NUR 105 G.I. ReviewNUR 105 G.I. Review
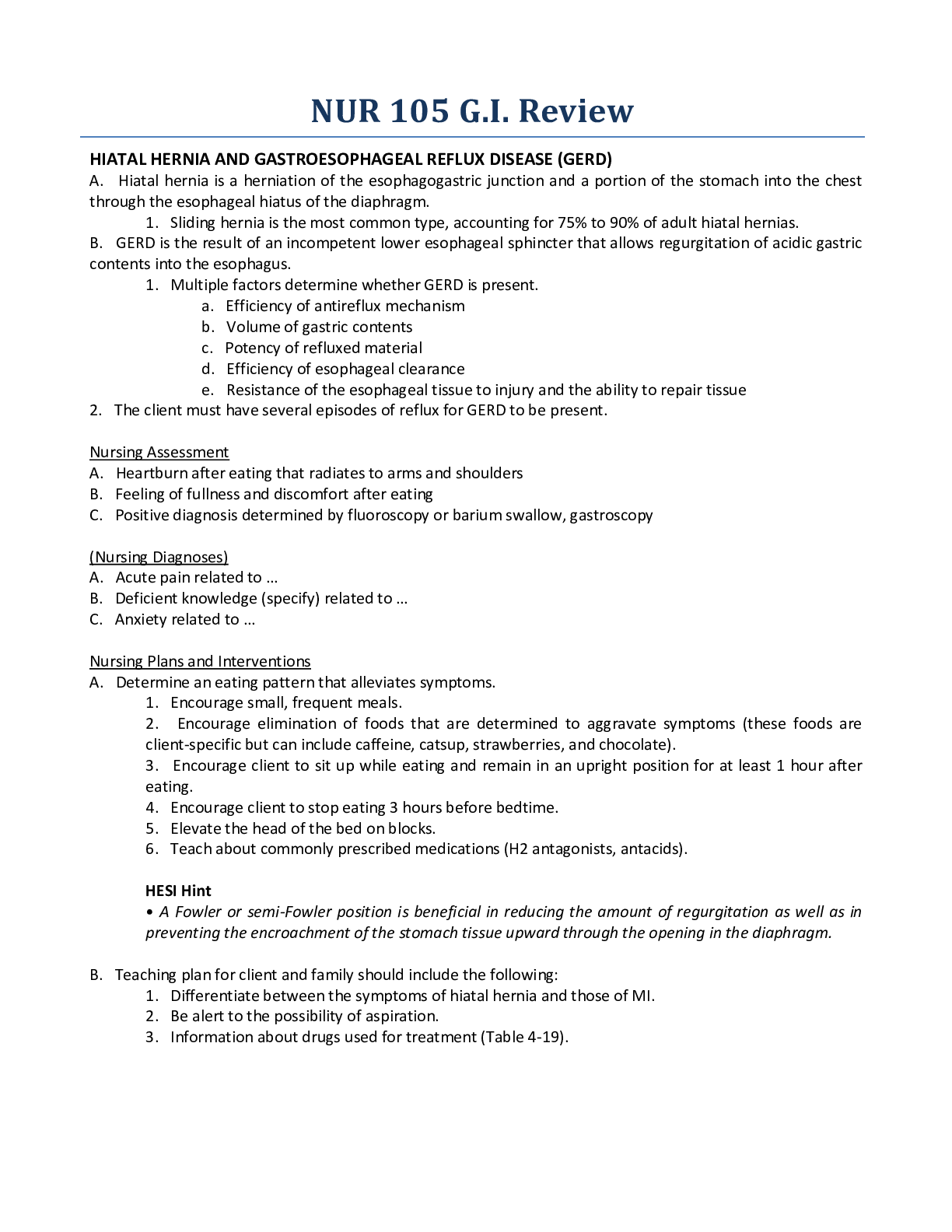
HIATAL HERNIA AND GASTROESOPHAGEAL REFLUX DISEASE (GERD)
A. Hiatal hernia is a herniation of the esophagogastric junction and a portion of the stomach into the chest
through the
...
NUR 105 G.I. ReviewNUR 105 G.I. Review
HIATAL HERNIA AND GASTROESOPHAGEAL REFLUX DISEASE (GERD)
A. Hiatal hernia is a herniation of the esophagogastric junction and a portion of the stomach into the chest
through the esophageal hiatus of the diaphragm.
