Medsurg Hesi Topics
1. Nursing process-Stroke TIA: Med-Surg book p930-945 lot of pages just hitting the
highlights.........TIA = Transient ischemic attack. TEMPORAY neurologic dysfunction resulting from
a brief interr
...
Medsurg Hesi Topics
1. Nursing process-Stroke TIA: Med-Surg book p930-945 lot of pages just hitting the
highlights.........TIA = Transient ischemic attack. TEMPORAY neurologic dysfunction resulting from
a brief interruption in cerebral blood flow. Typically resolves in 30 to 60 min. Treatment focuses
on preventing another TIA or stroke: Reducing high BP, the most common risk factor for stroke,
by adding or adjusting drugs to lower BPTaking aspirin or another antiplatelet drug to prevent
strokes (Plavix) Controlling diabetes and keeping blood sugar levels in a target range, typically
100-180mg/dl Promoting lifestyle changes such as quitting smoking, eating heart-healthy
foods, and being more active Ensure that the pt taking antiplatelet drugs is aware of precautions
and actions to take if bleeding occurs. A Stroke - Is a medical emergency, and it should be treated
immediately to reduce permanent disability. It is caused by an interruption of perfusion to any
part of the brain. Recommend a diet high in fruits and veggies and low in saturated fats. Light to
moderate alcohol consumption may reduce the risk for stroke, but a higher consumption may
increase it. NCLEX purple book p225, 937-939 1.In clients with hemorrhagic strokes, the head of
the bed is usually elevated to 30 degrees to reduce intracranial pressure and to facilitate venous
drainage. 2.For clients with ischemic strokes, the head of the bed is usually kept flat 3.Maintain
the head in a midline, neutral position to facilitate venous drainage from the head. 4.Avoid
extreme hip and neck flexion; extreme hip flexion may increase intrathoracic pressure, whereas
extreme neck flexion prohibits venous drainage from the brain ALERT! A critical factor in the
early intervention and treatment of stroke is the accurate identification of stroke manifestations
and establishing the onset of the manifestations. Stroke screening scales may be used to quickly
identify stroke manifestations. Box 66-17 Neurological Assessment in Stroke: Changes in level of
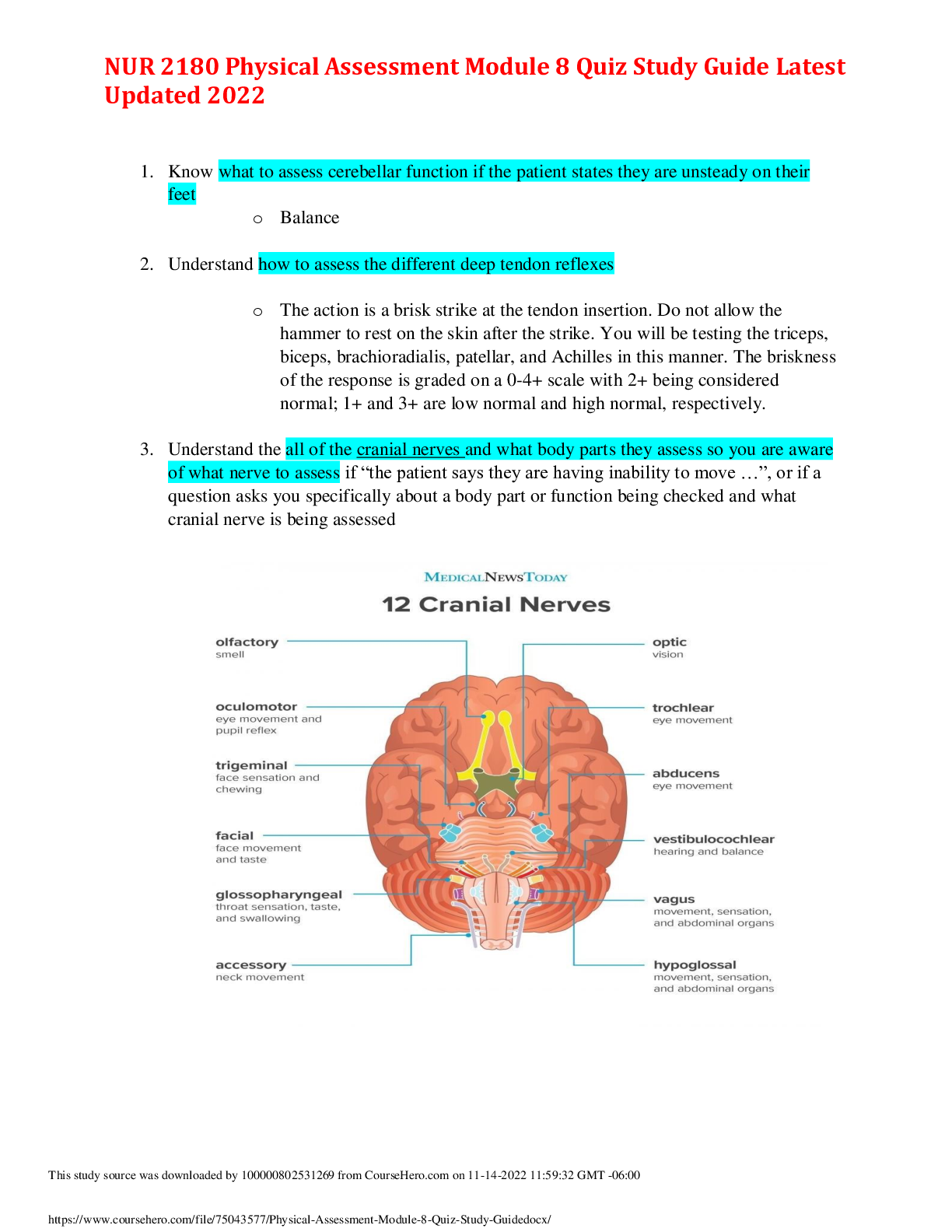
consciousness Signs of increasing intracranial pressure Assessment of cranial nerves V, VII, IX,
X and XII Cranial nerve V: Difficulty with chewing Cranial nerve VII: Facial paralysis or paresis
Cranial nerve IX and X: Dysphagia Cranial nerve IX: Absent gag reflex
Cranial nerve XII: Impaired tongue movement Review box 66-18 Assessmnet findings in a stroke
HESI green book p 144-146HESI HINT– CNS involvement related to cause of stroke:
Hemorrhagic: caused by a slow or fast hemorrhage into the brain tissue; often related to HTN
Emoblic: Caused by a clot that has broken away from a vessel and has lodged in one of the
arteries of the brain, blocking the blood supply. It is often related to atherosclerosis (so it may
occur again). HESI HINT– Atrial flutter and fibrillation produce a high incidence of thrombus
formation following dysrhythmia caused by turbulence of blood flow through all valves and
