NUR MISC EXAM 3
CH. 36 Antihistamines, Decongestants, Antitussives, & Expectorants
Antihistamines
Drugs that directly compete with histamine for specific receptor sites
Two histamine receptors
o H1 (histamine1):
...
NUR MISC EXAM 3
CH. 36 Antihistamines, Decongestants, Antitussives, & Expectorants
Antihistamines
Drugs that directly compete with histamine for specific receptor sites
Two histamine receptors
o H1 (histamine1): smooth muscle contraction and capillaries
o H2 (histamine2): GI and HR acceleration
H1 antagonists (H1 Blockers antihistamines
o Examples: chlorpheniramine, fexofenadine (Allegra), loratadine (Claritin),
cetirizine, diphenhydramine (Benadryl)
Antihistamine Properties
o Antihistaminic
o Anticholingeric
o Sedative
H2 blockers or H2 antagonists
o Used to reduce gastric acid in peptic ulcer disease (PUD)
o Examples: cimetidine, ranitidine, famotidine, nizatidine
Antihistamines: Mechanism of Action
Block action of histamine at H1 receptor sites
Compete with histamine for binding at unoccupied receptors
Cannot push histamine off the receptor if already bound
The binding of H1 blockers to the histamine receptors prevents the adverse
consequences of histamine stimulation
o Vasodilation
o Increased gastrointestinal (GI) and respiratory secretions
o Increased capillary permeability
More effective in preventing the actions of histamine rather than reversing them
Should be given early in treatment, before all the histamine binds to the receptors
Histamine vs. Antihistamine Effects
Cardiovascular (small blood vessels)
o Histamine effects
Dilation and increased permeability (allowing substances to leak into
tissues)
o Antihistamine effects
Reduce dilation of blood vessels
Reduce increased permeability of blood vessels
Smooth muscle (on exocrine glands)
o Histamine effects
Stimulate salivary, gastric, lacrimal, and bronchial secretions
o Antihistamine effects
Reduce salivary, gastric, lacrimal, and bronchial secretions Immune system (release of substances commonly associated with allergic reactions)
o Histamine effects
Mast cells release histamine and other substances, resulting in allergic
reactions
o Antihistamine effects
Binds to histamine receptors, thus preventing histamine from causing a
response
Antihistamines: Other Effects
Skin
o Reduce capillary permeability, wheal-and-flare formation, itching
Anticholinergic
o Drying effect that reduces nasal, salivary, and lacrimal gland secretions (runny
nose, tearing, and itching eyes)
Sedative
o Some antihistamines cause drowsiness
Antihistamines: Clinical Indications
Management of:
o Nasal allergies
o Seasonal or perennial allergic rhinitis (hay fever)
o Allergic reactions
o Motion sickness
o Parkinson’s disease
o Sleep disorders
Also used to relieve symptoms associated with the common cold
o Sneezing, runny nose
o Palliative treatment, not curative
Antihistamines: Contraindications
Known drug allergy
Narrow-angle glaucoma
Cardiac disease, hypertension (HTN)
Kidney disease
Bronchial asthma, chronic obstructive pulmonary
disease (COPD)
Peptic ulcer disease (PUD)
Seizure disorders
Benign prostatic hyperplasia (BPH)
Pregnancy
Antihistamines: Adverse Effects
Anticholinergic (drying) effects, most common
o Dry mouth
o Difficulty urinating
o Constipation
o Changes in vision Drowsiness
o Mild drowsiness to deep sleep
Antihistamines: Two Types
Traditional
o Brompheniramine, chlorpheniramine,
dimenhydrinate, meclizine, and promethazine
Nonsedating
o Loratadine, cetirizine, and fexofenadine
Nonsedating: Peripherally Acting Antihistamines
Developed to eliminate unwanted adverse effects, mainly
sedation
Work peripherally to block the actions of histamine
fewer CNS adverse effects
Longer duration of action (increases compliance)
Traditional Antihistamines
Older
Work both peripherally and centrally
Have anticholinergic effects, making them more effective
than nonsedating drugs in some cases
Antihistamines: Nursing Management
Assess for allergic reactions that required treatment,
including drug allergies
Instruct patients
o Report excessive sedation, confusion, or
hypotension
o Avoid driving or operating heavy machinery,
consuming alcohol or other CNS depressants
o Not to take these medications with other
prescribed or over-the-counter medications
without checking with prescriber
Best tolerated when taken with meals reduces GI upset
If dry mouth occurs, teach patient to perform frequent mouth care, chew gum, or suck
on hard candy (preferably sugarless) to ease discomfort
Monitor for intended therapeutic effects
Nasal Congestion
Excessive nasal secretions
Inflamed and swollen nasal mucosa
Primary causes
o Allergies
o Upper respiratory infections (URIs; common cold)
Decongestants: Types
Three main types are used
o Adrenergics Largest group
Sympathomimetics
o Anticholinergics
Less commonly used
Parasympatholytics
o Corticosteroids
Topical, intranasal steroids
Oral Decongestants
Prolonged decongestant effects, but delayed onset
Effect less potent than topical
No rebound congestion
Exclusively adrenergics
Example: pseudoephedrine
Topical Nasal Decongestants
Topical adrenergics
o Prompt onset
o Potent
o Sustained use over several days causes rebound congestion, making the
condition worse
Examples
o Adrenergics: ephedrine, oxymetazoline, and tetrahydrozoline
o Others: phenylephrine
Inhaled Intranasal Steroids and Anticholinergic Drugs
Not associated with rebound congestion
Often used prophylactically to prevent nasal congestion in patients with chronic upper
respiratory tract symptoms
Examples
o Intranasal steroids: beclomethasone dipropionate, budesonide, flunisolide,
fluticasone, triamcinolone, ciclesonide
o Intranasal anticholinergic: ipratropium
Nasal Decongestants: Mechanism of Action
Site of action: blood vessels surrounding nasal sinuses
Adrenergics
o Constrict small blood vessels that supply upper respiratory tract structures
o As a result these tissues shrink nasal secretions in the swollen mucous
membranes are better able to drain
Nasal steroids
o Anti-inflammatory effect
o Work to turn off the immune system cells involved in the inflammatory response
o Decreased inflammation results in decreased congestion
o Shrink engorged nasal mucous membranes
o Relieve nasal stuffiness
Nasal Decongestants: Clinical Indications Relief of nasal congestion associated with
o Acute or chronic rhinitis
o Common cold
o Sinusitis
o Hay fever
o Other allergies
o Used to reduce swelling of the nasal/pharyngeal membranes before surgery or
diagnostic procedures
Nasal Decongestants: Contraindications
Drug allergy
Narrow-angle glaucoma
Uncontrolled cardiovascular disease, HTN
Diabetes and hyperthyroidism
History of cerebrovascular accident (CVA) or transient ischemic attacks (TIAs)
Long-standing asthma
BPH
Nasal Decongestants: Adverse Effects
Adrenergics
o Nervousness
o Irritation
o Insomnia
o Palpitations
o Tremors
Steroids
o Local mucosal dryness and irritation
Systemic sympathomimetic drugs and sympathomimetic nasal decongestants are likely
to cause drug toxicity when given together.
Nasal Decongestants: Interactions
Systemic sympathomimetic drugs and sympathomimetic nasal congestant are likely to
cause drug toxicity when given together
Monoamine oxidase inhibitors and sympathomimetic nasal decongestants raise blood
pressure.
Methyldopa
Urinary acidifiers and alkalinizers
Nasal Decongestants: Nursing Management
Assess for drug allergies
Decongestants hypertension, palpitations, CNS
stimulation
o Avoid in patients with these conditions
Patients on medication therapy for hypertension
should check with their HCP before taking OTC
decongestants
Avoid caffeine and caffeine-containing products Report a fever, cough, symptoms lasting longer than a week
Monitor for intended therapeutic effects
Cough Physiology
Respiratory secretions and foreign objects are naturally removed by the cough reflex
o Induces coughing and expectoration
o Initiated by irritation of sensory receptors in the respiratory tract
o Two basic types of cough
Productive: congested; removes excessive secretions
Nonproductive: dry cough
Coughing is mostly beneficial, but can be harmful in certain situations
Antitussives
Drugs used to stop or reduce coughing
Opioid and non-opioid
Used only for nonproductive coughs!
May be used in cases where coughing is harmful
Antitussives: Mechanism of Action
Opioids
o Suppress the cough reflex by direct action on the cough center in the medulla
o Analgesia, drying effect on the mucosa of the respiratory tract, increased
viscosity of respiratory secretions, reduction of runny nose and postnasal drip
o Examples:
codeine
hydrocodone
Nonopioids
o Suppress the cough reflex by numbing the stretch receptors in the respiratory
tract preventing the cough reflex from being stimulated
o No analgesic properties no CNS depression
o Examples:
benzonatate (Tessalon pearls)
dextromethorphan (Rubitussin DM or DXM)
Antitussives: Indications and Contraindications
Indications
o Used to stop the cough reflex when the cough is nonproductive harmful
Contraindications
o Drug allergy
o Opioid dependency
o Respiratory depression
Antitussives: Adverse Effects
benzonatate (Tessalon p)
o Dizziness, headache, sedation, nausea, and others
dextromethorphan (R DM)
o Dizziness, drowsiness, nausea
Opioids (Codeine)o Sedation, nausea, vomiting, lightheadedness, constipation
Antitussives: Nursing Management
Perform respiratory, cough assessment, & allergies
Instruct patients to avoid driving or operating heavy equipment because of possible
sedation, drowsiness, or dizziness
Report the following:
o Cough that lasts more than a week
o A persistent headache
o Fever
o Rash
Patients taking chewable tablets or lozenges should not drink liquids for 30 to 35
minutes afterward
Monitor for intended therapeutic effects
Expectorants
Drugs that aid in the expectoration (removal) of mucus
Reduce the viscosity of secretions: drink fluids!
