be caused from gradual venous distension in people who are on their feet a lot o Blood pools in the legs frequently due to gravity • Whatever the cause, the vein gets swollen and filled with blood, which then causes the surrounding tissues to become edematous CAD- Coronary artery disease, myocardial ischemia, acute coronary syndrome, and myocardial infarction are a continuum of disease that impair the pumping ability of the heart by depriving it of oxygen and nutrients • Atherosclerosis is the most common cause of all 4 • Diagnosis of atherosclerosis and the continuum of disease is typically done through EKG, stress tests, echocardiograms, CT scans, or cardiac angiograms • The earliest lesions are those of CAD • CAD decreases blood and oxygen supply until ischemia occurs • CAD causes 1 in 6 deaths in the United states • The risk factors for CAD are classified as major and modifiable • Major factors, which cannot be changed, include increased age, male gender, female gender after menopause, and family history • Modifiable factors, which can be changed, include dyslipidemia, HTN, smoking, DM, Obesity, Sedentary lifestyle, and an atherogenic diet which is high in cholesterol, protein, and fat • There are also some nontraditional risk factors • They are relatively new and the degree to which they affect CAD is still being explored • These include: • Presence of serum markers for inflammation • Specific levels of certain hormones • Certain infections • MI- (Myocardial Infarction) There is a multi-step pathologic process that the heart goes through with an infarction • The first step is cell injury o 10 seconds after blood flow is decreased, the muscle becomes cyanotic o After oxygen has been depleted, contractility of the heart decreases and electrolyte changes occur • The next step is cellular death o Cardiac cells can only live for 20 minutes without oxygen o If oxygen is not returned, cell death and necrosis occurs • The 3rd step is structural and functional changes of the infected tissue and the tissue surrounding the injured area • The final stage is repair of the cells in the area of the injury • CM of infarction include: o Chest pain that is more severe and prolonged than normal (unstable angina) o Pulmonary congestion – crackles o Increased HR and BP Extra heart sound Angina Pectoris (stable, Printzmetal, silent, unstable)- Myocardial ischemia is a temporary loss of blood supply and oxygen to one specific area of the heart • The most common cause of ischemia is the formation of atherosclerotic plaques • But can also be caused by anything that decreases oxygen and blood to the tissues, such as hypotension, vasospasm, or presence of a thrombus or embolus • Myocardial cells become ischemic in 10 seconds • If oxygen is not restored, infarction can occur • If blood flow is returned at the right time, the heart will start to contract again and fix any cells that were injured • People with reversible ischemia can present with different CM’s: o Stable angina pectoris ( e.g during physical exercise and one starts having chest pain then when you stop the pain goes away) ▪ Recurrent, predictable pain ▪ The vessel of the heart is starting to narrow and cannot respond to an increase in workload demand ▪ So there are people who get pain when exerting themselves o Prinzmetal angina ▪ Unpredictable and occurs at rest and with activity ▪ Most commonly occurs at night ▪ Causes by vasospasm of the vessels, with or without atherosclerosis o Silent Ischemia ▪ Totally asymptomatic ischemia ▪ More common in women Unstable angina- Chest pain that is more severe and prolonged than normal Acute Pericarditis- is acute inflammation of the pericardium • Cause is often idiopathic or due to a viral infection • The membrane becomes inflamed and rough, and sometimes a pleural effusion may develop CM include fever followed by chest pain, restlessness, anxiety, and weakness and the presence of a friction rub Constrictive Pericarditis- is associated with TB infections, radiation therapy, and rheumatoid arthritis • The pericardium becomes scarred and calcifies, causing the pericardial layers to adhere together causing a loss of the pericardial cavity • The scarring and calcification causes the heart to become encased in a hard shell • This compresses the heart, and decreases the cardiac output CM include exercise intolerance, DOE, fatigue, and anorexia Valvular Stenosis – In valvular stenosis, the valve orifice or opening is constricted and narrowed so blood cannot flow forward as easy as it should and the workload of the heart increases • Pressure rises in the specific chamber that the blood is coming from • So that chamber works harder to combat the increase in resistance (or afterload) and results in hypertrophy of the chamber • Typically, the left heart valves are affected more than the right • The most common cause of valvular dysfunction is related to rheumatic heart disease • Diagnosis of valvular dysfunctions needs to be done via echocardiogram • Regurgitation (aortic, mitral)- In valvular regurgitation, the valve fails to close completely, allowing blood to flow back into the previous chamber • This increases the amount of blood that the heart has to pump, thus increasing the workload of the heart and causing hypertrophy of the specific affected chamber • Causes of regurgitation include Rheumatic heart disease, Congenital abnormalities, HTN, infection, or trauma • In aortic regurgitation there is excess