1. Sliding hernia is the most common type, accounting for 75% to 90% of adult hiatal hernias.
B. GERD is the result of an incompetent lower esophageal sphincter that allows regurgitation of acidic gastric
contents into the esophagus.
1. Multiple factors determine whether GERD is present.
a. Efficiency of antireflux mechanism
b. Volume of gastric contents
c. Potency of refluxed material
d. Efficiency of esophageal clearance
e. Resistance of the esophageal tissue to injury and the ability to repair tissue
2. The client must have several episodes of reflux for GERD to be present.
Nursing Assessment
A. Heartburn after eating that radiates to arms and shoulders
B. Feeling of fullness and discomfort after eating
C. Positive diagnosis determined by fluoroscopy or barium swallow, gastroscopy
(Nursing Diagnoses)
A. Acute pain related to …
B. Deficient knowledge (specify) related to …
C. Anxiety related to …
Nursing Plans and Interventions
A. Determine an eating pattern that alleviates symptoms.
1. Encourage small, frequent meals.
2. Encourage elimination of foods that are determined to aggravate symptoms (these foods are
client-specific but can include caffeine, catsup, strawberries, and chocolate).
3. Encourage client to sit up while eating and remain in an upright position for at least 1 hour after
eating.
4. Encourage client to stop eating 3 hours before bedtime.
5. Elevate the head of the bed on blocks.
6. Teach about commonly prescribed medications (H2 antagonists, antacids).
HESI Hint
• A Fowler or semi-Fowler position is beneficial in reducing the amount of regurgitation as well as in
preventing the encroachment of the stomach tissue upward through the opening in the diaphragm.
B. Teaching plan for client and family should include the following:
1. Differentiate between the symptoms of hiatal hernia and those of MI.
2. Be alert to the possibility of aspiration.
3. Information about drugs used for treatment (Table 4-19).PEPTIC ULCER DISEASE (PUD)
Description: Ulceration that penetrates the mucosal wall of the GI tract
A. Gastric ulcers tend to occur in the lesser curvature of the stomach.
B. Duodenal ulcers occur in the duodenum.
C. Esophageal ulcers occur in the esophagus.
D. The cause of some peptic ulcer disease is unknown. A significant number of gastric ulcers are caused by a
bacterium, Helicobacter pylori (H. pylori), and can be successfully treated by drug therapy.
Risk factors for the development of peptic ulcers include:
1. Drugs (NSAIDs, corticosteroids)
2. Alcohol
3. Cigarette smoking
4. Acute medical crisis or trauma
E. Symptoms common to all types of ulcers include the following:
1. Belching
2. Bloating
3. Epigastric pain radiating to the back (not associated with the type of food eaten) and relieved by
antacids
Nursing Assessment
A. Determine how food intake affects pain.
B. Take history of antacid or histamine antagonist use.
C. Determine presence of melena.
D. Determine presence and location of peptic ulcer as determined by:
1. Barium swallow
2. Upper endoscopy
3. Gastric analysis indicating increased levels of stomach acid
E. Potential complications
1. Hemorrhage
2. Perforation (which always requires surgery)
3. Obstruction
(Nursing Diagnoses)