Disintegrate and thin secretions
o Example: guaifenesin (Mucinex)
Expectorants: Mechanism of Action
Reflex stimulation
o Drug causes irritation of the GI tract
o Loosening and thinning of respiratory tract secretions occur in response to this
irritation
Direct stimulation
o The secretory glands are stimulated directly to increase their production of
respiratory tract fluids
Result thinner mucus that is easier to remove
Drug Effect: by loosening and thinning sputum and bronchial secretions indirectly
diminishes coughing
Expectorants: Clinical Indications
Used for relief of productive coughs
o Common colds
o Bronchitis
o Laryngitis
o Pharyngitis
o Coughs chronic paranasal sinusitis
o Pertussis
o Influenza
o Measles
Expectorants: Nursing Management
Use cautiously in the older patients or those with asthma or respiratory insufficiency
Encourage fluid intake loosen and liquefy secretions
Report: fever, cough, or other symptoms longer than a week Monitor for intended therapeutic effects
Supplements and Herbal Products
Vitamin C
Goldenseal
Echinacea
o Herbal plant (daisy family )
o Reduces symptoms of the common cold and recovery time
o Adverse effects
Dermatitis
GI disturbances
Dizziness
Headache
Respiratory Drugs
Lower Respiratory Tract Diseases: Asthma
Persistent and present (air flow obstruction) most of the time despite treatment
Recurrent and reversible shortness of breath
Occurs when the airways of the lungs become narrow as a result of:
o Bronchospasms
o Inflammation of the bronchial mucosao Edema of the bronchial mucosa
o Production of viscous mucus
Alveolar ducts/alveoli remain open, airflow to them is obstructed
Symptoms
o Wheezing
o Difficulty breathing
Four categories
o Intrinsic: idiopathic
o Extrinsic: allergen
o Exercise induced
o Drug induced: NSAIDs, beta blocker, sulfites, etc
Status asthmaticus**
o Prolonged asthma attack that does not respond to typical
drug therapy
o May last several minutes to hours
o Medical emergency**: open airway asap rocky, give a short acting inhaled beta 2
agonist
Lower Respiratory Tract Diseases: Chronic Obstructive Pulmonary Disease (COPD)
Chronic bronchitis
o Continuous inflammation and low-grade infection of the bronchi
o Excessive secretion of mucus and certain pathologic changes in the bronchial
structure
o Often occurs as a result of prolonged exposure to bronchial irritants
Emphysema
o Air spaces enlarge as a result of the destruction of alveolar walls
o The surface area where gas exchange takes place is reduced
o Effective respiration is impairedBronchodilators
Relax the bronchial smooth muscle dilation of the bronchi and bronchioles that are
narrowed as a result of the disease process
Three classes
o Beta-adrenergic agonists
o Anticholinergics
o Xanthine derivatives
Beta-Adrenergic Agonists: Short and Long-Acting Examples
Short-acting beta agonist (SABA) inhalers (given in asthma attacks)
o albuterol (Ventolin)* know
o levalbuterol (Xopenex)* know
o pirbuterol
o terbutaline
o metaproterenol (Alupent)* know
Long-acting beta agonist (LABA) inhalers (given in maintenance)
o arformoterol (Brobana)* know
o formoterol
o salmeterol (severent)* know
o indacterol
o vilanterol in conjunction
fluticasone (Breo Ellipta)
umeclidinium (anticholinergic; Anoro Ellipta)
Beta-Adrenergic Agonists
Used during acute phase of asthmatic attacks
Quickly reduce airway constriction and restore normal airflow
Three Types know these
o Nonselective adrenergic agonists
Stimulate alpha, beta1 (cardiac), and beta2 (respiratory) receptors
Example: epinephrine
o Nonselective beta-adrenergics
Stimulate both beta1 and beta2 receptors Example: metaproterenol
o Selective beta2 drugs
Stimulate only beta2 receptors
Example: albuterol
Beta-Adrenergic Agonists: Mechanism of Action
Activation of beta2 receptors activates cyclic adenosine monophosphate (cAMP)
relaxes smooth muscle in the airway bronchial dilation and increased airflow
Beta-Adrenergic Agonists
Indications
o Relief of bronchospasm related to asthma, bronchitis, and other pulmonary diseases
o Used in treatment and prevention of acute attacks
o Used in hypotension and shock
Contraindications
o Known drug allergy
o Uncontrolled HTN*
o Cardiac dysrhythmias*
o High risk of stroke
Related to vasoconstrictive drug action**
Adverse Effects
o Alpha and beta (epinephrine)
Insomnia
Restlessness*
Anorexia
Vascular headache
Hyperglycemia
Tremor
Cardiac stimulation
o Beta1 and beta2 (metaproterenol)
Cardiac stimulation
Tremor*
Anginal pain
Vascular headache
Hypotensiono Beta2 (albuterol)
Hypotension or HTN
Vascular headache
Tremor
Beta-Adrenergic Agonists: Interactions
Diminished bronchodilation when nonselective beta blockers are used with the beta
agonist bronchodilators
Monoamine oxidase inhibitors (enhance HTN crisis)
Sympathomimetics
Monitor patients with diabetes; an increase in blood glucose levels can occur.
Beta-Adrenergic Agonists
Albuterol
o Short-acting beta2-specific bronchodilating beta agonist
o Most used drug in this class
o Must not be used too frequently**
o Oral and inhalational use
o Including metered-dose inhalers (MDIs)**
Salmeterol
o Long-acting beta2 agonist bronchodilator
o Never to be used for acute treatment
o Used for the maintenance treatment of asthma and COPD and in conjunction with
an inhaled corticosteroid
o Should never be given more than twice daily nor should the maximum daily dose
(one puff twice daily) be exceeded
Beta-Adrenergic Agonists: Nursing Implications
Albuterol, if used too frequently, loses its
beta2-specific actions at larger doses
stimulates beta1 receptors causing
nausea, increased anxiety, palpitations,
tremors, and increased heart rate
Ensure that patients take medications
exactly
as prescribed, with no omissions or
double doses
Inform patients to report insomnia,
jitteriness, restlessness, palpitations,
chest pain, or
any change in symptomsAnticholinergics
Used to prevent bronchoconstriction/bronchospasm associated with COPD
NOT used for acute exacerbations!
Examples
o Ipratropium (Atrovent)**similar to atropine
o Tiotropium (Spiriva)**
o Aclidinium (Tudorza)
Anticholinergics: Mechanism of Action
Acetylcholine (ACh) causes bronchial constriction and narrowing of the airways
anticholinergics bind to the ACh receptors prevents ACh from binding airways
dilate preventing bronchoconstriction
Indirectly cause airway relaxation and dilation
Help reduce secretions in COPD patients
Used to prevent bronchospasm associated with COPD not for acute symptoms
Anticholinergics: Adverse Effects
Dry mouth or throat
Nasal congestion
Heart palpitations
Gastrointestinal (GI) distress
Headache
Coughing
Anxiety
Anticholinergics: Ipratropium
Oldest and most commonly used
anticholinergic bronchodilator
Available both as a liquid aerosol for
inhalation and as a multidose inhaler
Usually dosed twice daily
Others:
o tiotropium (Spiriva)
o aclidinium (Tudorza)
o umeclidinium
Xanthine Derivatives
Plant alkaloids
o Caffeine, theobromine, and theophylline
o Only theophylline is used as a bronchodilator
Used in COPD patients as a last resource
Synthetic xanthines
o Aminophylline (it has to change to thophyline before it affects body) and dypillineXanthine Derivatives: Mechanism of Action
Increase levels of energy-producing cAMP inhibiting phosphodiesterase (PDE), the
enzyme that breaks down cAMP increased cAMP intracellular levels causes: smooth
muscle relaxation, bronchodilation, and increased airflow
Drug Effects: Cause bronchodilation by relaxing smooth muscle in the airways relief
of bronchospasm and greater airflow into and out of the lungs
o CNS stimulation: into the medullary respiratory center
o CV stimulation positive inotropic effect, positive chronotropic effect increased
cardiac output and blood flow to the kidneys (diuretic effect)
Xanthine Derivatives: Indications
Dilation of airways in asthmas, chronic bronchitis, and emphysema
Mild to moderate cases of acute asthma
NOT for management of acute asthma attack
Adjunct drug in the management of COPD
Not used as frequently because of potential for drug interactions and variables related
to drug levels in the blood
Xanthine Derivatives: Adverse Effects
Nausea, vomiting, anorexia
Gastroesophageal reflux during sleep
Sinus tachycardia, extrasystole, palpitations, ventricular dysrhythmias **
Transient increased urination *
Hyperglycemia
Xanthine Derivatives
Caffeine
o Used without prescription as a CNS stimulant or analeptic to promote alertness (for
long-duration driving or studying)
o Cardiac stimulant in infants with bradycardia *
o Enhancement of respiratory drive in infants
Theophylline
o Most used xanthine derivative
o Oral, rectal, injectable (as aminophylline), and topical dosage forms
o Aminophylline: intravenous (IV) treatment of patients with status asthmaticus who
have not responded to fast-acting beta agonists (epinephrine) **
o Therapeutic range for theophylline blood level is 10 to 20 mcg/mL (most clinicians
now advise levels between 5 and 15 mcg/mL)
Xanthine Derivatives: Nursing Implications
Contraindications: history of PUD or GI disorders**
Cautious use: cardiac disease
Timed-release preparations should not be crushed or chewed causes gastric irritation
Report to prescriber:
o Nausea
o Vomiting
o Restlessnesso Insomnia
o Irritability
o Tremors
Xanthine Derivatives: Nursing Implications
Be aware of drug interactions with cimetidine, oral contraceptives, allopurinol, certain
antibiotics, influenza vaccine- can increase Xanthine levels (decrease dose)
Cigarette smoking, Rifampin & St Johns wart enhances xanthine metabolism which
decrease theopilline levels (increase dose)
Interacting foods include charcoal-broiled, high-protein, and low-carbohydrate foods
o May reduce serum levels of xanthines through various metabolic mechanisms
Nonbronchodilating Respiratory Drugs
Leukotriene Receptor Antagonists (LTRAs): (monteluksat, zafirkulast and zileuton)
Corticosteroids: (beclomethasone, budesonide,…
Mast Cell stabilizers: rarely used cromolyn and nedocromil, which are sometimes used
for exercise-induced asthma
Leukotrienes & LTRAs
Leukotrienes are substances released when a trigger, such as cat hair or dust, starts a
series of chemical reactions in the body
o Leukotrienes inflammation, bronchoconstriction, and mucus production
coughing, wheezing, shortness of breath
LTRAs mechanism of action prevent leukotrienes from attaching to receptors on cells
in the lungs and circulation inflammation in lungs is blocked relieving asthma
symptoms
Nonbronchodilating
Newer class of asthma medications
Currently available drugs
o montelukast **
o zafirlukast
o zileuton
LRTAs: Drug Effects
By blocking leukotrienes:
o Prevent smooth muscle contraction of the bronchial airways
o Decrease mucus secretion
o Prevent vascular permeability
o Decrease neutrophil and leukocyte infiltration to the lungs preventing
inflammation
LRTAs: Indications & Contraindications
Indications
o Prophylaxis and long-term treatment and prevention of asthma in adults and
children 12 years and older
o NOT meant for management of acute asthmatic attacks
o Montelukast is approved for treatment of allergic rhinitis
o Improvement with use is typically seen in 1 week * Contraindications
o Known drug allergy
o Previous adverse drug reaction
o Allergy to povidone, lactose, titanium dioxide, or cellulose derivatives
These are inactive ingredients in these drugs
LRTAs: Adverse Effects
zileuton
o Headache, nausea, dizziness, insomnia
zafirlukast and montelukast
o Headache, nausea, diarrhea
Montelukast (PO) has fewer interactions
o Phenobarbital and rifampin decrease the concentration of this
LRTAs: Nursing Implications
Ensure that the drug is being used for chronic management of asthma, not acute asthma
Teach the patient the purpose of the therapy
Improvement should be seen in about 1 week
Advise patients to check with prescriber before taking over-the-counter (OTC) or
prescribed medications to determine drug interactions
Assess liver function before beginning therapy and throughout
Teach patient to take medications every night on a continuous schedule, even if
symptoms improve***
Corticosteroids (Glucocorticoids)
Antiinflammatory properties
Used for chronic asthma
Do not relieve symptoms of acute asthmatic attacks
Oral or inhaled forms
o Inhaled forms reduce systemic effects
May take several weeks before full effects are seen
Corticosteroids: Mechanism of Action
Stabilize membranes of cells that release harmful bronchoconstricting substances
(leukocytes or white blood cells)
Increase responsiveness of bronchial smooth muscle to beta-adrenergic stimulation
Dual effect of both reducing inflammation and enhancing the activity of beta agonists
Shown to restore in increase the responsiveness of bronchial smooth muscle to betaadrenergic receptor stimulation more pronounced stimulation of beta2 receptors by
beta agonist drugs (albuterol)
Inhaled Corticosteroids
beclomethasone dipropionate (Beclovent)*
budesonide (Pulmicort Turbuhaler)*
ciclesonide
flunisolide
fluticasone (Flovent- oral inhaler, Flonase- nose inhaler)
mometasone triamcinolone acetonide (Azmacort)**
Corticosteroids: Indications
Treatment of bronchospastic disorders to control the inflammatory response that cause
these disorders
Used for persistent asthma
Often used concurrently with beta-adrenergic agonists
Systemic corticosteroids are used only to treat acute exacerbations or severe asthma
