1
NR511 Final Exam
Study Guide
Week 1
1. Define diagnostic reasoning
-To solve problems, to promote health, and to screen for disease or illness all require a
sensitivity to complex stories, to contextual factors,
...
1
NR511 Final Exam
Study Guide
Week 1
1. Define diagnostic reasoning
-To solve problems, to promote health, and to screen for disease or illness all require a
sensitivity to complex stories, to contextual factors, and to a sense of probability and
uncertainty.
-Diagnostic reasoning can be seen as a kind of critical thinking. Critical thinking involves
the process of questioning one’s thinking to determine if all possible avenues have
been explored and if the conclusions that are being drawn are based on evidence.
Diagnostic reasoning then includes a systematic way of thinking that evaluates each
new piece of data as it either supports some diagnostic hypothesis or reduces the
likelihood of others.
2. Discuss and identify subjective & objective data
-Subjective:
-reports
-complains of
-tellscategory. Why is this so important? Well,
the MDM score gives us credit for the excess work involved in management of a more complex
patient.
15. Explain what a “well rounded” clinical experience means
-Includes both children from birth through young adult visits for well child and acute
visits, as well as adults for wellness and acute or routine visits
16. State the maximum number of hours that time can be spent “rounding” in a
facility
<25%
17. State 9 things that must be documented when inputting data into clinical
encounter
-date of service -visit E&M code (e.g., 99203) -age
-gender and ethnicity -chief concern -procedures
-tests performed or ordered -diagnoses -level of involvement
18. Identify and explain each part of the acronym SNAPPS
-S: Summarize
-N: Narrow
-A: Analyze
-P: Probe5
-P: Plan
-S: Self-directed learning
Week 2
1. Identify the most common type of pathogen responsible for acute gastroenteritis
-Viral: Norovirus (Leading cause for adults)
-Rotovirus (Leading cause for peds up to 2 years old)
2. Recognize that assessing for prior antibiotic use is a critical part of the history in
patients presenting with diarrhea
Due to risk of C Diff infection
3. Describe the difference between Irritable Bowel Disease (IBS) and Inflammatory
Bowel Disorder (IBD)
-IBS (Irritable bowel syndrome): disorder of bowel function not from anatomic abnormality
-constipation, diarrhea, bloating, urgency w/ diarrhea
-NOT assoc w/ serious medical consequences, IBD or CA
+S/S: result from disordered sensation or abnormal function of the small and
large bowel
-IBD (Inflammatory bowel disease): chronic immunologic disease that manifests in intestinal
inflammation
- UC/CD
4. Discuss two common Inflammatory Bowel Diseases
-Ulcerative colitis (UC): the mucosal surface of the colon is inflamed and ultimately results in
friability, erosions, and bleeding.
- Most common in recto-sigmoid colon. Can involve entire colon
- Pain in RLQ
-Crohns (CD): the inflammation extends deeper into the intestinal wall and can involve all or
any layer of the bowel wall and any portion of the GI tract from the mouth to the anus.
- Skipped lesions
- Pain in LLQ
5. Discuss the diagnosis of diverticulitis, risk factors, and treatments
Symptoms: LLQ pain/ tenderness, fever, N/V/D
Need imaging especially if perforation or peritonitis is suspected; free air = perforation;
patient may have ileus, small or large bowel obstruction
Can use plain x-ray6
CT or barium enema are preferred
CT with contrast is more sensitive and accurate
6. Identify the significance of Barrett’s esophagus
After repeated exposure to gastric contents, inflammation of the esophageal mucosa becomes
chronic.