A. Acute pain related to …
B. Imbalanced nutrition: less than body requirements related to …
C. Deficient knowledge related to …
D. Risk for injury related to …
Nursing Plans and Interventions
A. Determine symptom onset and how symptoms are relieved.
B. Monitor color, quantity, consistency of stools and emesis, and test for occult blood.
C. Administer medications as prescribed, usually 1 to 2 hours after meals and at bedtime (see Table 4-19).
D. Administer mucosal healing agents at least 1 hour before meals, as prescribed (see Table 4-19).
E. Encourage small, frequent meals; no bedtime snacks; and avoidance of beverages containing caffeine.
F. Prepare client for surgery if uncontrolled bleeding, obstruction, or perforation occurs.
1. Gastric resection
2. Vagotomy
3. Pyloroplasty
G. Teach client that dumping syndrome may occur postoperatively.
1. Secondary to rapid entry of hypertonic food into jejunum (pulls water out of bloodstream)
2. Occurs 5 to 30 minutes after eating3. Characterized by vertigo, syncope, sweating, pallor, tachycardia
4. Minimized by small, frequent meals: high-protein, high-fat, low-carbohydrate diet
5. Exacerbated by consuming liquids with meals; helped by lying down after eating
6. Can also be observed in clients on hypertonic tube feeding
H. Teach client to avoid medications that increase the risk for developing peptic ulcers.
1. Salicylates
2. NSAIDs such as ibuprofen
3. Corticosteroids in high doses
4. Reserpine (antihypertensive)
5. Anticoagulants
I. Teach client the importance of informing all health care personnel of ulcer history.
J. Teach client symptoms of GI bleeding.
1. Dark, tarry stools
2. Coffee-ground emesis
3. Bright-red rectal bleeding
4. Fatigue
5. Pallor
6. Severe abdominal pain, which should be reported immediately (could denote perforation)
K. Teach client importance of smoking cessation and stress management.
HESI Hint
• Stress can cause or exacerbate ulcers. Teach stress-reduction methods, and encourage those with a
family history of ulcers to obtain medical surveillance for ulcer formation.
• Clinical manifestations of GI bleeding:
• Pallor: conjunctival, mucous membranes, nail beds
• Dark, tarry stools
• Bright-red or coffee-ground emesis
• Abdominal mass or bruit
• Decreased BP, rapid pulse, cool extremities (shock), increased respirations
INFLAMMATORY BOWEL DISEASES
Description: Consists of Crohn disease and ulcerative colitis
Crohn Disease (Regional Enteritis)
Description: Subacute, chronic inflammation extending throughout the entire intestinal mucosa (most
commonly found in terminal ileum) with periods of remission interspersed with periods of exacerbation. Crohn
disease occurs during the teenage years and early adulthood but has a second peak in the sixth decade.
Capsule endoscopy has shown greater sensitivity than radiography when diagnosing Crohn disease. There is no
known cause and no cure, so treatment relies on medications to treat the acute inflammation and maintain a
remission. Surgery is reserved for patients who are unresponsive to medications or who develop lifethreatening complications. In a total proctocolectomy (the colon and rectum are removed and the anus is
closed), the terminal ileum is brought through the abdominal wall, and a permanent ileostomy is formed.
Nursing Assessment
A. Abdominal pain (unrelieved by defecation)
B. Diarrhea, steatorrhea (fatty diarrheal stools), and weight loss, with client becoming emaciated
C. Constant fluid loss
D. Low-grade fever
E. Perforation of the intestine occurring due to severe inflammation; constitutes a medical emergency(Nursing Diagnoses)
A. Risk for deficient fluid volume related to …
B. Chronic pain related to …
C. Imbalanced nutrition: less than body requirements related to …
Nursing Plans and Interventions
A. Determine bowel elimination pattern, and control diarrhea with diet and medication as indicated.
B. Provide a nutritious, well-balanced, low-residue, low-fat, high-protein, high-calorie diet, with no dairy
products.
C. Administer vitamin supplements and iron.
D. Advise client to avoid foods that are known to cause diarrhea, such as milk products and spicy foods.
E. Advise client to avoid smoking, caffeinated beverages, pepper, and alcohol.
F. Provide complete bowel rest with IV hyperalimentation if necessary.
G. Administer medications as prescribed: aminosalicylates, antimicrobials, corticosteroids,
immunosuppressants, and biologic therapy
H. Monitor I& O and serum electrolytes.
I. Weigh at least twice a week.
J. Provide emotional support, and encourage use of support groups such as the Crohn’s and Colitis
Foundation of America.
K. Encourage client to talk with the enterostomal therapists before surgery.
L. If ileostomy is performed, teach stoma care.
HESI Hint
• The GI tract usually accounts for only 100 to 200 ml of fluid loss per day, although it filters up to 8 L
per day. Large fluid losses can occur if vomiting or diarrhea exists.
Ulcerative Colitis
Description: Disease that affects the superficial mucosa of the colon, causing the bowel to eventually narrow,
shorten, and thicken due to muscular hypertrophy; occurs in the large bowel and rectum. Sigmoidoscopy and
colonoscopy allow direct examination of the large intestine mucosa and are used for diagnosis of ulcerative
colitis.
