Pearson Edexcel Level 3 GCE Business Advanced PAPER 3: Investigating business in a competitive environment QUESTION PAPER 2022
Pharmacology > STUDY GUIDE > Pharmacology Study Guides For Exam 1-4 with better layout and a final exam blueprint (All)
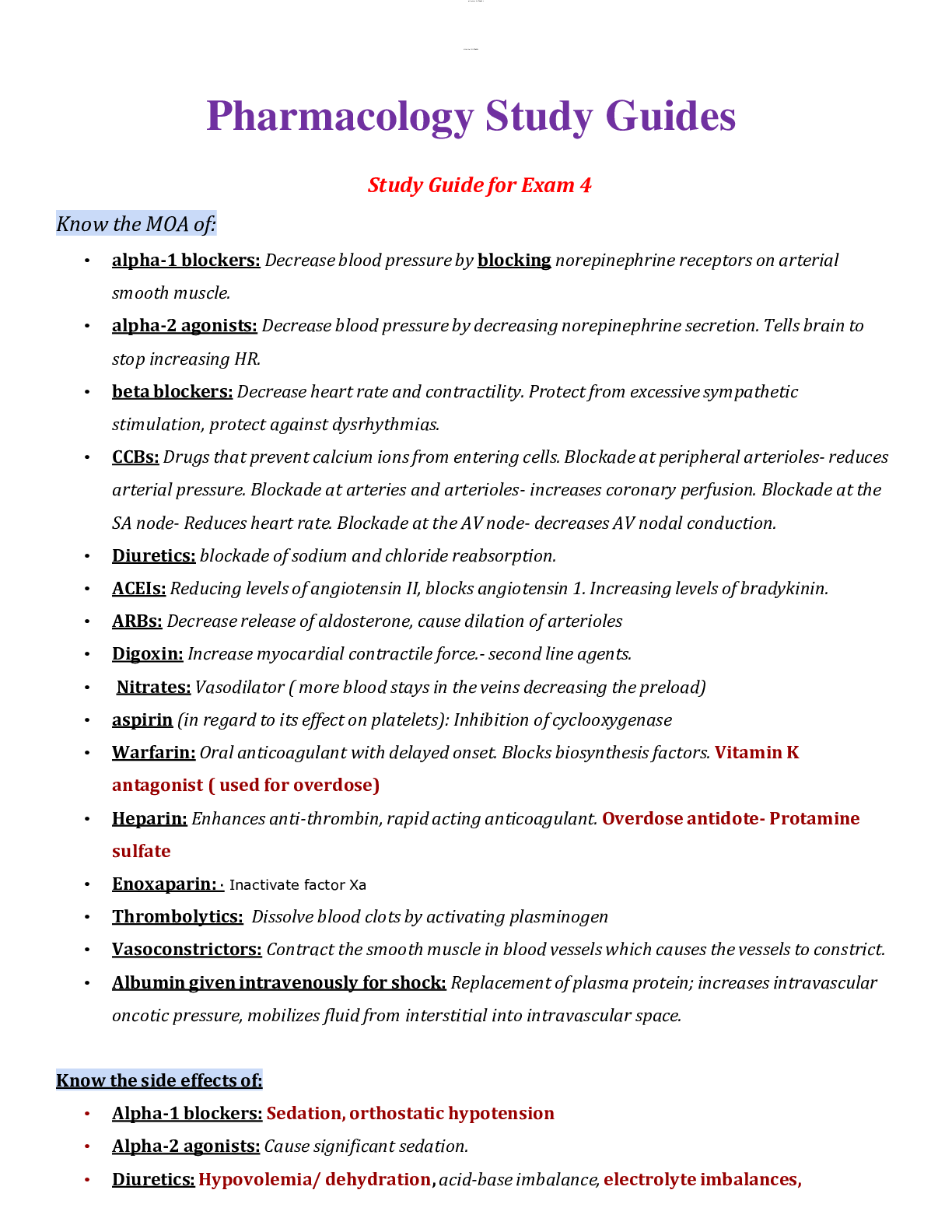
Pharmacology Study Guides Study Guide for Exam 4 Know the MOA of: • alpha-1 blockers: Decrease blood pressure by blocking norepinephrine receptors on arterial smooth muscle. • alpha-2 agonist ... s: Decrease blood pressure by decreasing norepinephrine secretion. Tells brain to stop increasing HR. • beta blockers: Decrease heart rate and contractility. Protect from excessive sympathetic stimulation, protect against dysrhythmias. • CCBs: Drugs that prevent calcium ions from entering cells. Blockade at peripheral arterioles- reduces arterial pressure. Blockade at arteries and arterioles- increases coronary perfusion. Blockade at the SA node- Reduces heart rate. Blockade at the AV node- decreases AV nodal conduction. • Diuretics: blockade of sodium and chloride reabsorption. • ACEIs: Reducing levels of angiotensin II, blocks angiotensin 1. Increasing levels of bradykinin. • ARBs: Decrease release of aldosterone, cause dilation of arterioles • Digoxin: Increase myocardial contractile force.- second line agents. • Nitrates: Vasodilator ( more blood stays in the veins decreasing the preload) • aspirin (in regard to its effect on platelets): Inhibition of cyclooxygenase • Warfarin: Oral anticoagulant with delayed onset. Blocks biosynthesis factors. Vitamin K antagonist ( used for overdose) • Heparin: Enhances anti-thrombin, rapid acting anticoagulant. Overdose antidote- Protamine sulfate • Enoxaparin: · Inactivate factor Xa • Thrombolytics: Dissolve blood clots by activating plasminogen • Vasoconstrictors: Contract the smooth muscle in blood vessels which causes the vessels to constrict. • Albumin given intravenously for shock: Replacement of plasma protein; increases intravascular oncotic pressure, mobilizes fluid from interstitial into intravascular space. Know the side effects of: • Alpha-1 blockers: Sedation, orthostatic hypotension • Alpha-2 agonists: Cause significant sedation. • Diuretics: Hypovolemia/ dehydration, acid-base imbalance, electrolyte imbalances,lOMoAR cPSD|784381 Hypokalemia. Hyperkalemia, K+ sparing • beta blockers: Fluid retention or worsening of HF, fatigue(exercise tol.), hypotension, bradycardia or heart block, can’t detect hypoglycemia, bronchospasm if non-selective. • ACEIs/ARBs (including which of the 2 classes can cause cough or angioedema): First done hypotension, fetal injury, cough( ace cause cough and ARBS do not) angioedema, hyperkalemia, rash, renal failure, neutropenia. • CCBs (and how to manage those side effects): Constipation: can be decreased by increasing dietary fiber and fluids. Dizziness, Edema, Gingival hyperplasia, Heart block. • Vasodilators: hypotension, resultant reflex tachycardia. • short-acting and long-acting nitrates: Headache, orthostatic hypotension, reflex tachycardia. • Aspirin: Increases of GI bleed. • Heparin: Hemorrhage, Heparin- induced thrombocytopenia, hypersensitivity reactions. • Warfarin: Hemorrhage ( vitamin K for toxicity) Fetal hemorrhage ( for use during pregnancy) • Thrombolytics: bleeding ( minor oozing to life-threatening amount) • Digoxin: Hypokalemia (may increase toxicity), Narrow Therapeutic Range that can lead to toxicity→ s/sx: blurred vision, halos around light, yellow fields. Contraindications • beta blockers: Hypersensitivity; Uncompensated HF; Pulmonary edema; Cardiogenic shock; Bradycardia, sick sinus syndrome, or heart block, low BP, asthma. • CCBs: Prevents calcium ions from entering cells of smooth muscles and myocardium. • ACEIs/ARBs: o Drug interactions: Diuretics, antihypertensive agents, drugs that raise potassium levels, lithium. • Diuretics: Digoxin, other ototoxic drugs, potassium-sparing diuretics, lithium, antihypertensive agents, nonsteroidal, anti-inflammatory drugs. • Amiodarone: • Anticoagulants: Drugs that increase anticoagulant effects, drugs that promote bleeding, drugs that decrease anticoagulant effects, heparin, aspirin, acetaminophen. • Thrombolytics: “clot buster”--breaks up clots in lungs, etc. (warfarin is anticoagulant that prevents the formation. Two different things!) • vasoconstrictors: • Why are beta blockers avoided with those with type 1 diabetes? o A sign of low blood sugar is tachycardialOMoAR cPSD|784381 o Beta-blockers slow the heartbeat o Won’t recognize blood sugar is low • What can happen if a beta blocker is stopped abruptly? o Abrupt withdrawal may precipitate life-threatening arrhythmias, hypertension, or myocardial ischemia. o Withdrawal symptoms, increase BP, recurrence of angina pains o Sensation of rapid, irregular of forceful heartbeats (palpitations) What type of drug is • Spironolactone – drug for HTN / K+ sparing agents diuretic (aldosterone antagonists) • Chlorothiazide – drug for HTN / Thiazide • Furosemide – drug for HTN / Loop Diuretic • Verapamil – drug for HTN / Calcium Channel Blocker • Hydrochlorothiazide - drug for HTN / Thiazide • Hydralazine – drug used for HF / Vasodilator • Atenolol - drug for HTN / Beta Blocker • Metoprolol - drug for HTN / Beta Blocker • Propranolol - drug for HTN / Beta Blocker • Captopril - drug for HTN / ACE Inhibitor • Amiodarone – Drugs for dysrhythmias / Potassium Channel Blocker • Procainamide - Drugs for dysrhythmias / Sodium Channel Blocker • Lidocaine - antiarrhythmic • Enoxaparin – Anticoagulant / Heparin • Heparin - Anticoagulant / Heparin • Aspirin - antiplatelet • Clopidogrel - Anticoagulant / antiplatelet • Reteplase - anticoagulant / Thrombolytics • Alteplase - anticoagulant / Thrombolytics • Streptokinase - anticoagulant / Thrombolytics • Isoproterenol - Isuprel (non-selective beta-agonist What lab test is used to monitor the effectiveness of warfarin, heparin? - Heparin = aPTT - Warfarin = INR/PT What is the pregnancy category of ACEIs/ARBs, and warfarin? Are contraindicated during pregnancy.lOMoAR cPSD|784381 o Pregnancy Category D What group of antihypertensive meds can increase lipids, the blood sugar and the uric acid level? o Diazoxide ( hyperstat IV) Which class of diuretics produces the greatest diuresis? • Loop diuretics Which diuretic classes are potassium sparing and which are not? • Spironolactone( aldactone) - potassium sparing • Triamterene - potassium sparing. Why are antiarrhythmics not being used as often as they used to be? • Can create new dysrhythmias and worsen existing ones. Increase the risk of death and nonpharmacologic therapies have begun to replace drugs as the preferred treatment for many dysrhythmia types (p. 534) What type of arrhythmias are treated with beta blockers, digoxin, lidocaine, amiodarone? • Beta blocker o Atrial fibrillation, Sustained supraventricular tachycardia (SVT), Premature Ventricular Complexes (PVCs), Supraventricular tachydysrhythmias, • Digoxin o Atrial fibrillation, Atrial flutter, supraventricular dysrhythmias, • Lidocaine o Sustained Ventricular Tachycardia (SVT), Ventricular Fibrillation, Digoxin-induced Ventricular Dysrhythmias, • Amiodarone o Atrial flutter, Sustained supraventricular tachycardia (SVT), Ventricular Fibrillation, Torsades de Pointes Why should antiarrhythmics never be stopped abruptly? • Serious changes in heart function Which IV solution would be used for a patient with an isotonic volume contraction? • Fluids that are isotonic to plasma. 