*NURSING > CASE STUDY > NR 603 WEEK 3 CASE DISCUSSION : CARDIOVASCULAR - DOWNLOAD TO SCORE AN A GRADE (All)
NR 603 WEEK 3 CASE DISCUSSION : CARDIOVASCULAR - DOWNLOAD TO SCORE AN A GRADE
Document Content and Description Below
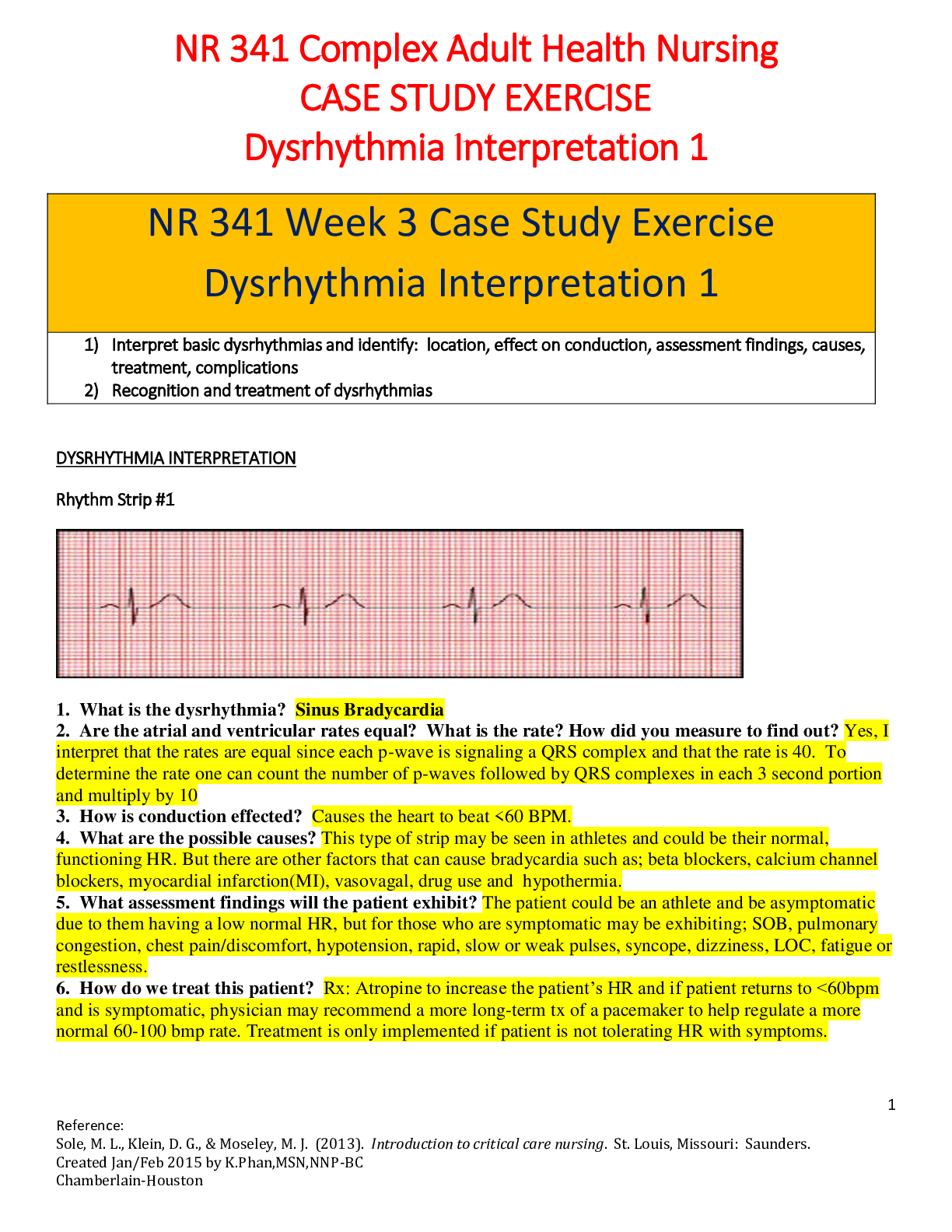
Week 3 Case Discussion: Cardiovascular Patient Information: Lorene, 60-year-old African American female, insurance unknown. SOAP S: Lorene’s chief complaint is shoulder discomfort and shortness ... of breath following exercise that started three days ago. She felt "a discomfort" radiating back and up between her shoulder blades. She also experienced feelings of nausea as well as sweat. However, these symptoms were resolved 3 minutes after exercises and have not recurred. The patient reports currently not being on medication after stopping Lisinopril that she was on, citing learning its side effects. Hx allergy to metformin, GI disturbance. PMH: Admits challenge to make healthy food choices. Exercise and diet has been the patient’s weight loss routine. The patient feels a little more tired than usual since stopping workout after chest pain. Chronic illnesses: Hypertension, Dyslipidemia, and Metabolic Syndrome. Moreover, gestational Diabetes has been experienced in the last 3 pregnancies which was managed with Insulin. Surgeries: T and A, cholecystectomy Childhood/previous illnesses: chickenpox. Immunization: None. Does not receive the flu shot. Soc Hx: Reports being a married for the last 20 years. Patient regularly eats out and consumes beer, wine, or cigarettes while entertaining clients on a weekly basis as part of her role as a CEO of a marketing company. Fam Hx: Lung cancer (father), mother (stroke and diabetes type 2), brother (malignant melanoma), sister and brother (metabolic syndrome) ROS: CONSTITUTIONAL: Reports increased fatigue as of 3 days ago. Planned weight loss. Does not report experiencing fever or chills. HEENT: None SKIN: None. CARDIOVASCULAR: Experiences shortness of breath, chest heaviness, sweating, and nausea. RESPIRATORY: Shortness of breath 3 days ago, none since. No sputum reported. GASTROINTESTINAL: Nausea as of 3 days ago. GENITOURINARY: None. NEUROLOGICAL: None. MUSCULOSKELETAL: None HEMATOLOGIC/LYMPHATICS: None. PSYCHIATRIC: None. ENDOCRINOLOGIC: None. ALLERGIES: None. O: Vital signs: BP 146/90 P 70 SaO2 97% Height 5'8", Weight 220 pounds, BMI 33.5 General: African American female in NAD. Alert, oriented, and cooperative. Pain: 0/10 now. Skin: Warm, dry, and intact. Light brown in color. No cyanosis or pallor. HEENT: Head normo-cephalic. Thick and evenly distributed hair. Eyes: Sclera clear. Conjunctiva: white, PERRLA, EOMs intact. No AV nicking noted. Ears: Tympanic membranes gray and intact with light reflex noted. Pinna and tragus are non-tender. Nose: Nares patent without exudate. Sinuses nontender to palpation, Right-sided Deviation Throat: Oropharynx moist, no lesions, or exudate. Teeth in poor repair, gums reddened and receding, filled cavities noted. Tongue smooth, pink, no lesions, protrudes in the midline. Neck supple. No cervical lymphadenopathy or tenderness noted. Thyroid midline, small and firm without palpable masses. Mild JVD in a recumbent position Lungs: Lungs clear to auscultation bilaterally. Respirations are unlabored. No rashes or vesicles noted on the chest. CV: Heart S1 and S2 noted, RRR, no murmurs, noted. No parasternal lifts, heaves, and thrills. Peripheral pulses equal bilaterally. PMI 5thICS displaced 4cm laterally. Trace edema in lower extremities. Abdomen: Abdomen round, soft, with bowel sounds noted in