· Blood flow increases, erosion occurs
· As erosion heals, normal squamous epithelium replaced with metaplastic columnar epithelium
containing goblet and columnar cells
· More resistant to acid and supports esophageal healing
· Premalignant tissue
· 40-fold risk for development of esophageal adenocarcinoma
· Fibrosis and scarring during healing of erosions; leads to strictures
7. Discuss the diagnosis of GERD, risk factors, and treatments
- Diagnosis made on history alone; sensitivity of 80%
- If symptoms are unclear/patient doesn’t respond to 4 weeks of empiric treatment
- Dx made by ambulatory esophageal pH monitoring
- pH < 4 above the lower esophageal sphincter and correlates with symptoms = GERD
- EGD with biopsy – Barrett’s esophagus
- Normal results in 50% of symptomatic patients
- Risks
o Obesity
o Increases after age 50
o Equal across gender, ethnic, and cultural groups
- Treatment
o Small, frequent meals – main meal at midday
o Avoid trigger foods
o No bedtime snacks; no eating < 4 hours prior to bed
o Eliminate caffeine
o Stop smoking
o Avoid tight fitting clothing
o Sleep with head elevated
- Medication:
o Step 1: antacids or OTC H2 (Tagamet, zantac, axid)
o Step 2: Rx-strength H2 (ranitidine 150mg BID, famotidine 20mg BID) or PPI
(pantoprazole 40mg daily, omeprazole 20mg daily)
o Step 3: PPI (omeprazole 40mg daily)
o Step 4: surgery (fundoplication)
8. Discuss the differential diagnosis of acute abdominal pain, work-up and testing,
treatments
Diff Diagnosis
Acute appendicitis:7
Inflammation of the vermiform appendix; due to obstruction or infection
Most common surgical emergency of the abdomen
Hollow tube – most common cause is obstruction of appendix
Fecaltih – hard lump of fecal matter
Undigested seeds
Pinworm infections
Lymphoid follicle growth/lymphoid hyperplasia Symptoms
4. Symptoms
Nausea/vomiting
RLQ pain
Guarding
Acute pancreatitis:
Sudden inflammation and hemorrhaging of the pancreas due to
destruction by its own digestive enzymes
1. Autodigestion
Most of the time mild, but can be severe
Pancreas
Cholescintigraphy (HIDA scan)
Radiolabeled marker used to visualize the biliary system
Acute cholecys – ducts are blocked, GB can’t be seen
Endoscopic Retrograde Cholangiopancreatography (ERCP)
Endoscope down to pancreas
Dye injected & viewed via fluoro
Magnetic Resonance Cholangiopancreatography (MRCP)
1. Visualizes bili system with MRI
Treatment:
Acute appendicitis:
Appendectomy
Antibiotic
Drain abscesses
Can be removed prophylactically
Acute pancreatitis:
o pain management
o hydration
o electrolytes
o rest bowels
NPO
IV nourishment
o Treat complications
O210
ATB
Acute cholecystitis:
o Supportive measures
IV
Pain management
ATB
o Surgical Removal
1. Cholecystectomy
1. Laparoscopic
9. Discuss the difference between sensorineural and conductive hearing loss
- Sensorineural: Results from deterioration of cochlea
-Loss of hair cells form the organ of Corti
-Gradual and progressive
-Not correctable but preventable
- Conductive: Obstruction between middle and outer ear
-Most types are reversible
10. Identify the triad of symptoms associated with Meniere's disease
-Meniere’s Disease: Sensory disorder of labyrinth (semi-circular canal system) and cochlea
-S/S:
-Vertigo
-Hearing loss
-Tinnitus
11. Identify the symptoms associated with peritonsilar abscess
-Increasing unilateral ear and throat pain ipsilateral to the affected tonsil
-Dysphagia
-Drooling
-Trismus
-Erythema
-Edema of the soft palate with fluctuance on palpation
12. Identify the most common cause of viral pharyngitis
-Adenovirus: MOST common -RSV
-Influenza A&B -Epstein-Barr
-coxsackie -enteroviruses
-herpes simplex11
13. Identify the most common cause of acute nausea & vomiting
Gastroenteritis
14. Discuss the importance of obtaining an abdominal xray to rule out perforation or
obstruction even though the diagnosis of diverticulitis can be made clinically
Abdominal xray films should be obtained on all patients with suspected diverticulitis to look for
free air (indicating perforation), ileus, or obstruction
15. Discuss colon cancer screening recommendations relative to certain populations
-Anyone over age 50 should have a routine c-scope
-African American’s should start screenings at age 40
-Individuals with a single first-degree relative with CRC or advanced adenomas diagnosed
at age ≥60 years can be screened like average-risk persons.