blood in the left ventricle, leading to overload and hypertrophy • CM include widening pulse pressures, a murmur, and bounding pulses • Mitral regurgitation is a backup of blood in the left atrium • This can be well tolerated for years • However, as the left atrium continues to be deformed, eventually the left ventricle will be affected and that is when the CM appear • CM are caused by left sided heart failure Tricuspid Regurgitation- Tricuspid regurgitation is a disorder in which the heart's tricuspid valve does not close properly, causing blood to flow backward (leak) into the right upper heart chamber (atrium) when the right lower heart chamber (ventricle) contracts Rheumatic Heart Disease- Rheumatic fever is a systemic inflammatory disease caused by a delayed exaggerated immune response to infection by the group A beta hemolytic streptococcus • It is a febrile illness characterized by inflammation of different parts of the body including joints, skin, and the heart • If it is left untreated, it can cause scarring and deformity of cardiac structures (valves) resulting in rheumatic heart disease • Infections are mainly found in children • Common CM are fever, lymphadenopathy, N/V, epistaxis, abdominal pain and tachycardia Left Heart Failure- Heart failure is when the heart is unable to generate an adequate cardiac output leading to: o Inadequate perfusion of blood and oxygen to the tissues o Increase in the filling pressures of the heart Left heart failure is commonly called Congestive heart failure o Pathophysiologically this is what happens: o It starts with decreased contractility of the heart, usually from an MI o This causes the heart to work harder and the myocardium to become dilated (dilated CMP) o As contractility decreases, preload increases o The heart can’t pump all the blood out effectively, so more remains in the heart, resulting in an increase in preload o Afterload also increases because there is more resistance that the heart has to push against to fully empty o In addition to the heart itself, there are other processes that play a role in the development of heart failure, including: o Immune and inflammatory processes o Dysfunction of the SNS and RAAS (like with HTN) o A vicious cycle of decreased contractility, increased preload, and increased afterload occurs leading to a steady decline of cardiac function, the presence of the CM’s, and eventually death o Manifestations of Left sided heart failure are the result of pulmonary vascular congestion (blood backs up in the lungs) and inadequate perfusion of the systemic circulation o Dyspnea, orthopnea, cough, frothy sputum, fatigue, edema, pulmonary edema with crackles, hyper or hypotension, heart murmurs o There is also usually evidence of underlying CAD, HTN, or other valvular disease o o Right Heart Failure- (Cor Pulmonale) Right heart failure is an inability of the right ventricle to provide adequate blood flow into the pulmonary circulation at a normal pressure • This is most commonly caused by diffuse hypoxic pulmonary disease such as seen with COPD or ARDS • It can also result from left sided heart failure • Also known as cor pulmonale from the pulmonary chapter QRS Complex (Electroconductivity of the heart)- The QRS complex represents the sum of all ventricular muscle cell depolarization. May vary between individuals. The duration is normally between 0.06 and 0.10 second. During the ST interval, the entire ventricular myocardium is depolarized. The QT interval is sometimes called the “electrical systole” of the ventricles. It lasts about 0.4 second but varies inversely with the heart rate. The T wave represents ventricular repolarization. Renal Pre, Intra, and Postrenal Acute Kidney Injury- acute kidney injury, in which there is a sudden decline in kidney function and a decrease in the GFR and accumulation of waste products in the blood • Common causes include: • A loss of extracellular fluid either by hemorrhage or dehydration • Decreased renal blood flow • Injury to the cells of the kidney • Acute kidney injury is classified in 3 ways • The first is Prerenal injury – Most common cause of AKI • And it is caused by renal hypoperfusion, or a lack of blood flow to the kidney • This can be caused by renal vasoconstriction, hypotension, hypovolemia, hemorrhage, or inadequate C.O. • Hypoperfusion results in a decrease in the GFR • The second classification is intrarenal injury • This usually results from Acute Tubular Necrosis, which caused destruction of the tubules of the glomerulus • ATN is caused by prerenal AKI, toxins to the kidney, DIC, infections, tumors, or renal ischemia • Postrenal injury is the third classification of AKI • It is considered rare, and is associated with urinary tract obstructions that eventually affect the kidneys • Manifestations: • Oliguria (low urine output) can occur in all 3 types of AKI, and can last from hours to weeks • Other CM depend on the initial cause of the AKI Nephrotic Syndrome- is the excretion of large amounts of protein in the urine per day • This is caused by glomerulonephritis most commonly (because the glomeruli are injured or destroyed) • Can also be seen with some systemic disease like DM, SLE, drugs, infections or cancers • CM are related to the loss of serum proteins and the associated sodium retention: o Edema o Hypoalbuminemia (low albumin- a major protein in the body) o Vitamin D deficiency (due to loss of activation by the kidney) Acute