Week 5
Identify the population most commonly affected by bacterial prostatitis: Acute bacterial
prostatitis occurs predominantly in sexually active men between the ages of 30 and 50 years old,
whereas chronic bacteria
...
Week 5
Identify the population most commonly affected by bacterial prostatitis: Acute bacterial
prostatitis occurs predominantly in sexually active men between the ages of 30 and 50 years old,
whereas chronic bacterial prostatitis is most common in men older than 50.
Prostatitis (Acute, chronic, nonbacterial)
Risk factors
Age> 50 yrs, Hx of prostate calculi, BPH, prev. UTI, recurrent UTIS
acute and chronic-> strep. Faecalis and staph. Aureus are most common
physical exam: abd. Exam to detect distended bladder, costovertebral angle tenderness, genital
exam, digital rectal exam
acute: warm, tense, swollen, boggy and very tender prostate vs chronic: normal or little boggy
diagnostic testing: U/A (PYURIA + for all three), midstream urine cand s, 츛, urethral swab for
GC AND CT, cystoscopy, transrectal ult
Acute-- treatment
14 to 28 day regimen-cipro 500 mg q 12 hr, levofloxacin 500mg daily or doxycycline or TMPSMX
STD coverage for ABP; single dose IM ceftriaxone 250 mg + single dose azithromycine or doXy
100 mg BID 7 D
Supportive measure: antipyretics, nsaids, hydration, stool softeners
Chronic-treatment
5 to 12 week antibiotic course with same meds + alpha-blocking agents to relax the smooth
muscles around prostate
Nonbacterial prostatitis- treatmentFEFER TO UROLOGIST
Discuss the physical exam characteristics of acute bacterial prostatitis: urinary complains
(frequency, urgency, nocturia, dysuria) pain & discomfort (LBP, penile, scrotal pain, fever, chills,
malaise or painful ejaculation, arthralgia, myalgia)
Chronic bacterial s/s: symptoms often absent, perineal pain, LBP, lower abd. Pain, scrotal or
penile pain, pain with ejaculation, dysuria…
Discuss how the Phren sign can differentiate between testicular torsion and epididymitis:
The most common symptom in testicular torsion is sudden, severe pain accompanied by swelling
of the affected testis. The patient may have pain for several days without seeking medical
attention. The most common finding on clinical exam is the absence of the cremasteric reflex and
unlike in epididymitis, elevation of the affected testis does not relieve the pain (negative Phren’s
sign).
Epididymitis
Can affect any age in male, Hx of unprotected intercourse, a new sexual partner, Hx of UTI or
urinary discharge
Symptoms
Unilateral scroll pain which radiates along the spermatic cord or to the flank
HALLMARK SYMPTOM: RELIEF OF DISCOMFORT WITH ELEVATION OF TESTIS