**Red flag symptoms should be sent to GI – unintentional weight loss, rectal bleeding,
diffuse lower abdomen pain, new onset diarrhea/constipation, early satiety, loss of appetite
16. Identify at least two disorders that are considered to be disorders related to
conductive hearing loss
-Chronic Otitis Media (OM)
-middle ear effusion
-mass
-vascular anomaly
-cholesteatoma – abnormal noncancerous skin growth in ear canal
17. Identify the most common bacterial cause of pharyngitis
-Group A Beta Hemolytic Streptococcus (GABHS)
-Absence of cough
-Tonsillar exudates
-History of fever
-Tender anterior cervical adenopathy
18. Identify the clinical findings associated with mononucleosis
-Fever -Malaise -Severe sore throat
-Exudative tonsillitis (50% of cases) -Palatal petchiae
-Rash -Anterior/posterior cervical lymphadenopathy12
-Splenic enlargement -POC Monospot test: (+)
19. Identify common characteristics in a rash caused be Group A Strep
Sandpaper rash
Fine, red, sparing hands & soles
20. Discuss that the diagnosis of streptococcal pharyngitis can be made clinically
based on the Centor criteria
-Absence of cough
-Tonsillar exudates
-History of fever
-Tender anterior cervical adenopathy
21. Describe an intervention for a patient with gastroenteritis
-Supportive care: fluid and nutrients
-Low residue diet (BRAT) – no evidence that this helps, but may be more tolerable for pt
-Viral cause = NO antibiotics
-Education surrounding not prescribing antibiotics/not spreading germs/eating safe foods
-Imodium/Zofran/Phenergan
22. Discuss an appropriate treatment for prophylaxis or treatment of traveler's
diarrhea
-empirical antimicrobial therapy: Trimethoprim-sulfamethoxazole (Bactrim) 1 PO BID ×3d
-ciprofloxacin (Cipro) 500 mg
-norfloxacin (Noroxin) 400 mg
-ofloxacin (Floxin) 300 mg
23. Identify at least one effective treatment for Irritable Bowel Syndrome (IBS)
- For IBS - C
o Psyllium (fiber)
o docusate (softner)
o bisacodyl/senna (stimulant/irritant)
o loperamide (antidiarrheal)
- For IBS – D
o dicyclomine (bentyl), hycosamine sulfate (Levsin) phenobarb/hycosamine
(donnatal)
anticholenergics – decrease motility of smooth muscle tone/decrease
cramping, relaxes muscles in stomach/intestines
o Linzess (linaclotide), Trulance (plecanatide), and Amitiza (lubiprostone):
drugs work by acting locally on the apical membrane of the GI tract to
increase intestinal fluid secretion and improve fecal transit13
- Antidepressants for depression/anxiety component
24. Identify at least one prescription medication for the treatment of chronic
confic factors- changes in weather, exercise,
environmental allergens, GERD, Beta blockers, sensitivity to ASA, strong emotional
expression
To establish the diagnosis of asthma, episodic symptoms of airflow obstruction must be
present, airflow obstruction must be at least partially reversible, and must rule out other
diagnoses.
Spirometry measurements are helpful in diagnosis & in evaluation of management