heart chambers. HESI HINT– A woman who had a stroke 2 days earlier has left-sided paralysis.
She has begun to regain some movement in her left side. What can the nurse tell the family
about the client’s recovery period? The quicker movement is recovered, the better the
prognosis is for full or improved recovery. She will need patience and understanding from her
family as she tried to cope with the stroke. Mood swings can be expected during the recovery
period, and bouts of depression and tearfulness are likely.See table 4-35 Location of disruption
in the brain p145 HESI HINT– Words that describe losses in strokes: 1.Apraxia: inability to
perform purposeful movements in the absence of motor problems 2.Dysarthria: difficulty
articulating 3.Dysphasia: impairment of speech and verbal comprehension 4.Aphasia: loss of
the ability to speak 5.Agraphia: loss of the ability to write 6.Alexia: loss of the ability to read
7.Dysphagia: dysfunctional swallowing HESI HINT– Steroids are administered after a stroke to
decrease cerebral edema and retard permanent disability. H2 inhibitors are administered to
prevent peptic ulcers
2. Vitamins and herbs, outcomes/nursing action/constipation-diarrhea:
3. Operative nutrition/ healing: Hesi green book p169, 170 8. Provide proper nutrition (BURN
patients):a.Maintain NPO status until bowel sounds are heard and then advance to clear liquids as
prescribed b.Provide a diet high in protein, carbohydrates, fats and vitamins c.Monitor caloric intake ***
Monitor hydration status: Record urinary output hourly (30/100 mL/hr is normal range). Maintain IV
fluids titrated to keep urine output at 30 to 100 mL/hr. accurately record I&O. Weigh daily. *** 5. Provide
adequate nutrition. a. Provide high-calorie (up to 5000 calories/day), high-protein, high-carbohydrate
diet.b. Give national supplements via NG tube feeding at night if caloric intake is inadequate. c. Keep
accurate calorie counts. d. Administer all medications with either milk or juice. e. May require total
parenteral nutrition (TPN). f. Weigh daily. NCLEX purple book p83,84 Monitoring of enteral feedings
and the client’s ability to tolerate feedings Monitoring of nutritional intake and oral hydration P572
ALERT! – Avoid the IM or SubQ medication route for meds administration because absorption through
the soft tissue is unreliable when hypovolemia and large fluid shifts occur. Nutrition a.Proper nutrition is
essential to promote wound healing and prevent infection. b.The basal metabolic rate is 40 to 100 times
higher than normal with a burn injury c.Maintain NPO status until bowel sounds are heard, and then
advance to clear liquids as prescribedd.Nutrition may be provided via enteral tube feeding or parenteral
nutrition through a central line e.Provide a diet high in protein, carbohydrates, fats, and vitamins
f.Monitor calorie intake Med-Surg book p486, 487 Nutrition requirements for a patient with a large burn
area can exceed 5000 kcal/day. Not meeting this need leads to very rapid weight loss. In addition to highcalorie intake, a diet high in protein is needed for wound healing. Work with the dietitian and the patient