AND EPIDIDYMIS
Tx: same antibiotics ceftriaxone 250mg IM TIMES 1 and azythromycine 1 gm po times 1
BPH
Most common condition in males > 40 yrs
Risk factors: ?
Size does not correlated with severity of symptoms
BPH= smooth and enlarged, if hard, suspect cancerTreatment
Avoid caffeine and alcohol
Conservative tx vs surgery
Alpha blockers (relax smooth muscle)Tamsulosine 0.4-0.8mg qd, doxazosin 4-8 mg qd
5-alpha-reductade inhibitors finasteride 5mg qd or dutasteride 0.5 mg qd
Testicular torsion- twisting or rotation of the testes around the spermatic cord, blocking blood to
the testes UROLOGICAL EMERGENCY!! (> 6 hrs, viability 10-15%, >24 hrs, below 10%)
Sx: mostly seen in adolescent and young adults; trauma, exercise, extreme cold,
absence of the cremasteric reflex, unlike in epididymitis, elevation of the affected testis does
NOT relieve pain (Phrens’s sign)
Discuss common symptoms reported from a patient with BPH:
Obstructive symptoms include
decreased stream
hesitancy
postvoid dribbling
sensation of incomplete bladder emptying
overflow incontinence
inability to voluntarily stop the urine stream
urinary retention
straining
Irritative symptoms include
nocturia
urinary frequency
urinary urgency
dysuria
urge incontinence
Discuss the hallmark characteristic of a varicocele: Sensation that the testes feel like a “bag of
wormsVaricocele (varicosvein of testes): abnormal degree of venous dilation in the vasculature above
the testes, due to weak walls and vascular engorgement of spermatic cord
Almost always unilateral, left side due to anatomy, venous engorgement with valsalva maneuver
Hydrocele: collection of peritoneal fluid within the scrotum between the 2 layered sac that holds
the testes and spermatic cord- most occur in mals> 40 yrs
Swelling in scrotum or inguinal canal
Painless or sense of heaviness
Transilumination- in dark room, use a penlight- light pink (r/o hematoma as well)
Inguino-scrotal ultrasound to r/o inguinal hernia if hydrocele cannot be distinguished by PE
No treatment
Identify the population most affected by testicular cancer: Most common cancer in American
males between the ages of 15 and 35
Testicular cancer
Risk factors: HIV infection, Caucasian race, cryptorchidism
Clinical presentation: painless lump in one of testicle, feeling of heaviness in the affected
scrotum, 10% are asymptomatic, firm, non-tender mass distinct from the spermatic cord
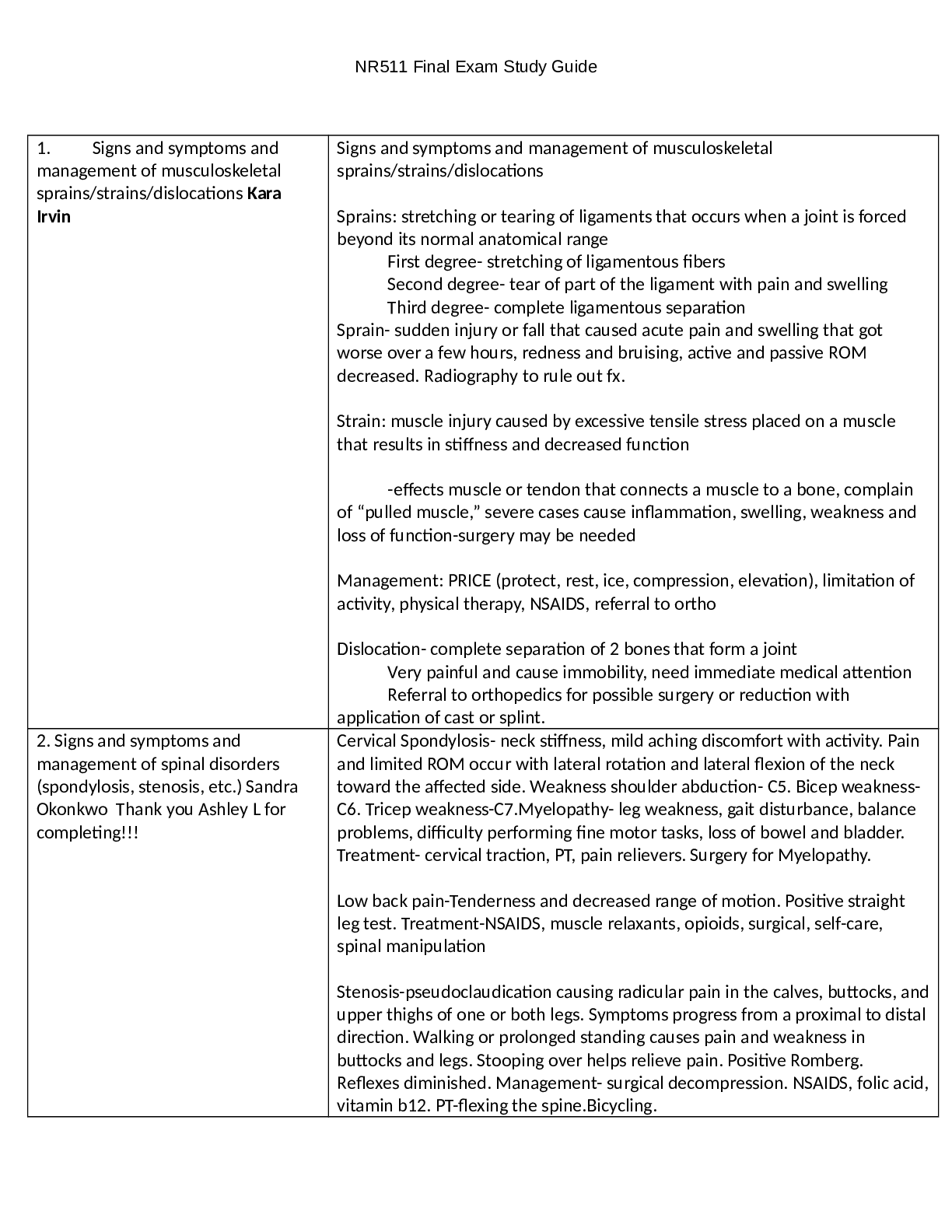
Explain spinal stenosis: Spinal stenosis is caused by a narrowing of the spinal canal as a result
of degeneration of the bony facet joints and the intervertebral disks.