The diagnosis is made by demonstrating the reversibility of the airway obstruction from the preand post- PFTs.
Reversibility is defined as a 15% or greater increase in the FEV1 after 2 puffs of a betaadrenergic agonist have been inhaled.
When spirometry is non-diagnostic, bronchial provocation testing maybe useful with histamine,
methacholine, or exercise.
Risk Factors
Family or personal history- allergic rhinitis, eczema/atopic diseases
Residing in urban area
Exposure to smoke or air pollution
Cockroaches and dust
Viral respiratory infections
Cold air intolerance
obesity16
Classifications of Asthma Severity
Mild Intermittent Symptoms < 2 days per week OR < 2 nights per month. Exacerbations brief
Mild Persistent Symptoms > 2 times per week, but not daily; OR 3-4 times per month at
nighttime
Moderate
Persistent
Daily symptoms OR >1 night per week but not nightly
Severe persistent Symptoms throughout the day; often 7 nights per week
Pharmacological Management
*Short acting bronchodilator (albuterol) is a mainstay of treatment for ALL asthma patients
Intermittent Short-acting bronchodilator (albuterol): for exacerbations (inhaled or nebulized)
Mild Persistent Short acting bronchodilator +
Preferred tx- Low-dose inhaled corticosteroids (fluticasone/Flovent,
budesonide/Pulmicort, mometasone/asmanex
Moderate
Persistent
Short acting bronchodilator +
Preferred tx- low to medium dose inhaled corticosteroid AND
Long acting inhaled bronchodilator (salmeterol/serevent, formoterol/Foradil)
Alternative tx-low to med dose inh. Corticosteroid AND
Either leukotriene blocker (Montelukast/singulair) OR theophylline
Severe Persistent Short acting bronchodilator +
High dose inhaled corticosteroids AND
Long acting inhaled bronchodilator AND
If needed, oral corticosteroids (2mg/kg/day, 60mg/day max)
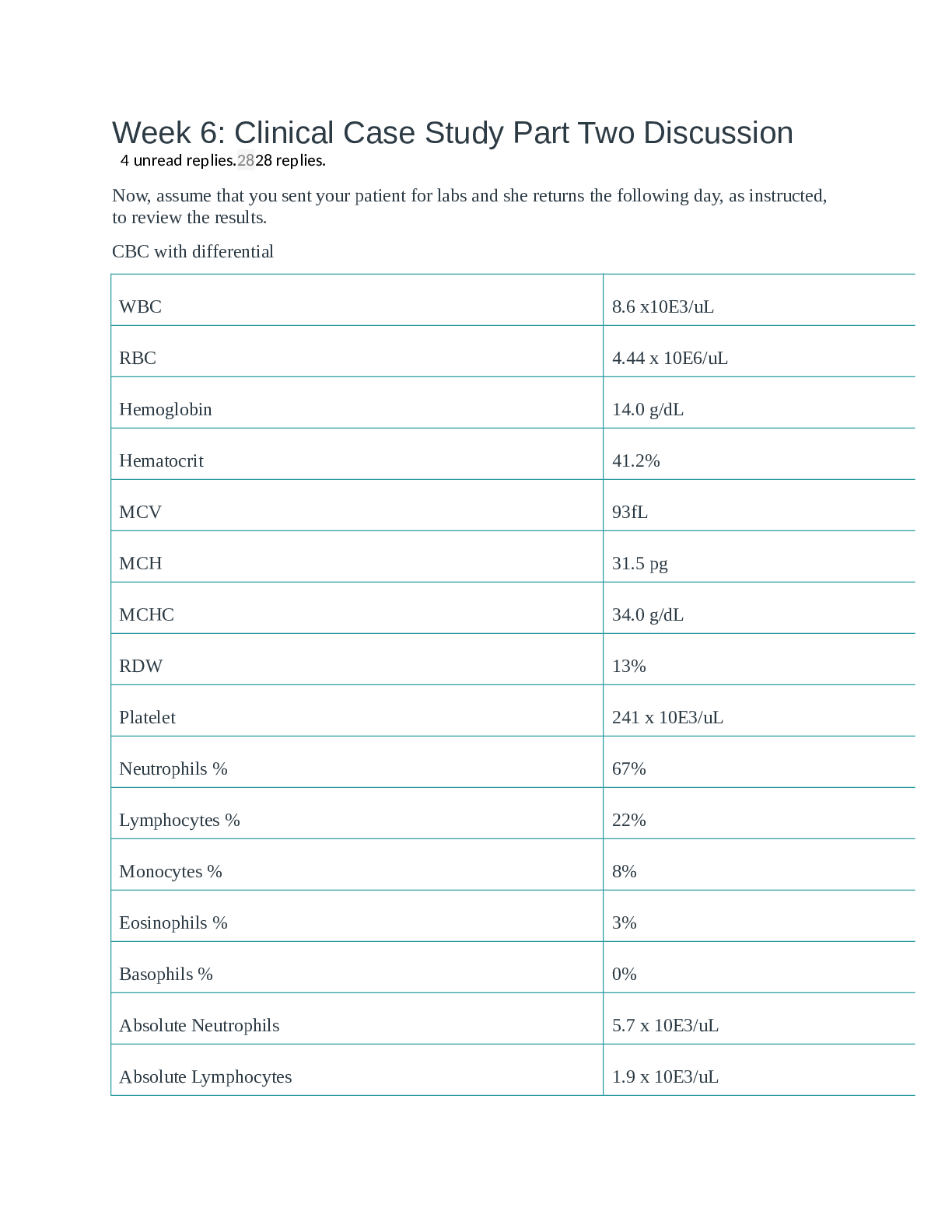
5. Describe appropriate tests in the work up for dyspnea
-CXR: rule out tumors, TB, pneumonia, and other major pulmonary disorders
-CBC with differential: rule out anemia and infection
-Peak expiratory flow test (in office): to determine the degree of expiratory airflow obstruction in
patients with asthma and COPD
-EKG, Echo
-Spirometry: to determine obstructive, restrictive and mixed lung disease
6. Discuss clinical findings and PFTs for asthma, chronic bronchitis, emphysema,
and COPD
- Asthma
o Subjective: c/o breathlessness, unable to talk, short sentences, profuse
sweating, c/o air hunger. In patients who are severely obstructed, there may
be no wheezing and only cough may be present. Wheezing, persistent and
recurrent cough, difficulty breathing, tightness in chest, endurance problems
during exercise. Symptoms are usually worse at night.17
o Objective: Nasal discharge, mucosal swelling, frontal tenderness, nasal
polyps, and allergic ―shiners‖ (dark discoloration beneath both eyes). Allergic
rhinitis and eczema often accompany the dx of asthma.