IV corticosteroids: acute exacerbation of asthma or COPD
Corticosteroids: Contraindications
Drug allergy
Not intended as sole therapy for acute asthma attacks
Hypersensitivity to glucocorticoids
Patients whose sputum tests positive for Candida organisms
Patients with systemic fungal infection
Causes immune suppressions
Inhaled Corticosteroids: Adverse Effects
Pharyngeal irritation
Coughing
Dry mouth
Oral fungal infections
Systemic effects are rare
because low doses are used for
inhalation therapy
Inhaled Corticosteroids: Drug
Interactions
Drug interactions are more likely
to occur with systemic (versus
inhaled) corticosteroids
May increase serum glucose
levels, possibly requiring
adjustments in dosages of
antidiabetic drugs
Cyclosporine and tacrolimus
Itraconazole
Phenytoin, phenobarbital, and rifampin
Inhaled Corticosteroids: Nursing Implications
Teach patients to gargle and rinse the mouth with lukewarm water afterward to prevent
the development of oral fungal infections
Teach patients to monitor disease with a peak flow meter
Encourage use of a spacer device to ensure successful inhalations
Teach patient how to keep inhalers and nebulizer equipment clean after uses If a beta agonist bronchodilator and corticosteroid inhaler are both ordered, the
bronchodilator should be used several minutes before the corticosteroid to provide
bronchodilation before administration of the corticosteroid
Phosphodiesterase-4 Inhibitor
roflumilast (Daliresp)
o Indicated to prevent coughing and excess mucus from worsening and to decrease
the frequency of life-threatening COPD exacerbations**
o Adverse effects include nausea, diarrhea, headache, insomnia, dizziness, weight loss,
and psychiatric symptoms
Monoclonial Antibody Antiasthmatic
omalizumab, mepolizumab, reslizumab
o Add-on therapy for treatment of asthma
o Selectively binds to the immunoglobulin IgE, which in turn limits the release of
mediators of the allergic response
o Given by injection**
o Potential for producing anaphylaxis
o Monitor closely for hypersensitivity reactions
Nursing Implications: All Respiratory Drugs
Encourage patients to take measures that promote a generally good state of health to
prevent, relieve, or decrease symptoms of COPD
o Avoid exposure to conditions that precipitate bronchospasm (allergens, smoking,
stress, air pollutants)
o Adequate fluid intake
o Compliance with medical treatment
o Avoid excessive fatigue, heat, extremes in temperature, caffeine
Encourage patients to get prompt treatment for flu or other illnesses, and to get
vaccinated against pneumonia or flu
Encourage patients to always check with their physician before taking any other
medication, including OTC medications
Perform a thorough assessment before beginning therapy, including:
o Skin color
o Baseline vital signs
o Respirations (should be between 12 and 24
breaths/min)
o Respiratory assessment, including pulse oximetry
o Sputum production
o Allergies
o History of respiratory problems
o Other medications
o Smoking history
Teach patients to take bronchodilators exactly as
prescribed Ensure that patients know how to use inhalers and MDIs, and have patients
demonstrate use of the devices
Monitor for adverse effects
Monitor for therapeutic effects
Decreased dyspnea
Decreased wheezing, restlessness, and anxiety
Improved respiratory patterns with return to normal rate and quality
Improved activity tolerance
Decreased symptoms and increased
ease of breathing
Inhalers: Patient Education
Ensure that the patient can self-administer the medication
Provide demonstration and return demonstration
Ensure that the patient knows the correct time intervals for inhalers
Provide a spacer if the patient has difficulty coordinating breathing with inhaler
activation
Ensure that the patient knows how to keep track of the number of doses in the inhaler
device
Antitubercular Drugs- Chapter 41Antitubercular Drugs
Tuberculosis (TB)
o Caused by Mycobacterium tuberculosis (MTB)
Antitubercular drugs treat all forms of Mycobacterium
TB is most characterized by granulomas in the lungs
Common infection sites
o Lung (primary site)
o Brain (cerebral cortex)
o Bone (growing end)
o Liver
o Kidney
Mycobacterium Infections
Aerobic bacillus**
Passed from infected:
o Humans
o Cows (bovine)
o Birds (avian)
Much less common
Tubercle bacilli (MTB)
o Droplet transmission
enter body by inhalation
spread to other organs via
blood & lymphatic systems
o May become dormant or
walled off by calcified or
fibrous tissue
Very slow-growing organism**
More difficult to treat than most
other bacterial infections
First infectious episode: primary TB infection
Reinfection: chronic form of the disease
Dormancy: may test positive for exposure but are not necessarily infectious because of
this dormancy process
Incidence/Timeline
1950s TB in the United States
TB incidence decreased in most years until about 1985
1985: TB incidence began to rise for the first time in 20 years because of the
development of TB in patients coinfected with HIV
1992: There was a resurgence peak in the United States, but it has decreased since that
time
o Decline is attributed to intensified public health efforts aimed at preventing,
diagnosing, and treating TB as well as HIV infection
Concern now: increasing number of multidrug-resistant tuberculosis (MDR-TB) casesMultidrug-Resistant Tuberculosis (MDR-TB)
TB infects one third of the world’s population.
MDR-TB that is resistant to both isoniazid (INH) and rifampin
Extensively drug-resistant tuberculosis (XDR-TB): relatively rare type of MDR-TB,
resistant to almost all drugs used to treat TB, including the two best first-line drugs, INH
and rifampin, as well as to the best second-line medications
XDR-TB is of special concern for patients who have AIDS or are otherwise
immunocompromised.
Use of multiple medications to treat TB due to increasing presence of resistance
TB Diagnosis
Antitubercular Drugs
First-line drugs
o isoniazid (INH)*
o rifapentine
o ethambutol
o rifabutin
o pyrazinamide (PZA)
o rifampin
o streptomycin
o *Primary drug used
Second-line drugs
o capreomycin
o cycloserine
o levofloxacin
o ethionamide
o ofloxacin
o kanamycin
o para-aminosalicyclic acid (PAS)Tuberculosis-Related Injections
Purified protein derivative
(PPD)
A diagnostic injection given
intradermally in doses of 5
tuberculin units (0.1 mL) to
detect exposure to the
tuberculosis (TB) organism
Positive result is indicated by
induration (not erythema) at
the site of injection
Bacille Calmette-Guérin (BCG)
o A vaccine injection
derived from an
inactivated strain of
Mycobacterium bovis
o Used in much of the
world to vaccinate
young children against TB
o Does not prevent infection
o Reduces active TB by 60% to 80%
o Effective at preventing more severe cases involving dissemination of infection
throughout the body
o Can cause false-positive results on the tuberculin skin test
o Not done in the us
o Will give a false positive test if test given after this injection
Antitubercular Therapy Considerations
Major effects: reduction of cough and reduction of infectiousness
o Normally occurs within 2 weeks of initiation of drug therapy if TB strain is drug
sensitive**
Most cases of TB can be cured
Successful treatment: several antibiotic drugs for at least 6 months and sometimes for
as long as 12 months
Perform drug-susceptibility testing on the first Mycobacterium spp. that is isolated from
a patient specimen to prevent the development of multidrug-resistant TB (MDR-TB)
Even before the results of susceptibility tests are known, begin a regime with multiple
antitubercular drugs to reduce the chances of resistance
Adjust drug regimen after the results of susceptibility testing are known
Monitor patient compliance closely during therapy
Problems with successful therapy occur because of patient nonadherence to drug
therapy and the increased incidence of drug-resistant organisms
Mechanism of Action
Three groupso Protein wall synthesis inhibitors: streptomycin, kanamycin, capreomycin,
rifampin, rifabutin, others
o Cell wall synthesis inhibitors: cycloserine, ethionamide, INH
o Other mechanisms of action: ethambutol, INH, PAS
Antitubercular Therapy
Effectiveness depends on:
o Type of infection
o Adequate dosing
o Sufficient duration of treatment
o Adherence to drug regimen
o Selection of an effective drug
combination
Problems:
o Drug-resistant organisms
o Drug toxicity
o Patient nonadherence
MDR-TB
Bedaquiline (Sirturo)
First drug approved in over 40 years
Treatment of multidrug-resistant TB
Inhibits mycobacterial ATP synthase
Adverse effects: headache, chest pain, nausea, and QT prolongation**
Interactions: alcohol, mifepristone, other drugs with high risk for causing QT
prolongation
Administer with food**
Ethambutol (Myambutol)
First bacteriostatic drug used in
treatment of TB
Diffuses into the mycobacteria
and suppresses RNA synthesis,
inhibiting protein synthesis
Used in combination with other
actions
Contraindications: optic neuritis,
pediatric patients (younger than
13)
Adverse effects: retrobulbar
neuritis, blindness
Isoniazid (INH)
Drug of choice for TB
Resistant strains of
Mycobacterium emerging
Metabolized in the liver throughacetylation—watch for “slow acetylators” (adjust dose downwards)
Used alone or in combination with other drugs
Contraindicated with liver disease
Black-box warning regarding possible hepatitis
Adverse effects: peripheral neuropathy, hepatotoxicity
Pyridoxine (Vitamin B6) may be used to combat neuropathy adverse effects *
Pyrazinamide (PZA)
Bacteriostatic or bactericidal
Used in combination with other agents
Inhibits lipid and nucleic acid synthesis in mycobacteria
Contraindications:
Severe hepatic disease
Acute gout
Rifabutin , Rifampin, and Rifapentine
Rifamycin antibiotic
Also used to treat infections caused by non-TB mycobacterial species
Adverse effects
o Turns urine, feces, saliva, skin, sputum, sweat, and tears a red-orange-brown
color (know! It is specific for these three meds)
o Tell patient that they can keep taking pills but to use other forms of brith control
as they are more likely to get pregnent
o Hepatitis***
Causes oral contraceptive to become ineffective another form of birth control
needed
Streptomycin
Aminoglycoside antibiotic
Used in combination with other agents
Injectable form only
Nursing Management
Obtain a thorough medical history and assessment
Perform liver function studies in patients who are to receive INH or rifampin
(especially in elderly patients or those who use alcohol daily)
Assess for contraindications to the various drugs, conditions for cautious use, and
potential drug interactions
Patient education is critical
Therapy may last for up to 24 months
Take medications exactly as ordered, at the same time, every day
Emphasize the importance of strict adherence to regimen for improvement of condition
or cure
Remind patients that they are contagious during the initial period of their illness—
instruct in proper hygiene and prevention of the spread of infected droplets
Teach patients to take care of themselves, including adequate nutrition and rest Patients should not consume alcohol while on these medications or take other
medications, including over-the-counter (OTC) medications, unless they check with their
prescriber
Oral preparations may be given with meals to reduce gastrointestinal upset, even
though recommendations are to take them 1 hour before or 2 hours after meals
Monitor for adverse effects:
o Instruct patients on the adverse effects that should be reported to the prescriber
immediately: fatigue, nausea, vomiting, numbness and tingling of the
extremities, fever, loss of appetite, depression, jaundice
Monitor for therapeutic effects:
o Decrease in symptoms of TB, such as cough
and fever (and weight gain)
o Lab studies (culture and sensitivity tests)
and chest x-ray should confirm clinical findings
o Watch for lack of clinical response to therapy, indicating possible drug resistance
Anti-inflammatory and Antigout Drugs
Nonsteroidal Anti-inflammatory Drugs (NSAIDs)
Large and chemically diverse group of drugs with the following properties:
o Analgesic
o Anti-inflammatory
o Antipyretic
o Aspirin-platelet inhibition
Properties all NSAIDs share:
o Antipyretic
o Analgesic
o Anti-inflammatory
NSAIDs
NSAIDs are also used for the relief of:
o Mild to moderate headaches
o Myalgia
o Neuralgia
o Arthralgia
o Alleviation of postoperative pain
o Relief of the pain in arthritic disorders
Rheumatoid arthritis, juvenile arthritis, ankylosing spondylitis, and
osteoarthritis
o Treatment of gout and hyperuricemia**
NSAIDs: Mechanism of Action
Inhibition of the leukotriene pathway, the prostaglandin pathway, or both blocking
the chemical activity of cyclooxygenase (COX)
o Cyclooxygenase-1 (COX-1) Maintains normal lining of the stomach (GI mucosa)
Involved in kidney and platelet function
o Cyclooxygenase-2 (COX-2)
Present primarily at sites of inflammation
Aspirin
o Irreversible inhibitor of COX-1 receptors within the platelets reduces
formation of thromboxane A2 (promotes platelet aggregation)
o Other NSAIDs lack these antiplatelet effects
NSAIDs: Contraindications and Interactions
Contraindications
o Known drug allergy
o Patients with documented aspirin allergy must not receive NSAIDs
o Conditions that place the patient at risk for bleeding:
Vitamin K deficiency
Peptic ulcer disease (PUD)
o Risk for maternal bleeding and neonatal toxicity
o Watch for syncope!!