Nursing Assessment
A. Diarrhea
B. Abdominal pain and cramping
C. Intermittent tenesmus (anal contractions) and rectal bleeding
D. Liquid stools containing blood, mucus, and pus (may pass 10 to 20 liquid stools per day)
E. Weakness and fatigue
F. Anemia
(Nursing Diagnoses)
A. Risk for deficient fluid volume related to …
B. Acute pain related to …
C. Imbalanced nutrition: less than body requirements related to …
Nursing Plans and Interventions
A. Determine bowel elimination pattern, and control diarrhea with diet and medication as indicated.
B. Provide a nutritious, well-balanced, low-residue, low-fat, high-protein, high-calorie diet, with no dairy
products.
C. Administer vitamin supplements and iron.D. Advise client to avoid foods that are known to cause diarrhea, such as milk products and spicy foods.
E. Advise client to avoid smoking, caffeinated beverages, pepper, and alcohol.
F. Provide complete bowel rest with IV hyperalimentation if necessary.
G. Administer medications as prescribed, often steroids, antidiarrheals, sulfasalazine (Azulfidine).
H. Monitor I& O and serum electrolytes.
I. Weigh at least twice a week.
J. Provide emotional support, and encourage use of support groups such as the local Ileitis and Colitis
Foundation.
K. Encourage client to talk with the enterostomal therapists before surgery.
L. If ileostomy is performed, teach stoma care.
HESI Hint
• Opiate drugs tend to depress gastric motility. However, they should be given with care, and those
receiving them should be closely monitored because a distended intestinal wall accompanied by
decreased muscle tone may lead to intestinal perforation.
Diverticular Diseases
Description: Manifested in two clinical forms: diverticulosis and diverticulitis
A. Diverticulosis: bulging pouches in the GI wall (diverticula), which push the mucosa lining through the
surrounding muscle
B. Diverticulitis: inflamed diverticula, which may cause obstruction, infection, and hemorrhage
HESI Hint
• Diverticulosis is the presence of pouches in the wall of the intestine. There is usually no discomfort,
and the problem goes unnoticed unless seen on radiologic examination (usually prompted by some
other condition). Diverticulitis is an inflammation of the diverticula (pouches), which can lead to
perforation of the bowel.
Nursing Assessment
A. Left lower quadrant pain
B. Increased flatus
C. Rectal bleeding
D. Signs of intestinal obstruction:
1. Constipation alternating with diarrhea
2. Abdominal distention
3. Anorexia
4. Low-grade fever
E. Barium enema or colonoscopy positive for diverticular disease: obstruction, ileus, or perforation confirmed
by abdominal radiograph (barium not used during acute phase of illness)
(Nursing Diagnoses)
A. Ineffective tissue perfusion related to …
B. Acute pain related to …
C. Imbalanced nutrition: less than body requirements related to …
Nursing Plans and Interventions
A. Provide a well-balanced, high-fiber diet unless inflammation is present, in which case client is NPO,
followed by low-residue bland foods.HESI Hint
• A client admitted with complaints of severe lower abdominal pain, cramping, and diarrhea is
diagnosed as having diverticulitis. What are the nutritional needs of this client throughout recovery?
• Acute phase: NPO, graduating to liquids
• Recovery phase: no fiber or foods that irritate the bowel
• Maintenance phase: high-fiber diet with bulk-forming laxatives to prevent pooling of foods in the
pouches where they can become inflamed; avoidance of small, poorly digested foods such as popcorn,
nuts, seeds, etc.
B. Include bulk-forming laxatives such as Metamucil in daily regimen.
C. Increase fluid intake to 3 L/ day.
D. Monitor I& O and bowel elimination; avoid constipation.
E. Observe for complications.
1. Obstruction
2. Peritonitis
3. Hemorrhage (With ruptured diverticula, a temporary colostomy is performed and maintained for
approximately 3 months to allow the bowel to rest.)
