NUR 2063 Exam 3 Focused Review Already Graded A+
Document Content and Description Below
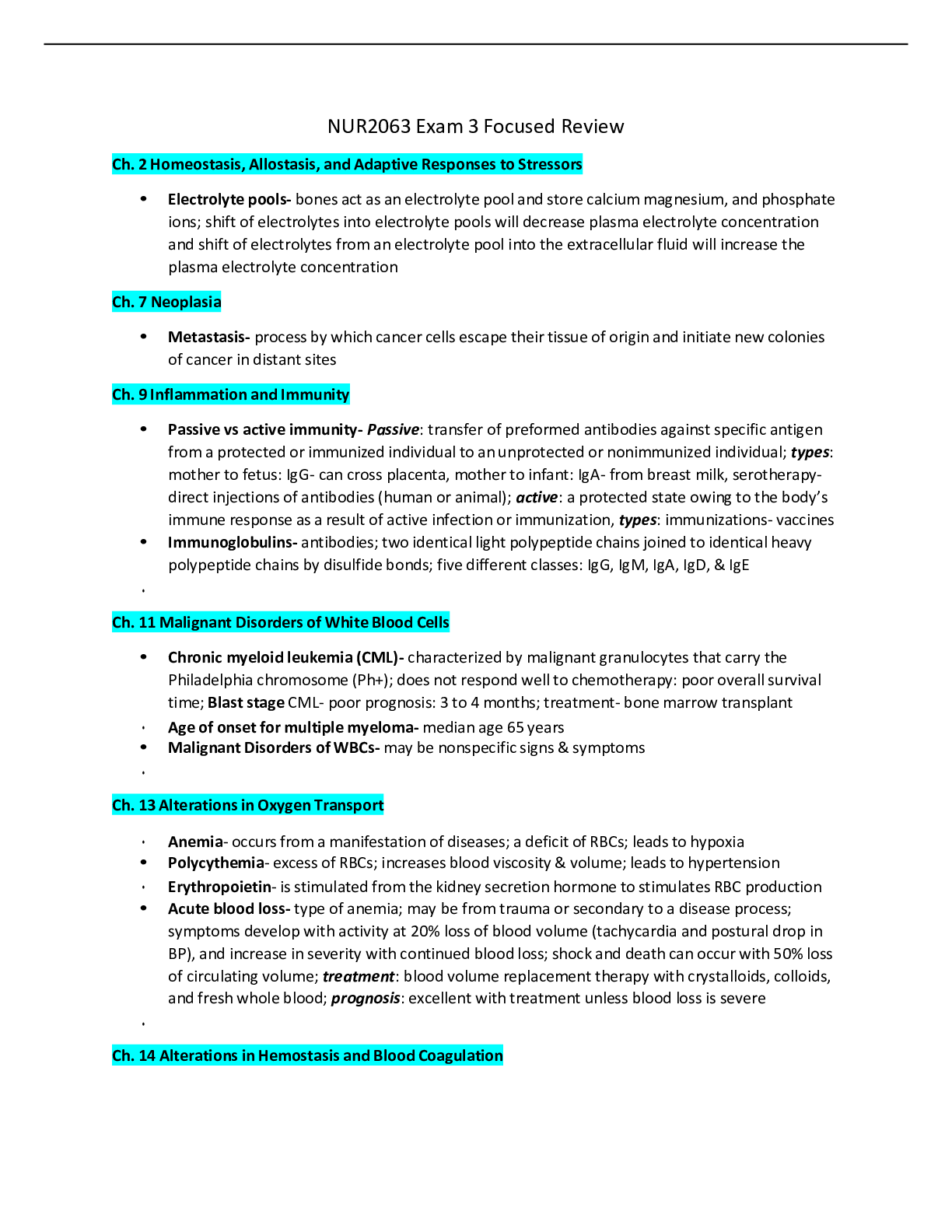
NUR2063 Exam 3 Focused Review Ch. 2 Homeostasis, Allostasis, and Adaptive Responses to Stressors • Electrolyte pools- bones act as an electrolyte pool and store calcium magnesium, and phosphate i ... ons; shift of electrolytes into electrolyte pools will decrease plasma electrolyte concentration and shift of electrolytes from an electrolyte pool into the extracellular fluid will increase the plasma electrolyte concentration Ch. 7 Neoplasia • Metastasis- process by which cancer cells escape their tissue of origin and initiate new colonies of cancer in distant sites Ch. 9 Inflammation and Immunity • Passive vs active immunity- Passive: transfer of preformed antibodies against specific antigen from a protected or immunized individual to an unprotected or nonimmunized individual; types: mother to fetus: IgG- can cross placenta, mother to infant: IgA- from breast milk, serotherapy- direct injections of antibodies (human or animal); active: a protected state owing to the body’s immune response as a result of active infection or immunization, types: immunizations- vaccines • Immunoglobulins- antibodies; two identical light polypeptide chains joined to identical heavy polypeptide chains by disulfide bonds; five different classes: IgG, IgM, IgA, IgD, & IgE • Ch. 11 Malignant Disorders of White Blood Cells • Chronic myeloid leukemia (CML)- characterized by malignant granulocytes that carry the Philadelphia chromosome (Ph+); does not respond well to chemotherapy: poor overallsurvival time; Blast stage CML- poor prognosis: 3 to 4 months; treatment- bone marrow transplant • Age of onset for multiple myeloma- median age 65 years • Malignant Disorders of WBCs- may be nonspecific signs & symptoms • Ch. 13 Alterationsin Oxygen Transport • Anemia- occursfrom a manifestation of diseases; a deficit of RBCs; leads to hypoxia • Polycythemia- excess of RBCs; increases blood viscosity & volume; leadsto hypertension • Erythropoietin- is stimulated from the kidney secretion hormone to stimulates RBC production • Acute blood loss- type of anemia; may be from trauma or secondary to a disease process; symptoms develop with activity at 20% loss of blood volume (tachycardia and postural drop in BP), and increase in severity with continued blood loss; shock and death can occur with 50% loss of circulating volume; treatment: blood volume replacement therapy with crystalloids, colloids, and fresh whole blood; prognosis: excellent with treatment unless blood loss is severe • Ch. 14 Alterationsin Hemostasis and Blood Coagulation This study source was downloaded by 100000831941162 from CourseHero.com on 09-22-2021 11:25:56 GMT -05:00 https://www.coursehero.com/file/46425461/NUR2063-Exam-3-Focused-Review-docx/ • Thrombocytopenia causes- 1) bone marrow suppression from chemotherapy, 2) recent immunizations, 3) alcohol ingestion, 4) decreased platelet production, 5) decreased platelet survival, 6) splenic sequestration, & 7) intravascular dilution of circulating platelets from transfusion • DIC (Disseminated Intravascular Coagulation)- acquired hemorrhagic syndrome in which clotting, and bleeding occursimultaneously. Widespread clot formation in small vessels; clotting and platelets consumed resulting in bleeding. Causes: trauma, malignancy, burns, shock, and abruptio placentae. Clinical manifestations: fibrinogen level and platelet count decreased, increased bleeding time, elevated PT/INR/aPTT, elevated