Glomerulonephritis- Acute GN is defined as the sudden onset of hematuria, proteinuria, and red blood cell (RBC) casts in the urine. This clinical picture is often accompanied by hypertension, edema, azotemia (ie, decreased glomerular filtration rate [GFR]), and renal salt and water retention Chronic Glomerulonephritis- is a kidney disorder caused by slow, cumulative damage and scarring of the tiny blood filters in the kidneys. These filters, known as glomeruli, remove waste products from the blood. In chronic glomerulonephritis, scarring of the glomeruli impedes the filtering process, trapping waste products in the blood while allowing red blood cells or proteins to escape into the urine, eventually producing the characteristic signs of high blood pressure and swelling in the legs and ankles Chronic Kidney Disease- Chronic Kidney Disease is a progressive and irreversible loss of renal function that eventually affects all the systems of the body • CKD is commonly associated with HTN, DM, and intrinsic kidney diseases, which are some of the ones we have already talked about: chronic pyelonephritis, chronic glomerulonephritis • There are 5 stages of kidney disease that start with normal functioning GFR, to end stage kidney disease • With normal functioning, the kidneys filter greater than 90ml of blood per minute • By the time the kidneys have reached end stage, they are filtering less than 15ml/minute • Whatever the cause of CKD, the end result is the destruction of the functional units of the kidney or the nephrons • The kidney will attempt to adapt and compensate for the loss, up until there is over 75% of functioning loss • Progression of CKD is associated with the following pathogenic processes: o Glomerular HTN, hyperfiltration, and hypertrophy o This leads to proteinuria o The glomerular HTN is caused by an increase in the production of Angiotensin II which causes vasocontriction o Glomerulosclerosis o Tubule inflammation and fibrosis Chronic Kidney Disease or Chronic Renal Failure-labs, diagnostics- For kidney disease diagnosis, you may also need certain tests and procedures, such as: • Blood tests. Kidney function tests look for the level of waste products, such as creatinine and urea, in your blood. • Urine tests. Analyzing a sample of your urine may reveal abnormalities that point to chronic kidney failure and help identify the cause of chronic kidney disease. • Imaging tests. Your doctor may use ultrasound to assess your kidneys' structure and size. Other imaging tests may be used in some cases. • Removing a sample of kidney tissue for testing. Your doctor may recommend a kidney biopsy to remove a sample of kidney tissue. Kidney biopsy is often done with local anesthesia using a long, thin needle that's inserted through your skin and into your kidney. The biopsy sample is sent to a lab for testing to help determine what's causing your kidney problem. Creatinine and BUN levels- Creatinine is a chemical waste molecule that is generated from muscle metabolism. Creatinine is produced from creatine, a molecule of major importance for energy production in muscles. Approximately 2% of the body's creatine is converted to creatinine every day. Creatinine is transported through the bloodstream to the kidneys. The kidneys filter out most of the creatinine and dispose of it in the urine. The creatinine levels in both urine and blood are determined and compared. Normal creatinine clearance for healthy women is 88-128 mL/min. and 97 to 137 mL/min. in males (normal levels may vary slightly between labs). Blood urea nitrogen (BUN) level is another indicator of kidney function. Acute Cystitis- is inflammation of the bladder and is the most common site of a UTI • The most common bacteria that causes cystitis is E.Coli • The infection of the bladder causes an inflammatory response • The edema from the inflammatory response affects the stretch receptors in the bladder • This causes symptoms of fullness when the bladder is only filled with small volumes, thus producing the CM of a UTI • CM: Some may be asymptomatic o Frequency o Dysuria (painful urination) o Urgency o Lower abdominal or suprapubic pain Interstitial cystitis- also known as painful bladder syndrome is a condition, in which an individual has symptoms of cystitis, but the cultures are negative and there is no other known cause • It is very common in women in their 20-30’s • Possible causes: o Non-bacterial infections like a parasite, a virus, or a fungus o Hypersensitivity reaction o Altered Immune response or someone who is Immunosuppressed o The bladder gets inflamed, but the reason for it is unknown • There are thoughts that it may be due to an autoimmune response • CM include: o Frequency, chronic pelvic pain, small volume of urine, cloudy urine and hematuria o (ones that would be seen with acute cystitis) Urinary Tract Obstruction- A urinary tract obstruction is anything that affects the flow of urine, anywhere along the urinary tract • The obstruction can be related to an anatomical problem or a functional problem • An obstruction will: • Stop the flow of urine proximal to the blockage • This will lead to dilation of the urinary structures which is an early response • This will increase the patients risk of infection • Eventually the overall functioning of the kidneys will be affected • Specifically, the kidneys ability to maintain F+E levels and excrete waste products • An obstructive uropathy is an anatomical change of the urinary