- Asthma PFTs
o Mild intermittent asthma- FEV1: >80%, PFT >20%
o Mild persistent asthma- FEV1: >80%, PFT 20%-30%
o Moderate persistent asthma- FEV1: 60%-80%, PFT >30%
o Severe persistent asthma- <60%, PFT >30%
- Chronic Bronchitis/Emphysema/COPD
o Subjective: frequent colds, persistent morning cough, upper respiratory
infectionsllowing tineas: pedis, cruris, corporis and unguium
and describe an appropriate treatment
Tinea Pedis: athletes foot
-Antifungal cream: -Ketaconozole for at least 4 weeks
-Tinea Cruris: Jock itch
-Topical antifungal
-Tinea corporis: Ring worm
-Topical antifungal cream
-Tinea unguium: onychomycosis: fungal infection of the fingernails or toenails
-topical agent: Ciclopirox nail laquer 8% applied daily for months at the base of the nail19
9. Identify the virus that causes warts
-HPV (Human papilloma virus)
10. Differentiate between atopic and contact dermatitis and give examples of each
-Contact Dermatitis: allergic reaction to a substance that produces an immune reaction in your
skin resulting in a very pruritic and erythemic rash
-Example: Poison Ivy
-Atopic dermatitis: a disorder that is the result of a gene variation that affects the skin’s ability to
retain moisture and protection from irritants
-Example: Eczema
11. Identify common characteristics associated with blepharitis, chalzion and
hordeolum
-Blepharitis: an inflammation around the eyelid margins that is caused by staphylococcal
infection at the lash bases and dysfunctional Meibomian glands
-Chalazion: a chronic internal granulomatous reaction of the Meibomian gland that produces a
mass in the lid
-Hordeolum: Stye: an abscess of the lid margin caused from a staph infection
12. Differentiate between viral, allergic, bacterial, toxic and HSV conjunctivitis
Bacterial: Pink eye: purulent discharge
-Viral: Adenovirus: watery or mucousy drainage: NOT purulent
-Allergic: environmental: uniquely identifying ―bumps‖ on the conjunctiva: follicles
-Toxic: Overuse of eye drops: clear/watery discharge/red conjunctiva
-HSV: Corneal infection with the hallmark ―dendrite‖ appearance
13. Discuss which chemical injury is associated with the most damage and highest
risk to vision loss
-Alkali injuries (moderate or severe) cause permanent scarring and vision loss
14. Recognize common eye emergency conditions that require emergency room
evaluation
-Orbital cellulitis -Chemical exposure
-Ruptured globe -Hyphema
-Foreign bodies -Moderate to severe subconjunctival hemorrhage
-Lid laceration20
15. Discuss glaucoma, diagnosis and treatment
Progressive damage to the optic nerve leading to atrophy and blindness.
Due to elevated intraoccular pressure
Open angle
More commonly seen chronic form
Good prognosis with treatment
S.sx
Typically asymptomatic until optic nerve damage
Slow gradual onset with slow painless bilateral peripheral vision loss
Poor night vision
Late s/sx
Halos around lights
Hardened eyeball
Marcus Gunn Pupil
Closed angle
Acute onset
S.sx
Rapid onset
Significant unilateral eye pain or pressure
Redness
Visual loss
Blurred vision
Photophobia
Halos around lights
Loss of peripheral vision followed by central vision loss
Headache
n/v
"Steamy" appearance to cornea
Pale optic disk with excavated cupping
If left untreated can lead to permanent vision loss.