all four quadrants. No organomegaly noted. Diagnostic results: Labs from 3 months ago: RBS 130mgs/dl, within the upper limit of normal. Hemoglobin A1C 6.4% is elevated indicating the risk of diabetes. Fasting glucose 135mgs/dl, prediabetes. Total Cholesterol 230 Triglycerides 180mgs/dl, Ldl 180, Hdl 38, each one is deranged indicating dyslipidemia. An ECG taken today in the office shows ST Depression. What Leads Demonstrate the ST Depression? Leads V2, V3, V4, V5, and V6 all demonstrate the ST depression. Harhash et al. (2019) cite coronary insufficiency as a major cause of the finding. A: What is the primary diagnosis causing Lorene's chest pain? Include ICD 10 code. Angina pectoris, unspecified - I20.9 What other secondary diagnoses does Lorene have that should be addressed? (Include the rationale and a reference for your diagnoses) 1. Essential (primary) hypertension, I10: Hypertension refers to sustained elevation of resting systolic blood pressure (≥ 130 mm Hg), diastolic blood pressure (≥ 80 mm Hg), or both (Ioannidis, 2018). Lorene is prior documented to have the illness, and at the time of the visit has a BP of 146/90 mm Hg. 2. Hyperlipidemia, unspecified E78. 5. Adhyaru and Jacobson (2016) indicate that hyperlipidemia is the elevation of plasma cholesterol, triglycerides (TGs), or both, or a low HDL cholesterol level which may cause atherosclerosis development. As noted above, Lorene’s total cholesterol, TGs, and LDLs are elevated, while her HDLs are below the normal range. 3. Metabolic Syndrome, E88. 81: As per Engin (2017), metabolic syndrome features a large waist circumference from excessive abdominal fat, hypertension, deranged fasting plasma glucose or insulin resistance, as well as dyslipidemia. Hypertension, dyslipidemia, and deranged fasting plasma glucose are above mentioned and noted. P: Design a treatment plan and discuss how each intervention is applicable to Lorene's case. Angina pectoris: Thadani (2016) suggests diagnosis and treatment, whereby disease can be determined clinically, with ECG, and cardiac imaging. Stress testing with ECG or imaging on echocardiography, radionuclide imaging, or MRI is beneficial. Coronary angiography is reserved for significant symptoms or positive stress tests. Antiplatelet drugs are given prophylactically. Others include nitrates, beta- blockers, calcium channel blockers, ACE inhibitors, or statins. Coronary angioplasty or coronary artery bypass graft surgery can be indicated. Hypertension: As indicated by Ioannidis (2018), separate blood pressure readings on digital or sphygmomanometry measurements are diagnostic. Other tests are for complications, including urinalysis and urinary albumin: creatinine ratio. Blood tests include fasting lipids, creatinine, potassium. Pheochromocytoma may be evaluated. Lifestyle and antihypertensive drug interventions are appropriate. Is Lorene Hypertensive per ACA 2017 Guidelines? Compare the ACC guidelines to JNC 8 guidelines and discuss what treatment you recommend for her BP and why. ACC 2017 guidelines define older patients as ≥65 years and <130/80 mmHg as BP targets (Cifu and Davis, 2017). In JNC 8 guidelines older patients are alluded to as ≥60 years, with BP targets of <150/90 mmHg (Currie & Delles, 2018). In the ACC guidelines, Ioannidis (2018) recommends in the black patient of stage 2 hypertension with clinical atherosclerotic cardiovascular disease (ASCVD), a two- drug therapy. A thiazide diuretic and an ACE inhibitor are prescribed. Metabolic syndrome: Hemoglobin A1C and lipids will be monitored in this visit and three months