system caused by the obstruction • The severity of the uropathy depends on many things: • The location of the obstruction • The involvement of one or both of the urinary tracts • How complete the obstruction is, or how much of it was obstructed • How long the obstruction was there • What caused the obstruction • 3 examples of obstructive uropathies in the upper urinary tract include: • Hydroureter – dilation of the ureter, causing accumulation of urine in the ureter • Hydronephrosis – dilation of the renal pelvis or calyces • Ureterohydronephrosis – Dilation of the ureter and the renal pelvis and/or calyces • Eventually relieving the obstruction will allow the kidney to regain some of the lost function, but not all Urinary Tract Infection- A UTI is inflammation of the urinary epithelium caused by bacteria from the gut (normal gut flora) • A UTI can occur anywhere along the urinary tract, from the urethra up to the kidney • The following people are at highest risk for a UTI: • Newborns and children and elderly • Pregnant and sexually active women • People with indwelling catheters • Diabetes • Urinary tract obstructions • They are most common in women because their urethra is shorter, and anatomically the urethral opening is very close to the anus Renal Calculi- A kidney stone or renal calculi is one of the most common causes of an upper urinary tract obstruction • They are masses of substances (protein, crystal, or something else) that form within the urinary tract and obstruct the flow of urine • Kidney stones can form anywhere, including the kidneys, ureter and the bladder • There are many things that put people at risk for kidney stones, including o Gender –more common in men o Race o Fluid intake, or lack of o Urinary retention – creates a good environment for kidney stone formation o Specific diet o Activity levels o Changes in urine pH • Kidney stones are classified by the specific material that it is made of: o Calcium – which is the most common type o Struvite – made of magnesium, ammonium, and phosphate o Uric Acid o Pathophysiologically, the formation of kidney stones is related to 4 things: o Super-saturation of 1 or more salts in the urine • Higher level of salts than normal than the body is able to dissolve like normal o Precipitation of the salts from a liquid to a solid state o Growth of the stone through crystallization o The presence or absence of stone inhibitors • Proteins or naturally occurring substances that prevent the formation of stones • CM: o The major CM is Renal colic which is moderate to severe pain that starts in the flank and radiates to the groin o Urgency o Frequency o Urge Incontinence o Hematuria Gastrointestinal Functions of GI System- The digestive system is responsible for taking whole foods and turning them into energy and nutrients to allow the body to function, grow, and repair itself. The six primary processes of the digestive system include: 1. Ingestion of food 2. Secretion of fluids and digestive enzymes 3. Mixing and movement of food and wastes through the body 4. Digestion of food into smaller pieces 5. Absorption of nutrients 6. Excretion of wastes Peristalsis- is a series of wave-like muscle contractions that moves food to different processing stations in the digestive tract. The process of peristalsis begins in the esophagus when a bolus of food is swallowed. Functions of GI organs (liver, pancreas, stomach, large intestine, small intestine, gall bladder)- The digestive system includes the gastrointestinal tract and accessory organs of digestion: the salivary glands, liver, gallbladder, and exocrine pancreas. The digestive system breaks down ingested food, prepares it for uptake by the body's cells, absorbs fluid, and eliminates wastes. Food breakdown begins in the mouth with chewing and continues in the stomach, where food is churned and mixed with acid, mucus, enzymes, and other secretions. From the stomach, the fluid and partially digested food pass into the small intestine, where biochemical agents and enzymes secreted by the intestinal cells, liver, gallbladder, and exocrine pancreas break it down into absorbable components of proteins, carbohydrates, and fats. These nutrients pass through the walls of the small intestine into blood vessels and lymphatics that carry them to the liver for storage or further processing. Ingested substances and secretions that are not absorbed in the small intestine pass into the large intestine, where fluid continues to be absorbed. Fluid wastes travel to the kidneys and are eliminated in the urine. Solid wastes pass into the rectum and are eliminated from the body through the anus GI Cancers-Gastric, Esophageal, Colorectal, Stomach, Liver-risk factors and causes General GI clinical manifestations-anorexia, nausea, vomiting, retching, abdominal pain, diarrhea, constipation, etc.