PCP should closely monitor a family hx of glaucoma or hyperopia with eye ache,
headache, dry eye
Dx
Screening is the most important for PCP's
PCP s
new blood vessel proliferation
Dx
diagnosed by hx of DM >10 years and fundoscopic exam changes
Tx
first goal is prevention
Risk increases with BS >200
Keep HgbA1C <7%
Only medication shown to slow progressionACE inhibitor - lisinopril
Laser surgery if in proliferative stage 3 or significant macular edema22
Week 5
1. Identify the population most commonly affected by bacterial prostatitis
o Acute - Sexually active men 30 to 50 years
- Chronic bacterial prostatitis common in men older than 50 years old
- Athletes who run long distance are predisposed
- Complaints of fever, chills, LBP, malaise, arthralgia, myalgia, frequency, urgency,
dysuria, nocturia, and bladder outlet obstruction
o Chronic bacterial prostatitis- men over age 50 years of age. Symptoms often absent ,
perineal pain, lower abdomen pain, scrotal or penile pain, pain with ejaculation, dysuria,
irritative voiding
2. Discuss the physical exam characteristics of acute bacterial prostatitis
Abdominal exam to detect distended bladder, costovertebral angle tenderness, genital exam, and
digital rectal exam
Acute bacterial prostatitis- warm, tense, swollen , boggy and very tender prostate.
Most common pathogen Strep faecalis and staph aureus
3. Discuss how the Phren sign can differentiate between testicular torsion and
epididymitis
Epididymis characteristic is relief of discomfort with elevation of testis. Positive Prehn’s
sign = pain relief.
Testicular torsion elevation of the affected testicle does NOT relieve the pain (Negative
Prehn’s sign = pain is NOT relieved)
Epididymis Positive Prehn’s sign = pain relief. Neg = no pain relief = testicular torsion).
4. Discuss common symptoms reported from a patient with BPH
Affects men age 40 years and older.
Obstructive symptoms include
• Decreased stream • Hesitancy
• Postvoid dribbling • Sensation of incomplete bladder emptying
• Overflow incontinence • Inability to voluntarily stop the urine stream
• Urinary retention • Straining23
Irritative symptoms include
• Nocturia • Urinary frequency
• Urinary urgency • Dysuria
Urge incontinence
Erectile dysfunction should be assessed on patient taking finasteride.
5. Discuss the hallmark characteristic of a varicocele
The hallmark characteristic of varicocele is the sensation that the testes feel like a ―bag of
worms.‖
Varicocele can be bilateral, but if it is unilateral it is almost always on the left side due to the
anatomy of the vasculature drainage in the testes.
Tortuous veins posterior and above testes can be seen with patient sitting upright
Venous engorgement may increase with Valsalva maneuver; resolves when patient lies down.
Grade 1 varicocele is one that is palpable only when the patient performs the Valsalva
maneuver.
Grade 2 varicocele is palpable when the patient is standing.
Grade 3 varicocele may be assessed with light palpation and visual inspection
6. Identify the population most affected by testicular cancer
Males between the ages of 15 and 35
7. Explain spinal stenosis
Narrowing of the spinal canal w/ compression of nerve roots
- Congenital or acquired (age)
- Most commonly from enlarging osteophytes at the facet joints, hypertrophy of the
ligamentum flavum and protrusion/buldging of the intervertebral discs
- May produce symptoms by directly pushing on nerve or interrupting the blood
supply to nerve
Common source of chronic low back pain, seen most with aging. All older people have some
degree of this.24
8. Discuss common characteristics (subjective and objective findings) of patients
with lumbar spinal stenosis
Subjective
- Radicular complaints in calves, buttocks, upper thighs
- Pain w/ walking or prolonged standing
o Vascular claudication – pain stops w/ rest
o Psuedoclaskin,
alopecia, dry course thick hair
GI Diarrhea, Increase in BM Constipation, nausea,
hypoactive bowel sounds,
ascites, enlarged tongue
Eye Blurred vision, tearing, double
vision, decreased visual acuity,
photophobia, increased orbital
pressure, lid lag, exophthalmos,
corneal ulcer
N/A
Neurological Tremors in hands, hyperactive
reflexes
Memory deficits, personality
changes, hyporeflexia,
bradykinesia
Cardiopulmonary Palpitations, SOBOE,
tachycardia, HTN, CHF, A-Fib
Exercise intolerance,
bradycardia, cardiac
enlargement, pleural effusion
GU Decreased menstrual flow,
gynecomastia
Irregular menses, decreased
fertility
Head & Neck Increased neck size, enlarged
thyroid gland
Enlarged neck, enlarged tongue
(late), hoarseness
Psychosocial Anxiety, nervousness, insomnia,
irritability, restlessness,
emotional lability, Increase in
HR, RR, and BP
Depression, slowing of mental
processes
Musculoskeletal Weakness, loss of muscle tone,
Osteoporosis in women
Muscle weakness and cramping
Hematological Fatigue, normochromic
normocytic anemia28
16. Describe a goiter and the type of thyroid dysfunction that can be associated with
it
A goiter is the hypertrophy and hyperplasia of the thyroid gland in response to TSH levels.