Interactions
o Serious interactions can occur when given with:
o Anticoagulants and aspirin: increased risk of bleeding
o Corticosteroids and other ulcerogenic drugs: increased risk of GI ulceration
o Protein bound drugs such as warfarin, sulfonylureas, methotrexate
o Diuretics
o ACE inhibitors: NSAIDs block production of vasodilator/natriuretic
prostaglandins; hyperkalemia, bradycardia syncope
NSAIDs: Adverse Effects
Misoprostol
o Many of the adverse effects of NSAIDs are secondary to their inactivation of
protective prostaglandins that help maintain the normal integrity of the stomach
lining.
o Prevents GI bleeding**
o Synthetic prostaglandin E1 analogue inhibits gastric acid secretion
cytoprotective component
o Mechanism of action: unclear
Gastrointestinal
o Dyspepsia, heartburn, epigastric distress, nausea
o GI bleeding*
misoprostol can be used to reduce these dangerous effects
o Mucosal lesions* (erosions or ulcerations)
Acute renal failure (if dehydration exists)
Noncardiogenic pulmonary edema
Increased risk of myocardial infarction (MI) and stroke (Black-box warning) except
aspirin***o NSAIDs may counteract
cardioprotective effects of aspirin
Altered hemostasis
Hepatotoxicity (acute reversible)
Skin eruption, sensitivity reaction
Tinnitus, hearing loss
NSAIDs and Renal Function
Renal function depends partly on
prostaglandins
Disruption of prostaglandin function by
NSAIDs is sometimes strong enough to
precipitate acute or chronic renal failure
Use of NSAIDs can compromise existing renal
function
Renal toxicity can occur in patients with dehydration, heart failure, liver dysfunction, or
use of diuretics or ACE inhibitors
NSAIDs: Chemical Categories
Salicylates
Acetic acid derivatives
Cyclooxygenase-2 (COX-2) inhibitors
Enolic acid derivatives
Propionic acid derivatives
Salicylates
Salicylic acid (Aspirin)- 81-325mg
prophylactic
o Inhibits platelet aggregation
o Antithrombotic effect: used in the
treatment of MI and other
thromboembolic disorders
o Patients with the lower dose
usually is given because they are
taking other blood thinners
Examples: aspirin, diflunisal, choline magnesium trisalicylate, and salsalate
Indications
o Headache (HA), neuralgia, myalgia, arthralgia
o Pain syndromes as a result of inflammation: arthritis, pleurisy, pericarditis
o Systemic lupus erythematosus (SLE)
o Antipyretic action
Aspirin: Reye’s Syndrome
Acute and potentially life-threatening condition involving progressive neurologic deficits
that can lead to coma and may also involve liver damage Triggered by viral illnesses such as
influenza as well as by salicylate therapy
itself in the presence of a viral illness
Survivors of this condition may or may
not have permanent neurologic damage
Do not give to children and teenagers
Salicylate Toxicity
Cardiovascular (CV): increased heart rate
Central nervous system (CNS): tinnitus,
hearing loss, dimness of vision, HA,
dizziness, mental confusion, lassitude,
drowsiness
Gastrointestinal (GI): nausea, vomiting,
diarrhea
Metabolic: sweating, thirst, hyperventilation, hypo- or hyperglycemia
Acetic Acid Derivatives (analgesic, antiinflammatory, antirheumatic and
antipyretic)
diclofenac sodium
indomethacin (Indocin)**
sulindac
etodolac
ketorolac (Toradol)**
o patient comes in after surgery
is given morphine max limit
for pain. And the pain is not
being relieved. You should
give this med for antiinflammatory purpose.
meclofenamate
mefenamic acid
Indomethacin
o Uses: rheumatoid arthritis, osteoarthritis, acute bursitis or tendonitis, ankylosing
spondylitis, acute gouty arthritis, and treatment of preterm labor
o Promote closure of patent ductus arteriosus (PDA), a heart defect that
sometimes occurs in premature infants
o Oral, rectal, intravenous (IV) use
Ketorolac
o Some antiinflammatory activity
o Used primarily for its powerful analgesic effects (comparable to narcotic drugs)
o Indication: short-term use (up to 5 days) to manage moderate to severe acute
paino Adverse effects: renal impairment, edema, GI pain, dyspepsia, and nausea
COX-2 Inhibitors
celecoxib
o First and only remaining COX-2
inhibitor
o Indicated: osteoarthritis,
rheumatoid arthritis, acute pain
symptoms, ankylosing
spondylitis, and primary
dysmenorrhea
o Adverse effects: headache, sinus
irritation, diarrhea, fatigue,
dizziness, lower extremity edema,
and hypertension
o Little effect on platelet function
o Celecoxib is not to be used in
clients with known sulfa
allergy***
Enolic Acid Derivatives
piroxicam (Feldene)**
o used to treat RA, gouty arthritis and osteoarthritis
o assess GI system before you give it
meloxicam (Mobic)
o used to treat RA, gouty arthritis and osteoarthritis
nabumetone (Relafen)
o better tolerated by GI system than other NSAIDs
o used for OA and RA
Propionic Acid Derivatives
o fenoprofen
o flurbiprofen
o Ibuprofen (Motrin, Advil)
Most commonly used
o ketoprofen
o Naproxen
Second most commonly used
o oxaprozin
Uses: analgesic effects in the management of RA, OA, primary dysmenorrhea, gout,
dental pain, musculoskeletal disorders, antipyretic actions
Gout
Gout: condition that results from inappropriate uric acid metabolism
o Underexcretion of uric acid
o Overproduction of uric acid Uric acid crystals are deposited in tissues and joints, resulting in pain
Hyperuricemia
Antigout Drug Examples
allopurinol (Zyloprim)
febuxostat (Uloric)
colchicine*
probenecid
lesinurad
sulfinpyrazone
Antigout Drugs: Indications
allopurinol (Zyloprim) 200-600 mg/day
(800mg)
o Prevents uric acid production**
o Prevents acute tumor lysis
syndrome
Probenecid (250 to 500 mg PO BID)
o Inhibits the reabsorption of uric
acid in the kidneys increases the excretion of uric acid
Must have good renal function**
Febuxostat (Uloric) (40-80/day max 120 mg)
o Nonpurine selective inhibitor of xanthine oxidase
o More selective for xanthine oxidase than allopurinol
o May pose a greater risk of CV events than allopurinol
colchicine
o Reduces inflammatory response to
the deposits of urate crystals in joint
tissue
o Used for short-term management or
prevention of gout
For acute gout:
Initial dose of 0.6-1.2
mg, followed by 0.6
mg/hr until:
Pain is relieved
Severe nausea and
diarrhea occur
Total of 6 mg has been
administered
o May cause short-term leukopenia
and bleeding into the gastrointestinal or urinary tracts
Lesinurad (Zurampic)
o Uric acid transporter inhibitorso Inhibits the transporter proteins involved in renal uric acid reabsorption resulting
in lower serum uric acid levels and increase renal clearance of uric acid
o Given in combination with xanthine oxidase inhibitor
o Teaching: at least 2 liters of fluid a day to get rid of the uric acid
o Dose: 200mg/day taking with food*
Herbal Products: Glucosamine and Chondroitin
Used to treat the pain of osteoarthritis
Adverse effects
o GI discomfort
o Drowsiness, headache, skin reactions (glucosamine)
Drug interactions
o Enhances effects of warfarin
o May increase insulin resistance(glucosamine)
NSAIDs & Antigout: Nursing Implications
Before beginning therapy, assess for conditions that may be contraindications to
therapy, especially:
o GI lesions or PUD
o Bleeding disorders
Assess for conditions that require cautious use
Perform laboratory studies as indicate:
o Cardiac, renal, and liver function studies
o Complete blood count (CBC)
o Platelet count
Perform a medication history to assess for potential drug interactions
Several serious drug interactions exist
Because these drugs generally cause GI distress, they are often better tolerated if taken
with food, milk, or an antacid to avoid irritation
Explain to patients that therapeutic effects may not be seen for 3 to 4 weeks
Educate clients about the various adverse effects of NSAIDs, and inform them to notify
their prescriber if these effects become severe or if bleeding or GI pain occurs
Inform clients to watch closely for the occurrence of any unusual bleeding
Advise patients that enteric-coated tablets should not be crushed or chewed
Monitor for therapeutic effects, which vary according to the condition being treated
o Decrease in swelling, pain, stiffness, and tenderness of a joint or muscle area
Musculoskeletal Agents: Antirheumatic & Osteoporosis
Rheumatoid Arthritis vs. Osteoarthritis
Rheumatoid Arthritis
o Autoimmune disorder causing inflammation and tissue damage in joints
o Diagnosis primarily symptomatic
o Treatment consists of nonsteroidal anti-inflammatory drugs (NSAIDs) and
DMARDs NSAIDs
DMARDs (Disease-Modifying Antirheumatic Arthritis Drugs)
Osteoarthritis
o Another type of arthritis
o Age-related degeneration of joint tissues
o Pain and reduced function
Disease-Modifying Antirheumatic Drugs (DMARDs)
Modify the disease of RA
Exhibit anti-inflammatory, antiarthritic, and immunomodulating effects
Inhibit the movement of various cells into an inflamed, damaged area, such as a joint
Slow onset of action of several weeks, versus minutes to hours for NSAIDs
Also referred to as slow-acting antirheumatic drugs (SAARDs)
DMARDs
Traditional/Nonbiologic
o Methotrexate **
o Leflunomide (Arava)*
o sulfasalazine
o hydroxychloroquine
Biologic Agents
o adalimumab (Humira)**
o anakinra
o etanercept (Enbrel)
o infliximab (Remicade) **
o adalimumab
o Abatacept (Orencia) **
o rituximab
o tocilizumab (Actemra)
o tofacitinib (Xeljanz) **
newest med
DMARDs
DMARDs provide anti-inflammatory and analgesic effects and can arrest or slow disease
processes associated with RA
Current recommendation of first-line therapy in clients with RA**
Methotrexate: Non-biologic DMARD
Used as baseline therapy in most RA clients
Long acting medication
Typical dose 7.5-25 mg orally or injection once per week (7.5-10mg)
o Always ask when was the last time they took the medication. Specially if you are
a nurse in the emergency room.