- Anorexia is a lack of a desire to eat despite the normal physiologic stimuli that normally tells you that you are hungry • It is often associated with other CM’s or side effects of drugs or diseases Nausea is a subjective experience that is associated with many diseases and conditions • The common symptoms are hypersalivation and tachycardia Retching is nonproductive vomiting Vomiting is the forceful emptying of the stomach through the mouth • There are many causes that will initiate the vomiting reflex, such as: o Severe pain o Stomach distension o Trauma o Drugs o Neurologic conditions o Motion o Flu • Consequences of vomiting are fluid/electrolyte and acid/base imbalances Constipation is an infrequent or difficult defecation • It can be categorized as primary or secondary • Primary has 3 types: • There are different subtypes of primary, but it is mainly caused by either a problem with: • Colon activity • Weak pelvic floor muscles • Secondary constipation can be caused by: • Neurogenic disorders – MS, spinal cord lesions. Neuropathways to the colon are altered • Low residue diet, sedentary lifestyle, meds, IBS, pregnancy, aging • CM of constipation include straining with defecation, hard stool, sensation of incomplete emptying, frequent manual maneuvers to remove stool, less than 3 BM’s per week Diarrhea is an increase in the frequency of BM’s • Characterized by stool with increased volume and fluid content • There are 3 major mechanism of diarrhea: • Osmotic diarrhea • Presence of a non-absorbable substance in the intestine causes water to be drawn in to the colon, increasing stool weight and volume, and causing large volume diarrhea. • This is seen with e.g lactose intolerance or with patients on tube feeds • Secretory diarrhea • Large volume diarrhea caused by excessive mucosal secretions in the intestines • Often seen with e.g bacterial infections • Motility diarrhea • Digestion and absorption are impaired • Can be caused by resection of the intestines or a fistula (abnormal passageway) • CM include dehydration, electrolyte imbalance, and weight loss Abdominal pain is a symptom of many GI disorders, and is most commonly the presenting symptom • There are 3 categories of abdominal pain • Parietal pain • Comes from the peritoneum or abdominal wall • Localized and intense • Visceral pain • From the abdominal organs themselves • Pain is diffuse and vague • Referred pain • Visceral pain felt at some distance from the disease or affected organ • It has radiated to another area Types of bleeding-Upper vs. Lower, vocabulary for bleeding- Gastrointestinal bleeding can be subcategorized as upper versus lower • Upper GI o Bleeding in esophagus (from bleeding veins), stomach (from ulcers) or duodenum o Frank, bright, red blood or o Dark grainy digested blood (coffee ground) that is affected by stomach acid • Lower GI o Bleeding from the jejunum, ileum, colon, or rectum o Polyps, diverticulitis, inflammatory disease, cancer, hemorrhoids • The physiologic response depends on the amount and rate of the blood loss • The best indicator for massive blood loss is a change in BP and HR • Other GI bleeding definitions: o Hematemesis – presence of blood in vomit o Hematochezia – fresh, bright red blood from the rectum o Melena – dark, tarry stool due to the digestion of food o Occult bleeding – is slow chronic blood loss that is not obvious, appears normal, can be detected only with positive fecal occult blood test (guaiac test) GERD/Reflux esophagitis, esophageal cancer risk- GERD is the regurgitation or reflux of chyme within 1-2 hours after eating • Patho: • Normally the pressures in the esophagus are high to keep the LES (lower esophageal sphincter) closed and prevent reflux • With GERD, the pressures are lower affecting the LES • In other words, the LES does not stay closed so the reflux of food and acid is allowed to happen • The other component of GERD is delayed gastric emptying • This increases the amount of gastric content and the amount of time in which reflux can occur • The severity of the GERD depends on the acidity of the contents that were refluxed and how long those contents are in the esophagus • Causes of GERD include: • A weak lower esophageal sphincter • Weak esophageal peristalsis • An increase in abdominal pressure from obesity or pregnancy • Hernia’s (which can weaken the LES) • Gastric ulcers (delay gastric emptying) • CM: heartburn, cough, Upper abdominal pain 1 hour after eating Hernias-hiatal, inguinal, etc., complications- Hiatal hernia is a protrusion or herniation of the upper stomach through the diaphragm • There are 2 main types o Sliding ▪ Most common ▪ Stomach moves into the thoracic cavity through the esophageal hiatus which is the hole in the diaphragm through which the esophagus passes o Paraesophageal ▪ The greater curvature of the stomach herniates through a secondary opening in the diaphragm ▪ It often sits right next to the esophagus ▪ Strangulation is a serious complication of this type • Causes of hernia’s are: o A short esophagus o Trauma o weak diaphragm muscles o Increased abdominal pressure • Manifestations o May be asymptomatic for years o Reflux o Dysphagia o Epigastric pain Pyloric Obstruction- Pyloric obstruction (also known as gastric outlet obstruction) is a blocking or narrowing of the opening between the stomach and the duodenum • It can be acquired from other diseases like peptic ulcer disease or gastric cancer or it can be a congenital problem o Ulceration causes obstruction from inflammation, edema, spasm, fibrosis, or scarring o Tumors cause obstruction by growing into the pylorus • The early sign of this is epigastric pain and fullness • Other signs are nausea and a succession splash which is when the abdomen produces a sloshing sound with movement • Vomiting is a later sign Small Bowel Obstruction-s/s, causes- (SBO) is caused by postoperative adhesions, tumors, Crohn disease, and hernias. SBO leads to distention caused by impaired absorption and increased secretion with accumulation of fluid and gas inside the lumen proximal to the obstruction. Distention