Most commonly seen with Hashimoto’s thyroiditis (hypothyroidism) in the United States. Toxic
multinodular goiter (hyperthyroidism) in iodine deficiency. Grave’s Disease (hyperthyroidism)
has a firm goiter.
17. Differentiate between overt hypothyroidism and subclinical hypothyroidism
- Overt hypothyroidism
o TSH above 10 and FT4 is decreased
o Too little hormone is being produced
o Pituitary is attempting to get the thyroid to produce more
Low FT4 and high TSH
- Subclinical hypothyroidism
o TSH levels are increased, but the FT4 is within range
o Some have symptoms, others do not
18. Differentiate between Hashimoto’s thyroiditis and Grave’s disease
Both are autoimmune, attacking thyroid cells.
Graves – overproduction of thyroid leading to hyperthyroidism
- 90% of hyperthyroidism cases
Hashimoto’s – underproduction of thyroid leading to hypothyroidism
-Identified via TPO and TBG Abs in blood
19. Identify at least 3 risks associated with obesity
Diabetes, CVD, Afib, HTN, NSTEMI, varicosities, cancer, skin infections, arthritis
Gallbladder disease, GERD, acute pancreatitis, NAFLD
Stress incontinence, infertility, OSA
20. Identify at least 3 causes of obesity
Calorie excess—either overeating or high intake of carbohydrates
Food insecurity—eating from a fear of potential hunger or past experience with poor availability
of food on a regular basis
Genetic pre
-Persons with psychiatric disorders
(Dunphy, p. 847 & 859 and ―Thyroid Disorders‖ Lecture)
26. Discuss one physical characteristic seen in a hyperthyroid patient
-Smooth, velvety skin
-Soft, thin hair
-Skin with increased pigmentation, spider angiomas, and vitiligo
-Onycholysis (splitting and spooning of the nails)
-Exophthalmos (buldging eyes)
(Dunphy, p. 851 & Hollier, p. 231)
Muscle atrophy, tremors, hyperpigmentation, warm flushed moist skin, fine silky hair, thin hair,
increased LFT, Exopthalamos, lid lag and edema, corneal ulceration, sinus tach, elevated BP,
A.Fib, symptoms of CHF, gynecomastia, osteoporosis, hypercalcemia, potassium wasting31
27. Identify the CDC recommended antibiotic class for treatment of acute bacterial
prostatitis
-Flouroquinolones (Ciprofloxacin, levofloxacin, ofloxacin, or norfloxacin)
(Dunphy, p. 657 & ―Male GU Problems‖ Lecture)
Alternatives to a fluoroquinolone include
Doxycycline 100 mg Q 12 hours; and
TMP-SMX [160 mg/800 mg] (Bactrim DS) one tab Q 12 hours
28. Identify at least one treatment for BPH
-Medication (conservative):
-Alpha Blockers (Terazosin, Tamsulosin)
-5-alpha Reductase Inhibitors (finasteride, dutasteride)
-Surgical
-TURP (transurethral resection of the prostate)
29. Identify treatment options for obesity based on BMI and comorbid conditions
Overweight BMI: 25-29.9kg/m2
Obesity BMI: 30-40 kg/m2
Severe (morbid) obesity BMI: >40kg/m2
Treatment options: lifestyle changes (diet, exercise- 45-60 minutes/day), managing
behavior (i.e. H.A.L.T. – hungry, angry, lonely, tired, behavior modification), reduce caloric
intake, drugs (i.e. fenfluramine/Fen Phen, dexfenfluramine/Redux, phentermine,
diethylopropion, orlistat).
Surgical intervention (vertical-banded (mason) gastroplasty and roux-en-Y bypass) for
BMI over 40 OR over 35 with comorbities
A structured weight loss diet is most effective. Encourage formal programs or weight loss
groups (WW, etc.). Diet goals should include a program with
1200–1500 calories per day for women and 1500–1800 calories per day for men;
500–750 calorie deficit per day;
low CHO diet, increased fiber, and decreased saturated fats; and
less than 800 calories per day in certain circumstances under medical supervision.32
30. Describe the Spurling test and what condition it is used to diagnose
Spurling’s maneuver assesses nerve root compression (i.e. radiculopathy) in the neck resulting
in pain.