4. Infection
INTESTINAL OBSTRUCTION
Description: Partial or complete blockage of intestinal flow (fluids, feces, gas)
A. Mechanical causes of intestinal obstruction
1. Adhesions (most common cause).
2. Hernia (strangulates the gut).
3. Volvulus (twisting of the gut).
4. Intussusception (telescoping of the gut within itself).
5. Tumors; develop slowly; usually a mass of feces becomes lodged against the tumor
B. Neurogenic causes of intestinal obstruction
1. Paralytic ileus (usually occurs in postoperative clients)
2. Spinal cord lesion
C. Vascular cause of intestinal obstruction
1. Mesenteric artery occlusion (leads to gut infarct)
HESI Hint
• BOWEL OBSTRUCTIONS
• Mechanical: Due to disorders outside the bowel (hernia, adhesions) caused by disorders within the
bowel (tumors, diverticulitis) or by blockage of the lumen in the intestine (intussusception, gallstone)
• Nonmechanical: Due to paralytic ileus, which does not involve any actual physical obstruction but
results from inability of the bowel itself to function
Nursing Assessment
A. Sudden onset of abdominal pain, tenderness, or guarding
B. History of abdominal surgeries
C. History of obstruction
D. Distention
(Nursing Diagnoses)
A. Impaired tissue perfusion related to …
B. Deficient volume related to …
C. Acute pain related to …HESI Hint
• Blood gas analysis will show an alkalotic state if the bowel obstruction is high in the small intestine
where gastric acid is secreted. If the obstruction is in the lower bowel where base solutions are
secreted, the blood will be acidic.
Nursing Plans and Interventions
A. Maintain client NPO, with IV fluids and electrolyte therapy.
B. Monitor I& O; a Foley catheter maintains strict output.
C. Implement NG intubation.
1. Attach to low suction (intermittent 80 mm Hg).
2. Document output every 8 hours.
3. Irrigate with normal saline if policy dictates.
D. NG tube, Cantor, Miller-Abbott, or Harris tubes are passed through the nose and into the stomach, usually
by the health care provider.
1. Advance tube every 1 to 2 hours.
2. Do not secure to nose until tube reaches specified position.
3. Reposition client every 2 hours to assist with placement of the tube.
4. Connect to suction.
5. Irrigate with air only.
6. Note amount, color, consistency, and any unusual odor of drainage.
E. Document pain; medicate as prescribed.
F. Assess abdomen regularly for distention, rigidity, change in status of bowel sounds.
G. If conservative medical interventions fail, surgery will be required to remove obstruction.
HESI Hint
• A client admitted with complaints of constipation, thready stools, and rectal bleeding over the past
few months is diagnosed with a rectal mass. What are the nursing priorities for this client?
• NPO
• NG tube (possibly an intestinal tube such as a Miller-Abbott)
• IV fluids • Surgical preparations of bowel (if obstruction is complete)
• Foods and fluids are restricted for 8 to 10 hours before surgery if possible.
• If the patient has a bowel obstruction or perforation, bowel cleansing is contraindicated.
• Oral erythromycin and neomycin are given to further decrease the amount of colonic and rectal
bacteria. • If possible, all clients who require surgery for obstruction undergo NG intubation and
suction before surgery. However, in cases of complete obstruction, surgery should proceed without
delay
• Teaching (preoperative nutrition, etc.)
COLORECTAL CANCER
Description: Tumors occurring in the colon
A. Cancer of the colon is the fourth most common cancer in the United States.
B. This is second leading cause of cancer-related deaths in the United States.
C. Approximately 45% of cancerous tumors of the colon occur in the rectal or sigmoid area, 25% in the cecum
and ascending colon, and 30% in the remainder of colon.
D. The highest incidence occurs in persons over 50 years of age.
E. A diet of high-fiber, low-fat foods, including cruciferous vegetables, may be a factor in prevention of colon
cancer.
F. Early detection is important.HESI Hint
• Diet recommended by the American Cancer Society to prevent bowel cancer:
• Eat more cruciferous vegetables (those from the cabbage family, such as broccoli, cauliflower,
Brussels sprouts, cabbage, and kale).
• Increase fiber intake.
• Maintain average body weight.
• Eat less animal fat.
• American Cancer Society recommendations for early detection of colon cancer:
• A digital rectal examination every year after 40.
• A stool blood test every year after 50.
• A colonoscopy or sigmoidoscopy examination every 3 to 5 years after the age of 50, based on the
advice of a physician.
