NURS 342 Sepsis Shock Case Study (2)
Sepsis Shock Case Study part 2
History of Current Problem:
Jack Holmes a 72-year-old Caucasian male brought to the ED by ambulance from a skilled nursing facility (SNF). Accordin
...
NURS 342 Sepsis Shock Case Study (2)
Sepsis Shock Case Study part 2
History of Current Problem:
Jack Holmes a 72-year-old Caucasian male brought to the ED by ambulance from a skilled nursing facility (SNF). According to report from the paramedic, when the SNF nursing staff attempted to wake him this morning, he would not respond, and his BP was 74/40 with a MAP of 51. He has a history of Parkinson’s disease, COPD, CHF, HTN, depression, and a stage IV decubitus ulcer on his coccyx that developed three months ago. He does not follow commands, is unresponsive to verbal stimuli, but responds to a sternal rub with grimacing and withdrawing from stimulus.
Personal/Social History:
He has lived in the skilled nursing facility the past three years and has been bed bound the past year due to his advanced Parkinson’s disease. He was a heavy smoker, 1 PPD for 40 years until he moved to the SNF.
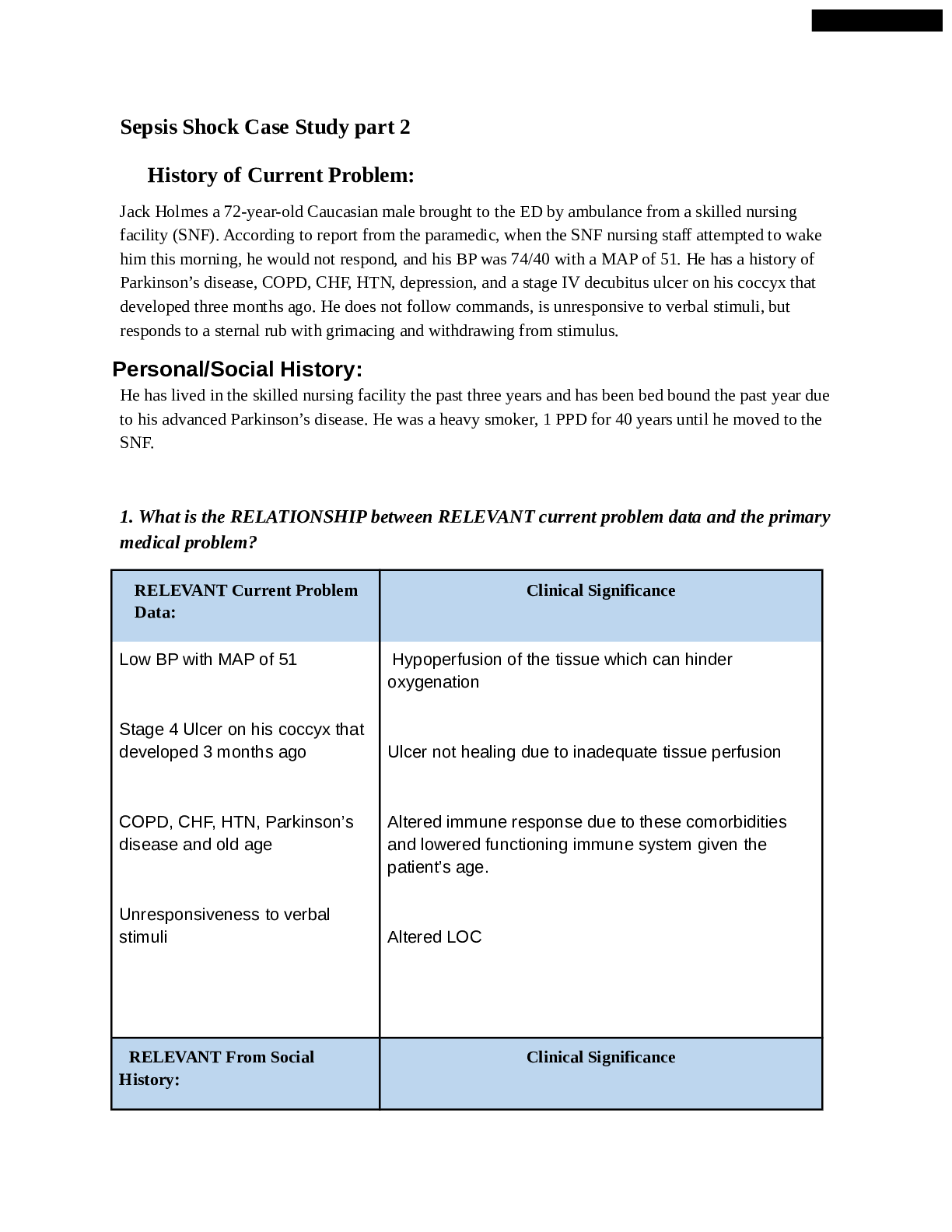
1. What is the RELATIONSHIP between RELEVANT current problem data and the primary medical problem?
RELEVANT Current Problem Data: Clinical Significance
Low BP with MAP of 51
Stage 4 Ulcer on his coccyx that developed 3 months ago
COPD, CHF, HTN, Parkinson’s disease and old age
Unresponsiveness to verbal stimuli
Hypoperfusion of the tissue which can hinder oxygenation
Ulcer not healing due to inadequate tissue perfusion
Altered immune response due to these comorbidities and lowered functioning immune system given the patient’s age.
Altered LOC
RELEVANT From Social History: Clinical Significance
Skilled Nursing Facility
Bed bound due to his parkinson’s
Depression More exposure to pathogens or iatrogenic illness at the facility
Poor skin integrity, atrophy of muscle, renal calculi, DVT, isolation
Isolation, no interest or motivation in performing ADLs, unable to self advocate, withdrawing from peers
Patient Care Begins
Current VS P-Q-R_S-T Pain Assessment
T: 103.4 F/39.7 C (oral) Provoking /palliative Not responsive verbally, withdraws to pain, no other indicators of pain
P: 135 (irregular) Quality
R: 32 (regular) Region/radiation
BP: 76/39 MAP: 51 Severity
O2 Sat: 91% 2 liters n/c Timing
2. What VS data are RELEVANT and must be interpreted as clinically significant by the nurse?
RELEVANT VS Data Clinical Significance
Temperature is high
Respiration is high
BP is low
O2 Sat is low (91%)
There is an active infection in the body, this can also cause higher metabolism which can lead to fatigue
Compensating for low BP inorder to adequately oxygenate the tissues
This is an indication of septic shock
Could be normal for a patient with COPD who is a heavy former smoker with a history of 1 PPD for 40 years.
Current Assessment
General appearance Pale and warm to touch. Appears tense.