0.9% NS How would you assess for fluid overload in a patient receiving IV fluids? • Respiratory assessment (adventitious lung sounds)lOMoAR cPSD|784381 • Electrolyte balance • Edema What are the s/sx of digoxin toxicity? (hypokalemia increases susceptibility of digoxin toxicity) o Confusion o Bradycardia o AV SA block o Loss of appetite o Palpitations o Decreased urine output. o Yellow halos around light What drugs are used to treat heart failure that is not severe, but stopped if the heart failure becomes decompensated? o Diuretics o RAAS inhibitors o Beta blockers o Digoxin What systolic blood pressure or diastolic reading should lead you to hold an antihypertensive? • Low BP, but also depends on the patient's usual BP readings What pulse reading should lead you to hold digoxin or a beta blocker? • Less than 60 bpm What is a positive of inotropic agent? • Increased cardiac output. How do ACEIs and ARBs decrease aldosterone secretion? • Decrease aldosterone and thus decreases blood volume thereby decreasing the heart workload. Why is transdermal nitroglycerin only left on for ½ the day? • The rate of release is constant and, depending on the patch used, can range from 0.1 to 0.8 mg/hr. Effects begin within 30 to 60 minutes and persist as long as the patch remains in place (up to 14 hours). Patches are applied once daily to a hairless area of skin. The site should be rotated to avoid local irritation. Tolerance develops if patches are used continuously (24 hours a day every day). Accordingly, a dailylOMoAR cPSD|784381 “patch-free” interval of 10 to 12 hours is recommended. This can be accomplished by applying a new patch each morning, leaving it in place for 12 to 14 hours, and then removing it in the evening. How do beta blockers and CCBs decrease oxygen use by the heart? • Beta blockers decrease oxygen demand by decreasing heart rate and contractility. • Calcium channel blockers- decrease oxygen demand by dilating arterioles, which decreases afterload, and by decreasing heart rate and contractility. What instructions should be given to someone about taking SL NTG? • Place under tongue and let dissolve. Take up to 3, wait 5 min after, then take another if indicated by doc, up to 3. What is the usual practice for changing a patient from parenteral to oral anticoagulants? • What instructions should be given to a patient about the storage and frequency of use of NTG sublingual for angina? • According to the current guidelines, patients with ongoing ischemic discomfort should be given sublingual nitroglycerin (0.4 mg) every 5 minutes for a total of three doses, and then be assessed to determine whether IV nitroglycerin should be given. What is the primary way that medications decrease angina pain and also help relieve HF? • By decreasing oxygen demand. What foods/fluids must be avoided when a patient is on warfarin, or a Calcium channel blocker? • Food that high in vitamin K. Spinach, mustard greens, collards, grapefruit juice, 3Gs - garlic, ginseng, ginkgo biloba. What are the s/sx of orthostatic hypotension? • Blurry vision, dizziness, light headed, weakness, fainting, confusion, nausea. Anaphylaxis? • Skin rashes and itching and hives, swelling of lips tongue or throat, SOB and wheezing, dizziness and or fainting, stomach pain, vomiting or diarrhea. What is the basic treatment for the latter. •lOMoAR cPSD|784381 How can fainting due to orthostatic hypotension be prevented? • Taking time to move from each position. What are the advantages of combination antihypertensives? • Combined with beta blocker to protect against reflex tachycardia and diuretics to prevent sodium and water retention and expansion of blood volume. What drugs, etc. absolutely cannot be taken when a patient uses nitrates? • Viagra Why are thiazide diuretics and digoxin a potentially dangerous combination? • Thiazide diuretics are known to induce hypokalemia, which increases digoxin toxicity (digoxin competes with K+ for the external K+ binding site on the Na+/K+ ATPase, so any reduction in plasma K+ levels makes it easier for digoxin to bind so increases its effect). Know these drug names and drug classes Drugs for HTN 1. Thiazide and thiazide-like agents (don't spare K+) hydrochlorothiazide (HCTZ) 2. K+-sparing agents diuretics (Aldosterone antagonists) spironolactone (Aldactone) 3. Loop diuretics furosemide (Lasix) 4. Calcium Channel Blockers NEGATIVE INOTROPIC a) Selective (for arteries) amlodipine (Norvasc) b) Non-selective (works on arteries and the heart) diltiazem (Cardizem) 5. ACE Inhibitors (ACEIs) a) enalapril (Vasotec) b) lisinopril (Zestril) 6. Angiotensin II receptor blockers losartan (Cozaar) 7. Alpha-1 adrenergic antagonists terazosin (Hytrin)lOMoAR cPSD|784381 8. Alpha-2 Adrenergic agonists clonidine (Catapres) 9. Beta-adrenergic antagonists (Beta blockers)NEGATIVE INOTROPIC a) atenolol (Tenorim) (selective) b) metoprolol (Toprol, Lopressor) (selective) c) propranolol (Inderal) (non-selective) Drugs used to treat HF A. Cardiac glycoside; also classified as a positive inotropic, antiarrhythmic for atrial fibrillation digoxin (Lanoxin) B. Vasodilators hydralazine (Apresoline) Drugs for CAD/Angina and MI A. Organic Nitrates 1. isosorbide dinitrate (Isordil) 2. nitroglycerin (Nitrostat, Nitro-Dur, Nitro-Bid) also classified as a positive inotropic Drugs for dysrhythmias A. Sodium channel blockers procainamide HCl (Procan) (Class 1A) B. Beta blockers are class 2 antidysrhythmic drugs C. Potassium Channel blockers amiodarone (Cordarone) D. Calcium channel blockers are Class IV antidysrhythmics Anticoagulants-more bruises/prone to bleeding A. Heparins-(makes blood less viscous) 1. heparin (Heplock) 2. enoxaparin (Lovenox) 3. warfarin (Coumadin) B. Antiplatelet agents-((prevents platelets from sticking together)) clopidogrel (Plavix)lOMoAR cPSD|784381 C. Thrombolytics 1. alteplase (Activase) 2. retaplase (Retavase) Drugs used for Shock A. Vasoconstrictors/Vasopressors phenylephrine (Neo-Synephrine) B. Inotropic drugs for shock 1. dobutamine (Dobutrex) 2. dopamine (Intropin)lOMoAR cPSD|784381 Pharmacology Exam 3 Study Guide Know the s/sx of and what neurotransmitter alterations are believed to exist with each: • Anxiety disorder o S/Sx: Symptoms include stress that's out of proportion to the impact of the event, inability to set aside a worry, and restlessness. o Neurotransmitter alterations: GABA (Gamma-Aminobutyric Acid) • Depression o S/Sx: The persistent feeling of sadness or loss of interest that