Discuss common characteristics (subjective and objective findings) of patients with lumbar
spinal stenosis: Leg pain is commonly greater than back pain and pain is characteristically
worse with prolonged standing or walking and improved by rest. In more advanced cases, leg
pain with weakness or numbness and tingling can be present. Patients with cervical stenosis
usually present with cervical radiculopathy, with or without myelopathy.
Identify the red flags associated with back and neck complaints which warrant further
investigation: Any evidence of neurological deficit
Define chronic pain: Longer than 3 months
Identify the number of joints involved in a poly-articular disorder:
Erythema
Warmth Pain
Swelling
Describe the four cardinal signs of joint inflammation
Differentiate between DeQuervain’s Tenosynovitis and Carpal Tunnel Syndrome: DT is
inflammation of tendons on the side of the wrist at the base of the thumb. CTS is a numbness and
tingling in the hand and arm caused by a pinched nerve in the wrist.
Differentiate between lateral and medial epicondylitis:
Medial epicondylitis (Golfer’s Elbow)
Pain is often sharp in the medial epicondyle and radiates down the arm from the inside of the
elbow. Pain occurs upon extension of the wrist or supination of the forearm such as when
gripping, twisting, or flexing at the wrist. There may be weakness in the hand or wrist as well or
numbness and tingling in the ring and little fingers. The difference between the two is based on
location of the pain.
Lateral epicondylitis (Tennis Elbow)
Pain is often sharp in the lateral epicondyle and radiates from the outside of the elbow and down
the forearm. Pain occurs upon extension of the wrist or supination of the forearm such as when
gripping and twisting. There may be weakness in the forearm or a weak grip.
Discuss at least 3 vital body functions which thyroid hormones regulate
Breathing
Heart rate
Central and peripheral nervous systems
Body weight
Muscle strength
Menstrual cycles
Body temperature
Cholesterol levels
Describe a goiter and the type of thyroid dysfunction that can be associated with:
insufficient iodine, the thyroid enlarges but thyroid hormone remains low. Hashimoto’s
thyroiditis, Graves’ disease, and thyroid nodules. Worldwide, the most common cause of goiter is
iodine deficiency due to diet deficiency.
Differentiate between overt hypothyroidism and subclinical hypothyroidism:Overt hypothyroidism—TSH above 10 and FT4 is decreased; this makes sense due to the normal
physiology of the hypothalamus-pituitary-thyroid axis. Too little hormone is being produced, and
the pituitary is attempting to get the thyroid to produce more (low FT4 and high TSH).
Subclinical hypothyroidism—In subclinical thyroidism, TSH levels are above normal, but the
FT4 is within range. Frequently, patients with subclinical hypothyroidism exhibit some
symptoms whereas others may not.
Treatment for hypothyroidism
Levothyroxine dosing- two options (1.6 mcg/kg base on ideal wt or TSH range 4-8; 25mcg, 8-
12; 50 mcg, >12; 75mcg.
Retest TSH q 6 to 8 weesk until target achicvd then retest 1 6 to 12 months
Hypothyroidism and pregnancy
First trimester: 0.45-2.5
Second: <3.0
Third: <3.5
Refere to endo
Tsh unstable infertility, cardiac disease, infants and children with thyroid disorder
Hyperthyroidism
TSH low, FT4 and antibodies normal
Overt: TSH low/ undetectable, increased FT4 AND t4
Graves dz-autoimmune (most common)
Subacute thyroiditis-post viral syndrome
Toxic multinodular goidter
Toxic adenoma
Treatment of hyperthyroidism
Radioactive iodine, anti-thyroid drugs- get baseline CBC and LFTs, thyroidectomyThyroid nodules
s/s: difficulty swallowing, chocking sensation with eating and drinking, voice changes
nodules >1cm refere to ENT to check if cancer
risk factors: males, pt with graves disease, children<20 yrs or elderly >70 yrs
[Show More]