Respirations Tachypneic and working hard to breathe, intercostal and suprasternal retractions present. Breath sounds diminished and light crackles in lower lobes bilat. Nail beds have noticeable clubbing, barrel chest present.
-
-
-
-
-
-
-
-
-
-
Wound culture
This test is carried out to determine the cause of sepsis and the type of antibiotic to use
Vancomycin 2 g IV after cultures collected This is a broad spectrum antibiotic that is used to treat infection until the main cause of the infection is determined
Clindamycin 600 mg IV every 6 hours
This is an antibiotic that is used to treat patient with infection
If MAP remains <65 after 2250 mL of 0.9% NS…start Norepinephrine 1-12 mcg/min to maintain MAP >65
An elevated MAP <65 initiate kidney perfusion. Norepinephrine is a vasopressor that constrict blood vessel to keep MAP elevated.
If MAP remains <65 after norepinephrine at 1 mcg/kg/min…start
Vasopressin 0.04 units/minute to maintain MAP >65 Vasopressin is considered an antidiuretic which can lead to the prevention of fluid loss leading to an increase fluid in vessel and MAP
Continuous cardiac monitor
This detects changes in heart rhythm, rate and conduction
VS every 5-15”
This is used to determine changes within a patient with sepsis
Acetaminophen 1000 mg PR every 6 hours PRN for fever >101
This is used to reduce fever which will then reduce body’s metabolic rate
15. Identify 3 Nursing Priorities (first part of nursing diagnosis- These should be active problems)
1. Impaired Gas Exchange
2. Ineffective tissue perfusion
3. Deficient fluid volume
4. Imbalanced nutrition less than body requirements
16. What will you do to address Jack’s psychosocial / emotional needs
As Jack’s nurse it is important to ensure his family is present for support during this time and that end of life decisions can be made in the event that his condition becomes irreversible. Additionally, because Jack’s condition has caused an altered level of consciousness, in addition to the changes caused by his Parkinson’s Disease--it is important to educate the family and the patient when/if the condition improves and the patient is to heal and eventually be discharged. Given that there are potential long-term effects of septic shock and MODS, it is important to teach the patient and family members of any risks. The long-term effects may include insomnia, disabling muscle joint pains, decreased cognitive function, organ dysfunction, anxiety and/or depression, mood changes, etc. It is vital to address Jack’s emotional needs as well by having family support present but also working to develop coping skills to deal with his condition and the aftermath but also his depression from being bed ridden. This may include frequent reorientation and administration of antidepressants and anxiolytics. It is imperative to educate Jack on his condition and involve him in his plan of care, which may instill a sense of empowerment in him.
[Show More]
 - Morgan State University.png)