Labs: (done prior to starting and then every 2-3 months)
o Hepatitis serologies
o LFTs
o CBCo Creatinine
Adverse effects: (bone marrow suppression*)
o Nausea, diarrhea, fatigue, mouth ulcers, rash, alopecia, pneumonitis, sepsis, liver
disease, Epstein-Barr virus-related lymphoma
Must be taken with folic acid supplements to counteract the bone marrow suppression
May take 3-6 weeks to see onset of antirheumatic action
Leflunomide: Non-biologic DMARD
Treatment of active RA (oral form)
Modulates or alters the responses of the immune system to RA
Antiproliferative, antiinflammatory, and immunosuppressive activity
Adverse effects: diarrhea, respiratory tract infection, alopecia, elevated liver enzymes,
rash
Contraindicated in women who are or may become pregnant
Biologic DMARDs: Can be administered in combination with methotrexate
Abatacept
o Caution if the patient has a history of recurrent infections or chronic obstructive
pulmonary disease
o Patients must be up to date on immunizations before starting therapy.
o May increase risk of infections associated with live vaccines
o May decrease response to vaccines
o IV- q 4 weeks, use filter
Etanercept
o Erelzi is the approved biosimilar product for etanercept.
o Patients must be screened for latex allergy (some dosage forms may contain
latex).
o Onset of action: 1 to 2 weeks
o Contraindicated in presence of active infections
Reactivation of hepatitis and tuberculosis has been reported
SQ
Nursing Implications
Assess for allergies, specifically allergies to
egg proteins, IgG, or neomycin
Assess for conditions that may be
contraindications
Assess baseline blood counts; perform
cardiac, renal, and liver studies
Assess for presence of infection
Do not give medication to the pt if they are
currently sick
Follow specific guidelines for preparation
and administration of drugs
Monitor the client’s response during
therapy Teach clients to report signs of infection immediately
o Sore throat
o Vomiting/diarrhea
o Fever over 100.5°F (38.1°C) or higher
Monitor for therapeutic responses
o Decrease in growth of lesion or mass
o Improved blood counts
o Absence of infection, anemia, and hemorrhage
Monitor for adverse effects
Osteoporosis
Age-related degeneration of joint tissues pain and reduced function
Low bone mass increased risk of fractures
Primarily affects women
o 40% of women over 50 years will develop osteoporotic fracture
20% with this condition are men
Osteoporosis: Risk Factors
European/Asian descent
Slender body build
Early estrogen deficiency
Smoking
Alcohol consumption
Low-calcium diet
Sedentary lifestyle
Family history
Drug Therapy for Osteoporosis
Calcium supplements and
vitamin D may be
recommended for women at
high risk for osteoporosis
Current recommendations are
that women, especially those
older than age 60, consider
taking calcium and vitamin D
supplements for bone health
Bisphosphonates
o Alendronate,
ibandronate,
risedronate, zoledronic
acid
Selective estrogen receptor
modifiers (SERMs)
o Raloxifene, tamoxifen
Hormoneso Calcitonin, teriparatide, denosumab
Bisphosphonates
Work by inhibiting osteoclast-mediated bone resorption indirectly enhances bone
mineral density preventing bone loss
Can reverse lost bone mass and reduce fracture risk
Prevention and treatment of osteoporosis and Paget’s Disease
Examples
o alendronate (Fosamax)*
o ibandronate (Boniva)
o risedronate (Actonel)
o zoledronic acid (Reclast)
Bisphosphonates: Mechanism of Action
Highly selective inhibitor of bone resorption
o Resorption occurs following activation of osteoclasts to breakdown bone and
releases from bone to the blood
Reduction in bone resorption decreased serum calcium & phosphate concentrations
Increased bone mineral density to reverse progression of osteoporosis
Absorbed orally - decreased absorption by 40% if taken with food & beverages (other
than plain water)
Stored in skeleton (not metabolized after absorption) slow release urinary
excretion
Bisphosphonates: Contraindications & Interactions
Drug hypersensitivity
Hypocalcemia
Esophageal dysfunction
Inability to sit or stand upright for at least 30 minutes after taking the medication
Known drug interactions
o Ranitidine: doubles bioavailability of alendronate
o Calcium supplements & antacids: separate doses by 2 hours
o Aspirin: increased risk of GI effects
Advise client to wait at least 30 minutes after taking alendronate before taking any
other drug
Bisphosphonates: Adverse Effects
Headache, GI upset, joint pain
Risk of esophageal burns if medication lodges in esophagus before reaching the stomach
o GI irritation more likely if client does not take with full glass of water
Risk of osteonecrosis of the jaw
o Always tell the dentist you take bisphosphonates as they cannot perform dental
procedures with this. Must run labs first.
Possible severe (incapacitating) bone, joint, or muscle pain
Alendronate (Fosamax)
Oral bisphosphonate First nonestrogen nonhormonal option for preventing bone loss
Inhibits or reverses osteoclastmediated bone resorption
Indications: prevention and
treatment of osteoporosis in
men and in postmenopausal
women as well as treatment
of glucocorticoid-induced
osteoporosis in men and for
the treatment of Paget disease
in women
Bisphosphonates: Nursing
Implications
Ensure that patients have no
esophageal abnormalities and
can remain upright or in a
sitting position for 30 minutes
after the dose
Instruct patients to take
medication upon rising in the morning, with a full glass of water, and
30 minutes before eating.
Emphasize that patients should sit upright for at least 30 minutes after taking the
medication
Selective Estrogen Receptor Modifiers (SERMs)
Stimulate estrogen receptors on bone and increase bone density (protectors of the
bones)
Drugs
o raloxifene (Evista)
o tamoxifen (Nolvadex)
Indications
o Prevention of postmenopausal osteoporosis**
Stimulate estrogen receptors on bone and increase bone density
SERMs: Contraindications
Women with known allergy
Women who may become pregnant**
Venous thromboembolic disorder or history
o Deep vein thrombosis (DVT)
o Pulmonary embolus (PE)
o Retinal vein thrombosis
SERMs: Adverse Effects
Hot flashes
Leg cramps
Increase risk of venous thromboembolism Teratogenic
Leukopenia
SERMs: Nursing Indications
Instruct clients that the medication will need to be discontinued 72 hours before and
during any prolonged immobility (such as surgery or a long trip)** with doctor
approval
Hormones: Calcitonin
Indications: treatment of osteoporosis
Mechanism of actions: Directly inhibits osteoclastic bone resorption
Contraindications: drug allergy or salmon allergy
Adverse effects
o Flushing of the face
o Nausea/diarrhea
o Reduced appetite
Nasal spray most used
Hormones: teriparatide (Forteo)
Mechanism of action: Stimulates bone formation**
Contraindications: drug allergy
Adverse effects
o Chest pain
o Dizziness
o Hypercalcemia
o Nausea
o arthralgia
Hormones: denosumab (Prolia)
Mechanism of action
o Blocks osteoclast activation prevents bone resorption by blocking osteoclast
activation
Given as a subcutaneous injection once every 6 months with daily calcium and vitamin D
Contraindications
o Hypocalcemia
o Renal impairment or failure
o Infection
Adverse effects: infections
Herbal Products: Soy
Relief of menopausal symptoms, osteoporosis prevention
Estrasorb, applied as a lotion
Adverse effects
o Nausea
o Diarrhea
o Abdominal pain
o Estrasorb remains on skin for 8 hours
Nursing Implications Assess baseline vital signs, weight, blood glucose levels, and renal and liver function
study results.
Assess whether the patient smokes.
Assess history and medication history.
Assess contraindications, including potential pregnancy.
Monitor for therapeutic responses.
Monitor for adverse effects.