- Spurling’s maneuver:
o With patient’s neck in extension, rotate the neck to the affected side
o Apply downward pressure on the head
o Assess for patient complaint of or accentuation of limb pain or paresthesia
(THIS IS A POSITIVE SIGN). Also, observe for neck atrophy.
31. Describe how to perform a Phalen and Tinnel test
A. Phalen test:
Purpose: Assess for median nerve compression
Procedur
IV drug users
Healthcare workers
6. Describe at least one pharmacologic treatment option for tremor
Primidone (Mysoline) - beta blocker
benzodiazepine (lorazepam)
If monotherapy is ineffective, REFER TO NEURO
If the tremor is medication induced, that agent may be reduced or eliminated.
Parkinson’s disease
- Dopamine agonist
o Carbidopa/levodopa (Sinemet)
o Pramipexole (Mirapex)
o Ropinirole (Requip)
- Anticholenergics
o Benztropine (Cogentin)
o Trihexyphenidyl (Artane)
- If pharmacological therapy has been ineffective, localized botox injections may be
considered
- Deep brain stimulation in severe cases.
- If tremor is due to alcohol withdrawal: diazepam, lorazepam (mild symptoms)36
7. Describe an appropriate empiric antibiotic treatment plan for cellulitis
Cellulitis = bacterial infection
most commonly group A beta-hemolytic streptococcus or staphylococcus aureus (gram
positive)
tx = dicloxacillin or cephalexin for 10-14 days
if PCN allergy, erythromycin
If caused by animal or human bite: amoxicillin-clavulanic acid (augmentin) for 2 weeks
8. Discuss an intervention to prevent HIV and HIV-associated behaviors
*safe sex practices - latex condoms
*needle exchange programs
*universal testing of donated blood products
*education to HIV positive women of childbearing age about c-sections, arv drugs for mother
and baby
*voluntary HIV testing a routine part of medical care
*new models for HIV diagnosing outside medical setting
*prevent new infection by working with HIV infected and their partners to minimize risk
9. Identify physical exam findings in the patient with HIV
fever, sore throat, myalgia, headaches, cervical lymphadenopathy, night sweats, majority are
asymptomatic
flu-like sumptoms 6 days to 6 weeks after viral transmission
dark purple colored spots (karposi's sarcoma)
non-productive cough, SOB, and fever for several weeks
pulmonary symptoms: pcp pneumonia, tb, bacterial pneumonia
localized candida infections
other STD's
weight loss
anemia, leukopenia, and/or thrombocytopenia
10. Describe symptoms, DDx, pathogens, testing, and treatment for the following
conditions: Cellulitis, impetigo, MRSA, Bites (dogs, cats, humans), Erysipelas
- Cellulitis
o Pathogens
Strep (A,B,C,G,F)
Staph37
o Symptoms
Skin erythema, edema, warmth, pain, possible fever
Lymphangitis, lymphadenopathy, peau d’orange (orange peel texture)
No fever/chills, localized symptoms only
Underlying infection, lymphedema, venous insufficiency
o Treatment
I&D if abscess is involved
Patients with cellulitis should be managed with empiric therapy for infection
due to beta-hemolytic streptococci and methicillin-susceptible Staphylococcus
aureus (MSSA) with:
Cephalexin 500 mg four times daily (alternative for mild penicillin
allergy)
Clindamycin 300 mg to 450 mg four times daily (alternative for
severe penicillin allergy)
- Erysipelas
o Pathogens
Group A Strep
o Symptoms
Skin erythema, edema, warmth, pain, possible fever
Lymphangitis, lymphadenopathy, peau d’orange (orange peel texture)
Copiously irrigate with sterile saline
Remove grossly visible debris
Prophylactic ATB are given if
Deep puncture wounds
Wounds requiring surgical repair
Moderate to severe wounds w/ associated crush injury
Wounds in areas of underlying venous and/or lymphatic
compromise
Wounds on the hands or in close proximity to a bone or joint
Wounds on the face or in the genital area
Immunocompromised hosts
[Show More]






![Preview of NR667 Complete Question Bank with Correct Answers: Final Exam Study Guide [2026 Updated]](https://browseimages.nyc3.digitaloceanspaces.com/paper-images/2026/02/25/AULA53fD2026-02-25-02-58699ee3d811bc7.png)