D-dimer/fibrin split products. Treatment: Removal/correction of underlying cause,support major organs, fresh frozen plasma, packed red blood cells, platelets, or cryoprecipitate, heparin used to minimize further consumption of clotting factors (controversial). • Ch. 15 Alterations in Blood Flow • Atherosclerosisis the leading cause of coronary artery/heart disease Ch. 16 Alterationsin Blood Pressure • Treatment of hypertension- (lifestyle modifications) weight loss, exercise, DASH diet, alcohol moderation, decreased sodium intake; drug therapy affects HR, SVR, and/or stroke volume • Long term problems from hypertension- Renal failure, stroke, heart disease, Damage to arterial system and acceleration of atherosclerosis lead to cardiovascular disease, Increased myocardial work results in heart failure, Glomerular damage results in kidney failure, Affects microcirculation of the eyes, Increased pressure in cerebral vasculature can result in hemorrhage • Modifiable vs nonmodifiable risk factors for hypertension- modifiable: dietary factors, sedentary lifestyle, obesity/weight gain, metabolic syndrome, elevated blood glucose levels/diabetes, elevated total cholesterol, alcohol & smoking; nonmodifiable: family history, age, ethnicity/genetics • Ch. 18 Alterationsin Cardiac Function • Coronary artery disease: characterized by insufficient delivery of oxygenated blood to the myocardium caused by atherosclerotic coronary arteries; known risk factor: atherosclerosis • How to determine causes of acute coronary syndrome: associated with acute changes in plaque morphology and thrombosis; evidence of acute ischemia on ECG- STEMI-candidates for acute reperfusion therapy; no ST elevation on ECG- non-STEMI- candidates for antiplatelet drugs; treatment: reperfusion • diagnosis and prognosis: diagnosis: Signs and symptoms, Electrocardiographic changes, Elevations ofspecific marker proteinsin the blood, Severe crushing, excruciating chest pain that may radiate to the arm, shoulder, jaw, or back, Accompanied by nausea, vomiting, diaphoresis (sweating), shortness of breath, prognosis: difficult to determine b/c of many different factors; After 18 to 24 hours: area of infarction becomes paler than surrounding tissues, 5 to 7 days: turns yellowish and soft with a rim of red vascular connective tissue, At 1 to 2 weeks: necrotic This study source was downloaded by 100000831941162 from CourseHero.com on 09-22-2021 11:25:56 GMT -05:00 https://www.coursehero.com/file/46425461/NUR2063-Exam-3-Focused-Review-docx/ tissue progressively degraded and cleared away; infarcted myocardium weakened and susceptible to rupture, By 6 weeks: necrotic tissue replaced by tough fibrousscar tissue • Unstable angina pectoris vs stable angina- angina pectoris: chest pain associated with intermittent myocardial ischemia;stable angina: most common; also called classic; chronic occlusion of a coronary vessel; chronic syndromes with slow progression because of chronic obstruction from stable atherosclerotic plaques; unstable/crescendo angina pectoris: [Show More]
Last updated: 3 years ago
Preview 1 out of 9 pages
Buy this document to get the full access instantly
Instant Download Access after purchase
Buy NowInstant download
We Accept:

Reviews( 0 )
$10.00
Can't find what you want? Try our AI powered Search
Document information
Connected school, study & course
About the document
Uploaded On
Sep 26, 2021
Number of pages
9
Written in
All

Additional information
This document has been written for:
Uploaded
Sep 26, 2021
Downloads
0
Views
196