decreases the intestine's ability to absorb water and electrolytes and increases the net secretion of these substances into the lumen. Copious vomiting or sequestration of fluids in the intestinal lumen prevents their reabsorption and produces severe fluid and electrolyte disturbances. Extracellular fluid volume and plasma volume decrease, causing dehydration, increased hematocrit level, hypotension, and tachycardia. Peptic Ulcer Disease- Peptic ulcer disease is a break or ulceration in the protective mucosal lining of the lower esophagus, stomach, or duodenum • The 3 major causes of peptic ulcers are: o H Pylori – causes 90% of all ulcers o Use of NSAIDS o Zollinger Ellison Syndrome – a syndrome characterized by an increased production of gastrin (a hormone that controls the release of gastric acid) • There are 2 major forms: o Duodenal ▪ Most common ▪ Affects the upper part of the small intestine ▪ Typically due to increased acid secretion or bacteria causing inflammation that erodes the wall ▪ Characteristic CM is pain when the abdomen is empty(exam) o Gastric ▪ Affects the stomach lining (mucosa) ▪ Gastric secretion is normal ▪ But mucosal barrier is damaged and becomes edematous ▪ Small vessels in the stomach are usually destroyed causing bleeding ▪ Characteristic CM is pain after eating instead of when empty(exam) There is also more N/V and weight loss as well Gastric vs. Duodenal Ulcers-see table in your book- Characteristics Gastric Ulcer Duodenal Ulcer Incidence Age at onset 50-70 years 20-50 years Family history Usually negative Positive Gender (prevalence) Equal in women and men Greater in men Stress factors Increased Average Ulcerogenic drugs Normal use Increased use Cancer risk Increased Not increased Pathophysiology Abnormal mucus May be present May be present Parietal cell mass Normal or decreased Increased Acid production Normal or decreased Increased Serum gastrin Increased Normal Serum pepsinogen Normal Increased Characteristics Gastric Ulcer Duodenal Ulcer Associated gastritis Helicobacter pylori More common Usually not present May be present (60-80%) Often present (95-100%) Stimulates reduced acid secretion, gastric atrophy, and risk of gastric cancer Clinical Manifestations Stimulates acid hypersecretion Pain Located in upper abdomen Located in upper abdomen Intermittent Intermittent Pain-antacid-relief pattern Pain-antacid/food-relief pattern Food-pain pattern (when food in stomach) Pain when stomach empty Nocturnal pain common Clinical course Chronic ulcer without pattern of remission and exacerbation Heals more slowly Pattern of remissions and exacerbation for years Heals more quickly Gastritis- Gastritis is an inflammatory disorder of the gastric mucosa • It is classified as acute versus chronic • Acute gastritis o Erodes the surface epithelium of the stomach o Usually caused by injury to the protective mucosal barrier by drugs like NSAID’s o CM include vague abdominal discomfort, epigastric tenderness, and bleeding o Chronic gastritis causes thinning and atrophy of the gastric mucosa • Chronic gastritis is classified by the location of the gastritis • There are 2 types: o Chronic fundal gastritis (top of stomach): ▪ The gastric mucosa (lining of stomach) degenerates in the fundus of the stomach leading to gastric atrophy ▪ It is thought to be due to an autoimmune cause ▪ This type of gastritis also puts people at a high risk for the development of gastric cancer o Chronic antral gastritis (bottom of stomach): ▪ Most common ▪ H Pylori seems to be a major factor that is associated with the inflammation found in this type ▪ Also caused by alcohol, tobacco, and NSAID’s ▪ CM of chronic gastritis include vague GI symptoms such as nausea, vomiting, anorexia, pain, and gastric bleeding Lactose Intolerant-s/s, patho- Lactose deficiency or intolerance is the inability to break down lactose into monosaccharide • Thus leading to an inability to digest and absorb monosaccharides • This is most common in African American’s, Latino’s, and native Americans • It also usually does not develop until adulthood • Undigested lactose remains in the intestine where it becomes fermented by bacteria • Leading to bloating, gas, cramping pain, and osmotic diarrhea Bile Salt Deficiency & Fat Soluble Vitamins- A bile salt deficiency is a lack of bile salts that are necessary for fat digestion and absorption • It can be caused by o Advanced liver disease – decreased bile salt production o Obstruction of the common bile duct o Intestinal stasis • CM are related to poor absorption of fat and fat soluble vitamins o Fatty stools o Diarrhea • Because fat soluble vitamins are also not absorbed correctly, other manifestations will be related to the vitamin that is lost (Fat Soluble Vitamins are) o Vitamin A deficiency will cause night blindness o Vitamin D deficiency will cause bone problems o Decreased calcium absorption, Osteoporosis, fractures o Vitamin K deficiency will cause bleeding problems o Vitamin E deficiencies are unknown Inflammatory Bowel Disease- Inflammatory bowel diseases are chronic, relapsing disorders of the colon of unknown origin that cause ulceration of the colon mucosa • There are 2 main types of IBD: • Ulcerative Colitis: o The cause of UC seems to be genetic, related to an abnormal immune response in the GI tract o It is characterized by periods of exacerbation and remission o Often the exacerbations are stress related. o Pathophysiology: o The disease