Anti-parkinson Drugs
Parkinson’s Disease (PD)
Chronic, progressive, degenerative disorder
Affects dopamine-producing neurons in the brain
Caused by an imbalance of two neurotransmitters
o Dopamine: inhibits excitement
o Acetylcholine (ACh): excites cells
Neurotransmitter Abnormality in Parkinson’s Disease
Symptoms occur when about 80% of the dopamine stored in the substantia nigra of the
basal ganglia is depleted
Symptoms can be partially controlled if there
are functioning nerve terminals that can take
up dopamine
Classic symptoms include:
o Tremor
o Rigidity
o Akinesia
o Postural instability
o Staggering gait
o Drooling
A progressive condition
Rapid swings in response to levodopa occur
(“on-off phenomenon”)
o PD worsens when too little dopamine
is present
o Dyskinesia occurs when too much dopamine is present
“Wearing-off phenomenon”
PD-associated dementia
Dyskinesia
Difficulty in performing voluntary movements
Two common types
o Chorea: irregular, spasmodic, involuntary movements of the limbs or facial
muscleso Dystonia: abnormal muscle tone leading to impaired or abnormal movements,
usually in feet
Treatment of Parkinson’s Disease
Full explanation of disease to the patient
Treatment centers on drug therapy
PT, OT, speech therapy important
Severe cases;
o Deep brain stimulation
Pharmacology Overview
Aimed at increasing levels of dopamine
Antagonizes or blocks the effects of ACh
Slows the progression of the symptoms not the disease process
Indirect-Acting Dopaminergics: MAOIs
Dopamine Modulators
Catechol Ortho-Methyltransferase (COMT) Inhibitors
Direct-Acting Dopamine Receptor Agonists
Dopamine Replacements
Anticholinergic drugs
Antihistamines
Indirect-Acting Dopaminergic Drugs
Monoamine Oxidase Inhibitors (MAOIs) break down catecholamines in the CNS,
primarily in the brain
Selegiline and rasagiline are selective MAO-B inhibitors
o Cause an increase in levels of dopaminergic stimulation in the CNS
o Do not elicit the “cheese effect” of the nonselective MAOIs used to treat
depression (if 10 mg or less is used)
o Used as monotherapy or as adjuncts with levadopa
o Contraindications
Known allergy
Concurrent use with meperidine
Adverse effects are usually mild
o Dizziness, insomnia, nausea, diarrhea, chest pain, headache, weight loss
o Doses higher than 10 mg/day may cause more severe adverse effects, such as
hypertensive crisis
Dopamine Modulator (indirect-acting)
amantadine
o Antiviral drug used for treatment of influenza
o Indirect acting
o Causes release of dopamine and other catecholamines from storage sites at the
end of nerve cells that have not yet been destroyed by the disease process
o Blocks reuptake of dopamine into the nerve fibers
o Result: higher levels of dopamine in the synapse between nerves and improved
dopamine neurotransmission between neuronsCOMT Inhibitors
Tolcapone and entacapone
Block COMT, the enzyme that catalyzes the breakdown of the body’s catecholamines
Prolong the duration of action of levodopa; reduce wearing-off phenomenon
Adverse effects:
o GI upset, urine discoloration, can worsen dyskinesia that may already be
present
o Tolcapone: severe liver failure
Direct-Acting Dopamine Receptor Agonists
Two subclasses:
o Nondopamine dopamine receptor
agonists (NDDRAs)
o Dopamine replacement drugs
o Can be used in late or early stages
Nondopamine Dopamine Receptor Agonists (NDDRAs)
Ergot derivatives: bromocriptine
o Works by activating presynaptic dopamine
receptors to stimulate the production of
more dopamine
o Inhibits the production of the hormone
prolactin, which stimulates normal lactation and can be used to treat women
with excessive or undesired breast milk production and prolactin-secreting
tumors
o Used with carbidopa-levadopa so that lower doses of levadopa are needed
o Caution when used for patients with peripheral vascular disease
o Adverse reactions: GI upset, dyskinesias, sleep disturbances
o Drug interactions: erythromycin and adrenergic drugs
Nonergot drugs: pramipexole, ropinirole, and rotigotine
o More specific antiparkinson effects with fewer adverse effects
o Used in both early- and late-stage PD
o May delay the need for levadopa
o Monotherapy or adjunctive therapy
o Also used for restless leg syndrome
Dopamine Replacement Drugs
Dopamine replacement drugs
o Levodopa, carbidopa, carbidopa-levodopa
o Work presynaptically to increase brain levels of dopamine
o Levodopa can cross the blood-brain barrier, and then it is converted to
dopamine
o However, large doses of levodopa needed to get dopamine to the brain also
cause adverse effects
o Carbidopa is given with levodopao Carbidopa does not cross the blood-brain barrier and prevents levodopa
breakdown in the periphery
o As a result, more levodopa crosses the blood-brain barrier, where it can be
converted to dopamine
Levodopa Therapy
Levodopa is taken up by the dopaminergic terminal, converted into dopamine, and then
released as needed
As a result, neurotransmitter imbalance is controlled in patients with early PD who still
have functioning nerve terminals
As PD progresses, it becomes more difficult to control it with levodopa
Ultimately, levodopa no longer controls the PD, and the patient is seriously debilitated
o Generally occurs between 5 and 10 years after the start of levodopa therapy
Adverse effects:
o Confusion
o Involuntary movements
o GI distress
o Hypotension
o Cardiac dysrhythmias
Carbidopa-Levodopa Therapy
Carbidopa: adjunct to treat nausea associated with Sinemet
Sinemet CR: increases “on” time and decreases “off” time
Drug interactions occur with tricyclic antidepressants and other drugs.
Carbidopa-levodopa: best taken on an empty stomach; to minimize GI side effects, it
can be taken with food
Contraindicated in cases of angle-closure glaucoma
Use cautiously in patients with open-angle glaucoma
Adverse effects: cardiac dysrhythmias, hypotension, chorea, muscle cramps, and GI
distress
Interactions: pyridoxine and dietary protein
Anticholinergic Therapy
Anticholinergics block the effects of Ach
Used to treat muscle tremors and muscle
rigidity associated with PD
o These two symptoms are caused by
excessive cholinergic activity
Does not relieve bradykinesia (extremely
slow movements)
SLUDGE: Ach is responsible for causing
increased salivation, lacrimation (tearing
of the eyes), urination, diarrhea,
increased GI motility, and possibly emesis
(vomiting). Anticholinergics have the opposite effects: dry mouth or decreased salivation, urinary
retention, decreased GI motility
(constipation), dilated pupils
(mydriasis), and smooth muscle
relaxation.
benztropine mesylate
o Also used to treat
extrapyramidal symptoms
caused by use of
antipsychotic drugs
o Caution during hot
weather or exercise; may
cause hyperthermia
o Adverse effects:
tachycardia, confusion,
disorientation, toxic
psychosis, urinary
retention, dry throat,
constipation, nausea and
vomiting
o Avoid alcohol
trihexyphenidyl
Antihistamines also have anticholinergic properties
o diphenhydramine (Benadryl)
Nursing Implications
Perform a thorough assessment, nursing history, and medication history
Include questions about the patient’s:
o CNS
o GI and GU tracts
o Psychologic and emotional status
Assess for signs and symptoms of PD
o Masklike expression
o Speech problems
o Dysphagia
o Rigidity of arms, legs, and neck
Assess for conditions that may be contraindications
Administer drugs as directed by manufacturer
Provide patient education regarding PD and the medication therapy
o Don’t stop abruptly
Inform patient not to take other medications with PD drugs unless he or she checks with
physician
When starting dopaminergic drugs, assist patient with walking because dizziness may
occur Administer oral doses with food to minimize GI upset
Encourage patient to force fluids to at least 3000 mL/day (unless contraindicated)
Taking levodopa with MAOIs may result in hypertensive crisis
Patient should be taught not to discontinue anti-parkinson drugs suddenly
Teach patient about expected therapeutic and adverse effects with anti-parkinson drug
therapy
Entacapone may darken the patient’s urine and sweat.
Therapeutic effects of COMT inhibitors may be noticed within a few days; it may take
weeks with other drugs.
Monitor for response to drug therapy
o Improved sense of well-being and mental status
o Increased appetite
o Increased ability to perform ADLs, to concentrate, and to think clearly
o Less intense parkinsonian manifestations, such as less tremor, shuffling gait,
muscle rigidity, and involuntary movements
Antiepileptic Drugs
Epilepsy
Seizure
o Brief episode of abnormal electrical activity in nerve cells of the brain
Convulsion
o Involuntary spasmodic contractions of any or all voluntary muscles throughout
the body, including skeletal, facial, and ocular muscles
Epilepsy
o Chronic, recurrent pattern of seizures
Primary (idiopathic)
o Cause cannot be determined
o Roughly 50% of epilepsy cases
Secondary (symptomatic)
o Distinct cause is identified
Trauma, infection, cerebrovascular disorder
Febrile in young children
Classification of Epilepsy
Generalized onset seizures
o Formerly known as grand mal seizures
o Tonic-clonic seizures: contractions
throughout the body
o Aclonic:
o Myoclonic
o Absence seizures
Partial onset seizures
o Simple (formerly known as petit mal
seizures)o Complex
o Secondary generalized tonic-clonic
Unclassified seizures
Status Epilepticus
Multiple seizures occur with no recovery between them
Result:
o Hypotension
o Hypoxia
o Brain damage
o Death
True medical emergency
Antiepileptic Drugs (AEDs)
Also known as anticonvulsants
Goals of therapy
o To control or prevent seizures while maintaining a reasonable quality of life
o To minimize adverse effects and drug-induced toxicity
AED therapy is usually lifelong
Combination of drugs may be used
Single-drug therapy started before multiple-drug therapy is tried
Serum drug concentrations must be measured
o Therapeutic drug monitoring