G. Usual treatment is surgical removal of the tumor, with adjuvant radiation or antineoplastic chemotherapy.
H. Diagnosis is made by digital examination, flexible fiberoptic sigmoidoscopy with biopsy, colonoscopy, and
barium enema.
I. Carcinoembryonic antigen (CEA) serum level is used to evaluate effectiveness of chemotherapy.
Nursing Assessment
A. Rectal bleeding
B. Change in bowel habits
C. Sense of incomplete evacuation
D. Abdominal pain, nausea, vomiting
E. Weight loss, cachexia
F. Abdominal distention or ascites
G. Family history of cancer, particularly cancer of the colon H. History of polyps
(Nursing Diagnoses)
A. Deficient knowledge related to …
B. Ineffective coping (specify) related to …
C. Disturbed body image related to …
Nursing Plans and Interventions
A. Prepare client for surgery.
B. Prepare client for bowel preparation, which may include laxatives and gut lavage with polyethylene glycol
(Golytely).
C. If colostomy has been performed, teach stoma care.
D. Provide high-calorie, high-protein diet.
E. Promote prevention of constipation with high-fiber diet.
F. Encourage early detection by screening with Hemoccult (guaiac) tests.
HESI Hint
• An early sign of colon cancer is rectal bleeding. Encourage patients 50 years of age or older and those
with increased risk factors to be screened yearly with fecal occult blood testing. Routine colonoscopy at
50 is also recommended.
Stoma Care
A. General information
1. The more distal the stoma is, the greater is the chance for continence.
2. An ileostomy drains liquid material; peristomal skin is prone to breakdown by enzymes.3. The lower the stoma’s location is in the GI tract, the more solid, or formed, is the effluence (stoma
drainage).
4. The greatest chance for continence is with a stoma created from the sigmoid colon on the left side
of the abdomen.
5. Consultation with an enterostomal therapist is essential.
B. Preoperative care
1. Client and family must be informed about what to expect postoperatively:
a. Proposed location of the stoma
b. Approximate size
c. What it will look like (Provide a picture, if indicated.)
2. The family should be included in teaching, but it should be emphasized that the client is ultimately
responsible for his or her own care.
C. Pouch care
1. Ostomates often wear pouches.
2. The adhesive-backed opening, designed to cover the stoma, should provide about ⅛-inch clearance
from the stoma.
3. A rubber band or clip is used to secure the bottom of the pouch and prevent leakage.
4. A simple squirt bottle is used to remove effluence from the sides of the bag. Pouch system is
changed every 3 to 7 days.
5. Clients should maintain an extra supply of pouches so that they never run out and should change
the pouch when bowel is inactive.
6. Pouch should be emptied when one third to one half full.
D. Irrigation
1. Those with descending-colon colostomies can irrigate to provide control over effluence.
a. Clients should irrigate at approximately the same time daily.
b. Clients should use warm water (cold or hot water causes cramping).
c. Clients should wash around stoma with lukewarm water and a mild soap.
d. Commercial skin barriers may be purchased for home use.
2. Odor control
a. Commercial preparations are available.
b. Foods in diet that cause offensive odors can be eliminated.
E. Diet
1. Ileostomy
a. Clients should chew food thoroughly.
b. High-fiber foods (popcorn, peanuts, unpeeled vegetables) can cause severe diarrhea and
may have to be eliminated.
2. Colostomy
a. Client should resume the regular diet gradually. Foods that were a problem preoperatively
should be tried cautiously.
HESI (2010-10-28). HESI Comprehensive Review for the NCLEX-RN® Examination (HESI Evolve Reach
Comprehensive Review f/ NCLEX-RN Examination) (Kindle Locations 4129-4142). Elsevier Health Sciences.
Kindle Edition.
[Show More]

.png)

 Med Surg test questions 06 Individual and Family Homeostasis, Stress, and Adaptation.png)
.png)
x.png)

![Preview of NUR2488 / NUR 2488 Exam 2 Study Guide [In Class Review] : Mental Health Nursing - Rasmuss](https://scholarfriends.com/storage/Mental Health Exam 2 Study Guide [In class review] MY21.png)


.png)



![Preview of NURS 6541 Week 7 Quiz [Completed A]](https://scholarfriends.com/storage/NURS 6541 Week 7 Quiz.png)