begins in the rectum and may affect the whole colon o Inflammation occurs and causes edema o Multiple abscesses form leading to ulceration formation o These ulcers bleed and cause increased peristalsis and diarrhea o As the disease progresses, the bowel mucosa thickens and shortens, decreasing the surface area of the colon that is available for absorption of nutrients. o Clinical manifestations o Blood diarrhea o Cramp-like abdominal pain o Fever, malaise, anorexia, weight loss Crohn’s Disease: Cause is unknown, may be a familial tendency/genetic or related to an altered immune response like in UC o It is often hard to differentiate UC from Crohn, but the biggest difference is the location of the inflammation – Crohns does not affect the rectum o Pathophysiology: o this is a recurring inflammation of the small and large intestine o May progress to ulceration of the intestine, and shortening and thickening of the mucosal wall o CM: o Non-bloody diarrhea o Steatorrhea o Crampy abdominal pain o Weight loss o Malnutrition o Diverticulosis/diverticulitis- Diverticula are herniations or sac like outpoutchings of the mucosa through the muscle layers of the colon • Very common in the sigmoid colon • Diverticulosis is asymptomatic disease • Diverticulitis is the inflammatory disease • The exact cause is unknown, but may be due to increased pressure at weaker points of the colon wall, often where arteries enter into the colon • In diverticulitis, retained undigested food and bacteria accumulate in the diverticula • That area becomes inflamed, and may lead to perforation, abscess, peritonitis, obstruction, or hemorrhage • CM: o Mild to severe abdominal pain o Fever, chills, diarrhea, constipation Appendicitis, s/s, causes- Appendicitis is an inflammation of the appendix • The possible causes are related to obstruction, ischemia, increased intraluminal pressure, infection, or ulceration • The biggest theory for appendicitis to occur is due to an obstruction with consequential bacterial infection • The typical symptoms are epigastric and right lower quadrant pain • The pain may be rebound tenderness, meaning that the pain starts after pressure has been removed from the abdomen, not when pressing on the abdomen • Nausea, vomiting, and anorexia can also occur • The most serious complication is peritonitis: An inflammation of the peritoneum Pancreatitis-remember NPO! causes, patho- Pancreatitis is inflammation of the pancreas • It can be acute or chronic • Acute pancreatitis o Usually mild and resolves itself spontaneously o Develops due to an obstruction in the pancreatic or bile duct, affecting the outflow of pancreatic enzymes (i.e. gallstones) o The enzymes will collect in the pancreas, become activated and destroy the cells of the pancreas through auto-digestion resulting in inflammation and acute pancreatitis o If the cause of acute pancreatitis is due to alcoholism, the ethanol is metabolized by the pancreas causing damage to the cells o This damage will also cause the enzymes to be activated leading to auto- digestion, and pancreatitis o CM: ▪ Epigastric or mid abdominal pain (cardinal sign) ▪ Pain is constant and will range from mild discomfort to severe incapacitating pain ▪ Nausea and vomiting ▪ Jaundice Chronic pancreatitis o Inflammation leading to irreversible structural and functional impairment of the pancreas o Most common cause is alcohol abuse o The pancreatic duct will become obstructed and it will calcify causing fibrosis and atrophy of the pancreas o Abscesses or cysts can also develop ▪ The cysts contain pancreatic juice, necrotic debris, and blood o CM include intermittent abdominal pain and weight loss o These patients can also have signs of malabsoption syndrome Cause of Obesity-leptin resistance- Obesity is an increase in body fat mass with a BMI greater than 30 • It has become a worldwide problem that is becoming more common in children as well • Causes and consequences are multiple and complex • It is a major cause of morbidity, mortality, and increased health care costs • It is said to be caused by a combination of genetics and environmental factors (food, culture, physical activity, etc.) • You have many hormones that serve as peripheral signals to tell the hypothalamus to regulate appetite and metabolism • In obesity, these hormone levels are altered, thus affecting how the hypothalamus regulates or does not regulate appetite and food metabolism • There are multiple hormones that are increased in an obese individual • The most specific hormone is Leptin • Leptin resistance promotes over-eating, weight gain, and insulin resistance • CM of obesity: o Begins as visceral obesity: ▪ Distribution of fat around the abdomen and upper body o Peripheral obesity ▪ Distribution around the thighs and buttocks More common in females • Anorexia nervosa, Bulimia nervosa, starvation, malnutrition- Anorexia nervosa is a condition in which a person has a poor body image disorder who refuses to eat • Anorexic patients can lose 25-30% of their body weight as a result of fat and muscle depletion, which can affect many organs and eventually lead to death • Anorexia is often also associated with other disorders such as anxiety, depression, and OCD • Anorexia is characterized by: o Fear of becoming obese despite weight loss o Distorted body image o Body weight less than 15% of optimal o In females – the absence of 3 consecutive menstrual periods o Skeleton like appearance • In bulimia