o Serum concentrations of phenytoin, phenobarbital, carbamazepine,
levetiracetam, and primidone correlate better with seizure control and toxicity
than do those of valproic acid, ethosuximide, and clonazepam
Antiepileptic drugs traditionally used to manage seizure disorders include:
o Barbiturates
o Hydantoins
o Iminostilbenes plus valproic acid
o Second- and third-generation antiepileptics
Mechanism of Action and Drug Effects
Exact mechanism of action is not known
Pharmacologic effects:
o Reduce nerve’s ability to be stimulated
o Suppress transmission of impulses from one nerve to the next
o Decrease speed of nerve impulse conduction within a neuron
Antiepileptic Drugs: Indications
Prevention or control of seizure activity
Long-term maintenance therapy for chronic, recurring seizures
Acute treatment of convulsions and status epilepticus
Other uses
Antiepileptic Drugs: Adverse Effects
Numerous adverse effects—vary per drug
Adverse effects often necessitate a change in medication Black box warning as of 2008
o Suicidal thoughts and behavior
Long-term therapy with phenytoin may cause gingival hyperplasia, acne, hirsutism, and
Dilantin facies
Antiepileptic Drugs: Interactions
Drug interactions are numerous
Many antiepileptic drugs interact with each other
Induce hepatic metabolism resulting in reduction of effects of other drugs
Interfere with birth control
Avoid grapefruit with carbamazepine
Antiepileptic Drug Listing
Valproic acid
Gabapentin
Lamotrigine
Felbamate
Levetiracetam
Topiramate
Zonisamide
Tiagabine
Pregabalin
Perampanel
Ezogabine
Vigabatrin
Eslicarbazepine
Clobazam
Brivaracetam
Barbiturates: Phenobarbital and Primidone
Primidone is metabolized in the liver to phenobarbital
Most common adverse effect: sedation
Therapeutic effects: serum levels of 10-40 µg/mL
Contraindications: known allergy, porphyria, liver or kidney impairment, and respiratory
illness
Adverse effects: cardiovascular, CNS, GI, and dermatologic reactions
Hydantoins: Phenytoin
Phenytoin has been used as a first-line drug for many years and is a prototypical drug
Adverse effects: gingival hyperplasia, acne, hirsutism, Dilantin facies, and osteoporosis
Therapeutic levels are usually 10-20 µg/mL
Highly protein bound: binds to protein, you will have little protein if at first they had too
much and now it binds to the medication
Intravenous (IV) administration
o Very irritating to veinso Slow IV directly into a large vein through a large-gauge (20-gauge or larger)
venous catheter
o Diluted in normal saline (NS) for IV infusion
o Filter must be used
o Saline flush
Fosphenytoin is an injectable water-soluble prodrug of phenytoin that can be given IM
or IV without causing burning on injection associated with phenytoin
Iminostilbenes: Carbamazepine
Second most prescribed
antiepileptic in US after phenytoin
Autoinduction of hepatic enzymes
o Autoinduction is a process
in which, over time, a drug
stimulates the production
of enzymes that enhance its
own metabolism, which
leads to lower than
expected drug
concentrations
Oxcarbazepine – chemical
analogue of carbamazepine; for
partial seizures
o Adverse reactions:
headache, dizziness, nausea
Ethosuximide
Used in the treatment of uncomplicated absence seizures
Not effective for secondary generalized tonic-clonic seizures
Contraindication: known allergy
Adverse effects: GI and CNS effects
Drug interactions: hepatic enzyme-inducing drugs
Miscellaneous Drugs
Gabapentin
o Chemical analogue of GABA (a neurotransmitter that inhibits brain activity)
o Works by increasing the synthesis and synaptic accumulation of GABA between
neurons
o Used in the treatment of partial seizures and neuropathy
Lamotrigine
o Used for simple or complex partial seizures; also used in treatment of bipolar
disorder
o Common adverse effects: relatively minor CNS and GI symptoms and possible
Stevens-Johnson syndrome
Levetiracetam
o Adjunct therapy for partial seizureso Contraindication: known allergy
o Mechanism of action: unknown
o Adverse effects: generally well tolerated, CNS
o No drug interactions
Pregabalin
o Schedule V controlled substance
o Indication: adjunct therapy for partial seizures
o Other common uses: neuropathic pain, postherpetic neuralgia, and fibromyalgia
Tiagabine
o Adjunct therapy for partial seizures
o Beneficial effects by inhibiting the reuptake of GABA
o Avoid off label use of this drug it can cause paradoxical seizures
o Adverse effects: CNS and GI symptoms
Topiramate
o Adjunct therapy for partial and generalized seizures
o Mechanism of action unknown
o Adverse effects: CNS related, angle-closure glaucoma
Valproic Acid
o Treatment of generalized seizures, bipolar disorder, and controlling partial
seizures
o Highly protein bound
o Adverse effects: drowsiness, GI disturbances, tremor, weight gain, hair loss,
hepatotoxicity, pancreatitis
Zonisamide
o Sulfonamide derivative
o Used for a variety of seizure types
o Adverse effects: CNS and GI symptoms
Nursing Implications
Assessment
o Health history, including current medications
o Drug allergies
o Liver function studies, CBC
o Baseline vital signs
Oral drugs
o Take regularly, same time each day
o Take with meals to reduce GI upset
o Do not crush, chew, or open extended-release forms
o If patient is NPO for a procedure, contact prescriber regarding AED dosage
Intravenous forms
o Follow manufacturer’s recommendations for IV delivery—usually given slowly
o Monitor vital signs during administration
o Avoid extravasation of fluids
o Use only normal saline with IV phenytoin (Dilantin) Teach patients that therapy is long term and possibly lifelong (not a cure)
Monitor for therapeutic effects
o Decreased or absent seizure activity
Monitor for adverse effects
o Mental status changes, mood changes, changes in level of consciousness or
sensorium
o Eye problems, visual disorders
o Sore throat, fever (blood dyscrasias may occur with Dilantin)
Ophthalmic Drugs
Drugs That Affect the Eye
Mydriatics (apraclonidine)
o Dilate the pupil
Miotics (acetylcholine, pilocarpine)
o Constrict the pupil
Cycloplegics (atropine, cyclopentolate)
o Paralyze the ciliary body
o Have mydriatic properties
o Cycloplegia: paralysis of accommodation
Ocular Drugs Antiglaucoma drugs
Antimicrobial and anti-inflammatory drugs
Topical anesthetics
Diagnostic drugs
Antiallergic drugs
Lubricants and moisturizers
Glaucoma
Inhibition of the normal flow and drainage of aqueous humor
Results in increased intraocular pressure (IOP)
Pressure against the retina destroys neurons, leading to impaired vision and eventual
blindness
Types of Glaucoma
Angle-closure glaucoma
Open-angle glaucoma
Also characterized by underlying cause
o Primary
o Secondary
o Congenital
Drugs Used to Reduce IOP
Direct-acting cholinergics
Indirect-acting cholinergics
Adrenergics: sympathomimetics
Anti-adrenergics: beta blockers
Carbonic anhydrase inhibitors (CAIs)
Osmotic diuretics
Prostaglandin agonists
Cholinergic Drugs
Mimic the PSNS neurotransmitter acetylcholine
Also called miotics, cholinergics
Direct-acting and indirect-acting drugs
Cause pupillary constriction (miosis), which leads to reduced IOP caused by increased
outflow of aqueous humor
Direct-acting drugs
o acetylcholine
o carbachol
o pilocarpine
Indirect-acting drugs
o echothiophate
Indications
o Open-angle glaucoma
o Angle-closure glaucoma
o Ocular surgery
o Convergent strabismus (“cross-eye”)o Ophthalmologic exams
Cholinergic Drugs: Adverse Effects
Most limited to local effects
If sufficient amounts enter the bloodstream, systemic effect may occur (most likely with
indirect acting)
o Hypotension, bradycardia, or tachycardia
o Headache, nausea, vomiting, diarrhea, abdominal cramps, asthma attacks
o Others
Sympathomimetics
Mimic the sympathetic neurotransmitters epinephrine and norepinephrine
Stimulate the dilator muscle to contract
o Result is increased pupil size (mydriasis)
Enhance aqueous humor outflow through the canal of Schlemm
o IOP is reduced
apraclonidine
brimonidine
dipivefrin
o Prodrug of epinephrine
o When applied topically
Hydrolyzed to epinephrine
Penetrates tissues better
Indications
o Chronic, open-angle glaucoma (to reduce IOP)
o Reduction of perioperative IOP
o Reduction of ocular hypertension
Sympathomimetics: Adverse Effects
Primarily limited to ocular effects
o Burning
o Eye pain
o Lacrimation
Rare systemic effects
o Hypertension
o Tachycardia
o Extrasystoles
o Headache
o Faintness
Beta-Adrenergic Blockers
betaxolol
carteolol
levobetaxolol
metipranolol
timolol
Reduce IOP by:o Reducing aqueous humor formation
o Increasing aqueous humor outflow
Does not affect pupil size, accommodation, or night vision
Beta-Adrenergic Blockers: Indications
Reduction of elevated IOP
o Chronic open-angle glaucoma
o Ocular hypertension
Treatment of some forms of angle-closure glaucoma
Administration of systemic beta blockers with high doses of ophthalmic beta blockers
may result in additive effects
Beta-Adrenergic Blockers: Adverse Effects
Primarily ocular effects
o Transient burning and discomfort
o Blurred vision
o Pain
o Photophobia
o Others
Limited systemic effects
o Headache
o Dizziness
o Cardiac irregularities
o Bronchospasm
Carbonic Anhydrase Inhibitors
brinzolamide (Azopt)
dorzolamide (Trusopt)
Inhibit the enzyme carbonic anhydrase, which reduces aqueous humor formation in the
eye
Ask for any allergies to sulfide
Result is decreased IOP
Carbonic Anhydrase Inhibitors: Indications
Treatment of glaucoma
o Open angle
o Angle closure
Preoperatively to reduce intraocular pressure
Carbonic Anhydrase Inhibitors: Adverse Effects
Oral forms can produce systemic effects
o Drowsiness, confusion
o Transient myopia, tinnitus
o Anorexia, vomiting, diarrhea
o Several others
Patients with sulfa allergies may develop cross-sensitivities
Osmotic Diuretics
Create ocular hypotension by producing an osmotic gradient Water is forced from the aqueous and vitreous humors into the bloodstream