later. Treatment is through dietary changes, exercise, and lipid- lowering drugs, especially statins Prescription: Rx: Hydrochlorothiazide 12.5 mg tablet Sig: Take one tablet once daily Dispense: 30 Refills: 3 Rx: Ramipril 1.25 mg tablet Sig: Take one tablet 4 times a day Dispense: 30 Refills: 3 Rx: Aspirin 325 mg tablet Sig: Take one tablet daily Dispense: OTC Rx: Nitroglycerin 0.3mg tablet Sig: Take 1 tablet SL every 5 minutes up to 3 doses for chest pain Dispense: 30 Refills: 3 Rx: Simvastatin 20mg tablet Sig: Take one tablet every evening Dispense: 30 Refills: 3 Rx: Pneumococcal vaccine 13-valent IM injection 0.5mL/syringe, stat Patient Education Lorene should take blood pressures in the morning at home recording readings every morning on booklet or phone app. She should continue a healthy diet with low sodium and cholesterol. Recommend specialized physical training. Limit alcohol and stop cigarette smoking. Advice that pneumococcal vaccine is due to the current smoking risk factor. Referrals/Consults Lorena should go to the cardiology department for further assessment and management of angina pectoris. A nutritional consult will specify a diet plan. Consult an exercise physiologist for specialized physical training. Follow-up Plan Visit the cardiology department within the week for further assessment. Return in a week to evaluate symptom improvement and review drugs References Adhyaru, B. B., & Jacobson, T. A. (2016). New cholesterol guidelines for the management of atherosclerotic cardiovascular disease risk: a comparison of the 2013 American College of Cardiology/American Heart Association cholesterol guidelines with the 2014 National Lipid Association recommendations for patient- centered management of dyslipidemia. Endocrinology and Metabolism Clinics, 45(1), 17-37. doi: 10.1016/j.ccl.2015.02.001 Cifu, A. S., & Davis, A. M. (2017). Prevention, detection, evaluation, and management of high blood pressure in adults. Jama, 318(21), 2132-2134. doi: 10.7326/M17-3203 Currie, G., & Delles, C. (2018). Blood pressure targets in the elderly. Journal of hypertension, 36(2), 234. doi: 10.1097/HJH.0000000000001576 Engin, A. (2017). The definition and prevalence of obesity and metabolic syndrome. In Obesity and Lipotoxicity (pp. 1-17). Springer, Cham. doi: 10.1007/978-3-319-48382-5_1 Harhash, A. A., Huang, J. J., Reddy, S., Natarajan, B., Balakrishnan, M., Shetty, R., ... & Kern, K. B. (2019). aVR ST segment elevation: acute STEMI or not? Incidence of an acute coronary occlusion. The American journal of medicine, 132(5), 622-630. doi: 0.1016/j.amjmed.2018.12.021 Ioannidis, J. P. (2018). Diagnosis and treatment of hypertension in the 2017 ACC/AHA guidelines and in the real world. Jama, 319(2), 115-116. doi: 10.1001/jama.2017.19672 Thadani, U. (2016). Management of stable angina–current guidelines: a critical appraisal. Cardiovascular drugs and therapy, 30(4), 419-426.Thadani, U. (2016). Management of stable angina–current guidelines: a critical appraisal. Cardiovascular drugs and therapy, 30(4), 419-426. doi: 10.1007/s10557-016- 6681-2 [Show More]
Last updated: 2 years ago
Preview 1 out of 6 pages
Buy this document to get the full access instantly
Instant Download Access after purchase
Buy NowInstant download
We Accept:


Reviews( 0 )
$16.00
Can't find what you want? Try our AI powered Search
Document information
Connected school, study & course
About the document
Uploaded On
Mar 07, 2023
Number of pages
6
Written in

Additional information
This document has been written for:
Uploaded
Mar 07, 2023
Downloads
0
Views
122






.png)