nervosa, body weight remains near normal, but they have a desire that they need or want to lose weight • Bulimia is characterized by: o Recurrent episodes of binge eating o Self-induced vomiting or frequent laxative use o Two binge eating episodes per week for at least 3 months o Fasting to negate the effect of binge eating o Or they excessively exercise • The continued vomiting of acidic chyme can cause: o Pitted teeth o Pharyngeal and esophageal inflammation • The overuse of laxatives can lead to rectal bleeding Malnutrition is a lack of nourishment from inadequate amounts of calories, vitamins, or minerals Starvation is a state of extreme malnutrition and hunger from the lack of nutrients • Sometimes short term starvation is used for weight loss plans • Long term starvation can lead to eventual death o The body is breaking down all body stores for energy, eventually causing breakdown of proteins and muscles Hepatitis-types (A, B, C, D, E), route of transmission, phases- Viral hepatitis is a systemic inflammatory viral disease that primarily affects the liver • Different strains cause different forms of hepatitis and are transmitted in different ways: • Hepatitis A • Transmitted through fecal oral route • Found in crowded and unsanitary conditions • Hepatitis B • Transmitted through contact with infected blood and body fluids or contaminated needles • Hepatitis C • Transmitted through blood transfusion or IV drug use • Hepatitis D and E are also fecal oral route • The pathologic lesions of hepatitis will cause: • Necrosis of the hepatic cells • Scarring of the liver • Hyperplasia of the Kuppfer cells (immune cells of the liver) • Damage to the bile tract causing obstructive jaundice • The regeneration of hepatic cells occurs within 48 hours of the initial injury • The clinical course of hepatitis is broken down into 3 phases: o Prodromal phase ▪ Starts 2 weeks after the infection exposure, and goes until jaundice appears ▪ Fatigue, anorexia, nausea, vomiting, headache and low grade temp are common ▪ The hepatitis infection is highly infectious to others at this stage o Icteric phase ▪ Takes place 1 to 2 weeks after the prodromal stage ▪ Symptoms include jaundice, dark urine, and an enlarged and painful, palpable liver o Recovery phase ▪ Begins with the resolution of the jaundice ▪ However the liver will remain enlarged and tender for weeks Types of Jaundice-Obstructive, Hemolytic-causes- Jaundice is a yellow or green discoloration of the skin • There are 2 types of jaundice: o Obstructive jaundice – most common ▪ Caused by an occlusion in the bile duct, stopping the flow of bile from the liver o Hemolytic Jaundice ▪ Caused by excessive RBC destruction • CM: Yellow discoloration in the eye and the skin o Pruritus – due to bilirubin accumulation in the skin o Fever/Chills/Pain Cirrhosis- Cirrhosis is an irreversible, inflammatory liver disease characterized by inflammation of the liver and structural changes of fibrosis and scar tissue growth in the liver • Similar to hepatitis in that it is inflammation of the liver, however cirrhosis is not reversible • It is the leading cause of death in the United States • Cirrhosis may be caused by alcohol, Hepatitis infection, or it is also idiopathic Portal Hypertension/Esophageal varices/Upper GI bleed- Portal hypertension is abnormally high blood pressure in the hepatic portal venous system • This is caused by any disorder that obstructs or impede’ s blood flow: o Cirrhosis (most common) o Viral hepatitis o Varices are distended, tortuous veins from prolonged high pressures in the portal system o Blood backs up causing these varices o Common in the esophagus, stomach, and rectum o Have a high risk of rupturing and causing life-threatening GI bleeds o Splenomegaly or enlargement of the spleen o Due to increased pressure in the splenic veins Ascites-what is it, cause?- Ascites which are an accumulation of fluid in the peritoneal cavity o It is caused by portal hypertension and a decrease in the creation of Albumin by the liver The combination of portal hypertension and the loss of albumin causes an increase in capillary hydrostatic pressure and thus edema Cholecystitis/Cholelithiasis- Obstruction and inflammation of the gall bladder are the two most common problems of the gall bladder • Cholelithiasis are gallstones • There are 2 main types of gall stones o Cholesterol ▪ Most common ▪ Form in bile when it is supersaturated with cholesterol, leading to cholesterol crystal formation o Pigmented ▪ Form from increased levels of bilirubin in bile • The exact cause of gallstones is unknown • Stones can lie dormant in the gall bladder, or they can become lodged and cause pain • CM: patient may be asymptomatic o However abdominal pain and jaundice are cardinal signs that someone has gall stones • Cholecystitis is inflammation of the gall bladder and is typically caused by a gall stone that has lodged in one of the ducts • CM include severe pain [Show More]
Last updated: 2 years ago
Preview 1 out of 41 pages
Buy this document to get the full access instantly
Instant Download Access after purchase
Buy NowInstant download
We Accept:

Reviews( 0 )
$14.50
Can't find what you want? Try our AI powered Search
Document information
Connected school, study & course
About the document
Uploaded On
Dec 13, 2022
Number of pages
41
Written in

Additional information
This document has been written for:
Uploaded
Dec 13, 2022
Downloads
0
Views
232





.png)

.png)