Result is reduced volume of intraocular fluid, thus reduced IOP
Administered IV, PO, or topically
Glycerin usually tried first
o Can cause hyperglycemia
Mannitol used if glycerin is unsuccessful
Isosorbide and urea may also be used
Indications
o Acute glaucoma episodes
o Before and after ocular surgery to reduce IOP
Adverse effects
o Nausea, vomiting, headache
o May cause fluid and electrolyte imbalance
Prostaglandin Agonists
Newest class of drugs for glaucoma
Three drugs
o latanoprost (Xalatan)
o travoprost (Travatan-Z)
o bimatoprost (Lumigan)
Reduce IOP by increasing the outflow of aqueous fluid
Increase uveoscleral outflow of fluid
Used in the treatment of glaucoma
Most drugs allow for single daily dosing because of effects lasting for 20 to 24 hours
Effects on eye color
o In some persons with hazel, green, or blue/brown eyes, eye color will change
permanently to brown
o Color change occurs even if medication stopped
Ocular Antimicrobial Drugs
Topical and systemic administration
o Antibacterial
o Antiviral
o Antifungal
o Topical application may cause transient and local inflammation, burning, and
stinging
Use of ophthalmic antibiotics with corticosteroids may make it more difficult to rid the
eye of infection
Aminoglycosides
o Antibacterial
o gentamicin (Garamycin) , tobramycin (Tobrex)
Macrolides
o Antibacterial
o erythromycin, azithromycin, otherso Erythromycin also is used for prevention of Neisseria gonorrhoeae eye infections
in newborns
o Treatment of neonatal conjunctivitis caused by Chlamydia trachomatis
o Polypeptides
o Antibacterial
o bacitracin (AK-Tracin), polymyxin B
Quinolones
o ciprofloxacin (Ciloxan)
o gatifloxacin (Zymar)
o moxifloxacin (Vigamox)
o levofloxacin (Quixin)
o ofloxacin (Ocuflox)
Sulfonamides
o sulfacetamide (Bleph-10)
o sulfisoxazole (Gantrisin)
Ocular Antifungal Drugs
natamycin (Natacyn)
o Used topically to treat
Blepharitis
Conjunctivitis
Keratitis
ganciclovir (Vitrasert)
o Treatment of ocular cytomegalovirus (CMV)
o Administered by surgical implant in the eye
fomivirsen (Vitravene)
o Treatment of ocular CMV
o Administered by surgical implant in the eye
trifluridine (Viroptic,1% ophthalmic drops)
o Used for ocular infections (keratitis and keratoconjunctivitis) caused by types 1
and 2 of the herpes simplex virus
o Applied topically as drops
o Significant adverse effects include secondary glaucoma, corneal punctate
defects, uveitis, and stromal edema (edema in the tough, fibrous, transparent
portion of the cornea known as the stroma)
Ocular Anti-inflammatory Drugs
NSAIDs
o ketorolac (Acular)
o flurbiprofen (Ocufen)
o bromfenac (Xibrom)
o diclofenac (Voltaren)
Corticosteroids
o dexamethasone (Decadron, AK-Dex)
o fluocinonide (Retisert)o fluorometholone (Fluor-Op)
o loteprednol (Lotemax)
o medrysone (HMS)
o prednisolone (Pred Forte)
o rimexolone (Vexol)
Act on various parts of the arachidonic acid metabolic pathway
Reduce the production of various inflammatory mediators
As a result, pain, erythema, and other inflammatory processes are reduced
Used prophylactically after surgery to prevent inflammation and scarring
NSAIDs used for symptomatic treatment of seasonal allergic conjunctivitis
Topical Ophthalmic Anesthetics
tetracaine
proparacaine (Alcaine)
Used to prevent eye pain during
o Surgery
o Ophthalmic examinations
o Removal of foreign bodies or sutures
o Diagnostic testing and procedures
Short-term use only
Not for self-administration
Ophthalmic Diagnostic Drugs
Cycloplegic mydratics
atropine sulfate (Isopto Atropine)
o Results in
Mydriasis
Cycloplegia
o Used for
Ophthalmic examinations
Uveitis (which benefits from pupillary dilation)
Cycloplegic mydratics (cont’d)
cyclopentolate (Cyclogyl)
o Causes mydriasis and cycloplegia
o Used for diagnostic examinations
o Not used for uveitis
Other cycloplegic mydriatics
o scopolamine (Isopto Hyoscine)
o homatropine (Isopto Homatropine)
o tropicamide (Mydriacyl)
Ophthalmic dye
o fluorescein (AK-Fluor)
Diagnostic dye used to identify corneal defects and to locate foreign
objects in the eye
Used in fitting hard contact lenses Various defects are highlighted in either bright green or yellow-orange,
and foreign objects have a green halo around them
Ophthalmic Antiallergic Drugs
Ophthalmic antihistamines
o Used to treat symptoms of allergic conjunctivitis (“hay fever”)
o azelastine (Optivar)
o olopatadine (Patanol)
o emedastine (Emadine)
o ketotifen (Zaditor)
o epinastine (Elestat)
Used for seasonal allergy symptoms
o Mast cell stabilizers
cromolyn sodium (Crolom)
pemirolast (Alamast)
nedocromil (Alocril)
lodoxamide (Alomide)
o Decongestants
Tetrahydrolozine (Visine)
phenylephrine (Neo-Synephrine)
oxymetazoline (Visine LR)
naphazoline (Clear Eyes)
Ophthalmic Lubricants and Moisturizers
Artificial tears
o Over-the-counter products
o Provide lubrication or moisture for dry or irritated eyes
o Available in drops or ointment
o Brand names include: Murine, Nu-Tears, Moisture Drops, Tears Plus, Akwa Tears
Restasis
o Ophthalmic form of cyclosporine
o Immunosuppressant drug
o Used to treat keratoconjunctivitis sicca (dry eyes)
o It can be used together with artificial tears, if the drugs are given 15 minutes
apart
Nursing Implications
Assess the patient’s history, including medication history
Assess patient’s baseline vital signs and visual acuity, and perform a physical assessment
of the eye and surrounding structures
Assess for contraindications to specific drugs
Follow specific guidelines for administration of ophthalmic drugs
Avoid touching the eye with the tip of the dropper or container
Apply ointments as a thin layer in the conjunctival sac
When applying eyedrops, have the patient look up to the ceiling, and place the drop in
the conjunctival sac Pressure may be applied to the inner canthus for at least 1 minute to reduce systemic
absorption of the drug
If more than one eye medication is ordered, clarify the correct order and intervals for
administration
If the patient wears contact lenses, check to see if they should be removed during
therapy with eye medications
Provide patient/family education on correct procedures for administration of eye
medications
Monitor for adverse effects
Monitor for therapeutic response to therapy
Otic Drugs
Structure of the Ear
Ear Disorders
Bacterial and fungal infections
Inflammatory disorders that cause pain
Earwax accumulation
External ear: physical trauma, dermatitis
Middle ear: otitis media
o Most often afflicts children, following a respiratory tract infection
o In adults usually results from foreign objects or water sportso Symptoms include pain, fever, malaise, pressure, sensation of fullness in the
ears, hearing loss
o If untreated, tinnitus, nausea,
vertigo, mastoiditis may occur
o Hearing deficits and hearing loss
may result if prompt therapy not
started
Otic Drugs for External and Middle Ear Disorders
Antibiotics
Antifungals
Antiinflammatory drugs
Local analgesics
Local anesthetics
Steroids
Wax emulsifiers
Antibacterial and Antifungal Otic Drugs
Topical formulations applied to the
external ear
Often combined with steroids for antiinflammatory, antipruritic, and antiallergic drug
effects
Middle ear infections generally require systemically administered antibiotics
Antibiotics
o neomycin and polymyxin B plus hydrocortisone combination (Cortisporin Otic)
o Others containing ciprofloxacin and dexamethasone (Ciprodex)
o Fluroquinolone: Ofloxacin
Antifungals
o Cortic (combination of antifungal drugs and hydrocortisone)
o Acetasol HC (hydrocortisone, local anesthetic, antiseptic, antifungal, emulsifier,
and antiseptic preservative)
Wax Emulsifiers
carbamide peroxide (Debrox)
Combined with other drugs, such as glycerin, to work together to loosen and help
remove cerumen
Ear canal irrigation with water may be required
Other names include: Debrox Drops, Murine Ear Drops, Auro Ear Drops
Nursing Implications
Assess baseline hearing or auditory status
Evaluate patient’s symptoms
Assess drug and food allergies
Assess for contraindications
Perforated eardrum(s) may be a contraindication to these drugs
o ciprofloxacin and ofloxacin can be used with perforated ear drums
If necessary or if ordered, remove cerumen before instilling ear drops by irrigation Cleanse outer ear thoroughly
Ear drops should be warmed to approximately body temperature before instillation
Allow refrigerated solutions to warm to room temperature.
Cold solutions may cause vomiting and dizziness
For adults, drops should be given while holding the pinna up and back
For children younger than 3 years, hold the pinna down and back when giving ear drops
Allow the drops time to flow down into the ear canal
Patients should lie on the side opposite to the side of the affected ear for about 5
minutes after instillation of the drug
A small cotton ball may be gently inserted into the ear canal to keep the drug in, but do
not force the cotton into the ear canal
Gently massage the tragus of the ear to encourage flow of medication
[Show More]
.png)





.png)




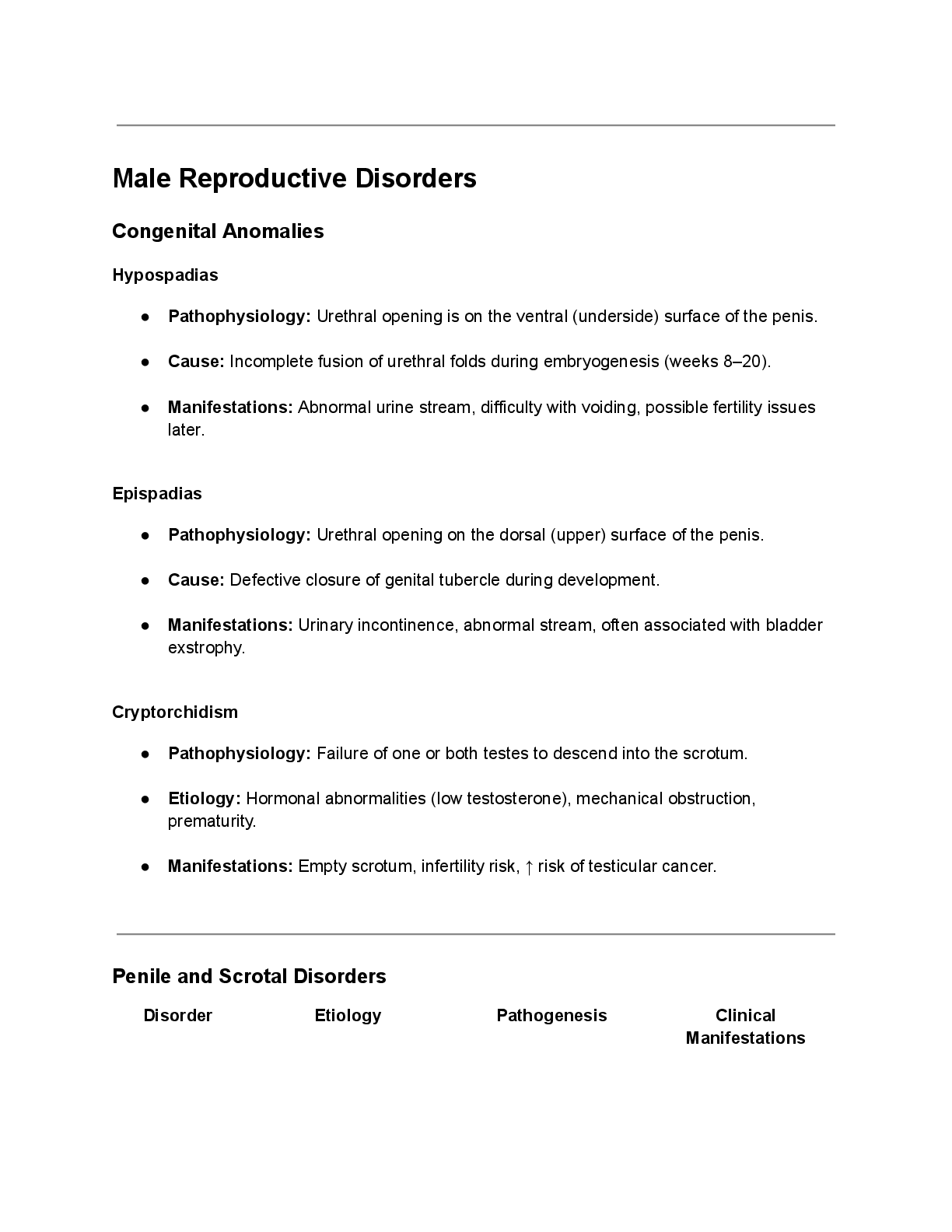
![Preview of eBook [PDF] Barash, Cullen, and Stoelting's Clinical Anesthesia 9th Edition By Bruce F. Cu](https://browseimages.nyc3.digitaloceanspaces.com/paper-images/2024/Aug/29/8DF2QRTq2024-08-29-10-3966d0259b7c4b5.png)
![Preview of eBook [PDF] Burns' Pediatric Primary Care 7th Edition BY Dawn Lee Garzon Maaks,, Nancy Bar](https://browseimages.nyc3.digitaloceanspaces.com/paper-images/2024/Aug/26/WR2rowXX2024-08-26-02-0966cc625bea839.png)

![Preview of eBook [PDF] AACN Essentials of Progressive Care Nursing 5th Edition By Sarah A. Delgado](https://browseimages.nyc3.digitaloceanspaces.com/paper-images/2024/Aug/29/ipbdJSTN2024-08-29-11-1466d02df30fc96.png)
![Preview of eBook [PDF] AACN Essentials of Progressive Care Nursing 5th Edition By Sarah Delgado](https://browseimages.nyc3.digitaloceanspaces.com/paper-images/2025/Aug/06/lAjhFV4A2025-08-06-09-286892f5fd83090.png)