characterizes major depression can lead to a range of behavioral and physical symptoms. These may include changes in sleep, appetite, energy level, concentration, daily behavior, or self-esteem. Depression can also be associated with thoughts of suicide. o Neurotransmitter alterations: depletion of the neurotransmitters serotonin, norepinephrine or dopamine in the central nervous system. Serotonin is the most extensively studied neurotransmitter in depression. • Bipolar disorder o S/Sx: Manic episodes may include symptoms such as high energy, reduced need for sleep, and loss of touch with reality. Depressive episodes may include symptoms such as low energy, low motivation, and loss of interest in daily activities. Mood episodes last days to months at a time and may also be associated with suicidal thoughts. o Neurotransmitter alterations: alterations of excitatory neurotransmitters (dopamine, serotonin, noradrenaline, acetylcholine), glutamate and GABA (a presynaptic inhibitory neurotransmitter) • Psychosis o S/Sx: Possible symptoms include delusions, hallucinations, talking incoherently, and agitation. The person with the condition usually isn't aware of his or her behavior. o Neurotransmitter alterations: Dopamine Know the basic pathophysiology and s/sx of Parkinson’s and Alzheimer’s Disease: • Parkinson’s: o Pathophysiology: Degeneration of dopamine neurons is particularly evident in a part of the substantia nigra called the pars compacta. Significantly, the loss of dopamine in the pars compacta increases the overall excitatory drive in the basal ganglia,* disrupting voluntary motor control and causing the characteristic symptoms of PD. o S/Sx: Tremor, slowed movements, rigid muscles, impaired posture or balance, loss of automatic movements, speech changes, writing changes • Alzheimer’s: o Pathophysiology: AD's core neuropathologic findings include extracellular amyloid plaques, intracellular NFTs, synaptic deterioration, and neuronal death.1 Granulovacuolar degeneration inlOMoAR cPSD|784381 the hippocampus and amyloid deposition in blood vessels (congophilic angiopathy) may also be seen on tissue examination, but are not required for the diagnosis o S/Sx: mental decline, difficulty thinking and understanding, confusion in the evening hours, delusion, disorientation, forgetfulness, making things up, mental confusion, difficulty concentrating, inability to create new memories, inability to do simple math, or inability to recognize common things Know all the terms used to classify medications that work primarily on the ANS and the effects of the categories drugs *if you block one system you get the effects of the opposite system*:::::::::::::::::::::::::::::::::::::MORE CONTENT IN THE ATTACHMENT::::::::::::::::::::::::::::: [Show More]
Last updated: 1 year ago
Preview 6 out of 53 pages

Loading document previews ...
Buy this document to get the full access instantly
Instant Download Access after purchase
Buy NowInstant download
We Accept:

Can't find what you want? Try our AI powered Search
Connected school, study & course
About the document
Uploaded On
May 30, 2021
Number of pages
53
Written in
All
This document has been written for:
Uploaded
May 30, 2021
Downloads
0
Views
246
Scholarfriends.com Online Platform by Browsegrades Inc. 651N South Broad St, Middletown DE. United States.
We're available through e-mail, Twitter, Facebook, and live chat.
FAQ
Questions? Leave a message!
Copyright © Scholarfriends · High quality services·

.png)