to plan additions to standard nutrition patterns. Encourage pts who can eat solid food to ingest as many
calories as possible. Offer frequent high-calorie, high-protein supplemental feedings. Keep an accurate
calorie count for foods and beverages that are actually ingested by the pt. P542 Nutrition with pts who
had head and neck cancer surgery: A nasogastric, gastrostomy, or jejunostomy tube is placed during
surgery for nutrition support while the head and neck heal. After the intestinal tract is motile, nutrients
can be given via the feeding tube. The nutrition support team or dietitian assesses the pt before surgery
and is available for consultation after surgery. Replacement of calories, protein, and water loss is
calculated carefully for each pt. The feeding tube usually remains in place for 7 to 10 days after surgery.
Before removing the tube, assess the pts ability to swallow if nutrition is to be given by mouth.
Aspiration CANNOT occur after a total laryngectomy because the airway is completely separated from
the esophagus. Stay with the pt during the first few swallowing attempts. Swallowing may be
uncomfortable at first, and analgesics may be needed. ** review Chart 29-3 Prevention of Aspiration
during swallowing on p543 P436 Table 25-2 Causes of Impaired wound healing: Nutritional deficiencies
–Calories Protein Vitamins Minerals Water P438 Nutrition for preventing pressure ulcers: Ensure
a fluid intake between 2000 and 3000 mL /day Help the pt maintain an adequate intake of protein and
calories P440 High risk pts, impaired mobility: Nutrition status is a critical risk factor or pressure ulcer
development and for successful healing. Tissue integrity and would healing depend on a positive
nitrogen balance and adequate serum protein levels. Draining wounds contribute to protein loss and
require aggressive intervention. Nutrition is considered inadequate when the serum pre-albumin level is
less than 19.5 g/dL, albumin level is less than 3.5 g/dL, or the lymphocyte count is less than 1800/mm3.
P446 Nutrition Therapy: Severe protein deficiency inhibits healing and impairs host infection defenses.
SEE Table 60-2 p1239 Manifestations of Nutrient Deficiencies ********** This table would be great for
HESI TOPIC #2!!!! As it says which vitamin causes what deficiency ********** P1239,1240 Providing
high-calorie, nutrient-rich foods (milkshakes, cheese, supplements, drinks like Boost or Ensure. A feeding
schedule of six small meals may be tolerated better than three.
** Review chart 60-3 Promoting Nutrition Intake ** P1325 Regarding the Diabetic patient : Pts requiring
clear of full liquid diets should receive about 200 g of carbohydrate daily in equally divided amounts at
meals and snack times. After surgery, food intake is initiated as quickly as possible with progression from
clear liquids to solid foods occurring as rapidly as tolerated. Returning to a normal meal plan as soon as
possible after surgery promotes healing and metabolic balance. If TPN is used after surgery, severe
hyperglycemia may occur. Monitor blood glucose often to determine the need for supplemental insulin.
4. Cirrhosis / edema: It is extensive, irreversible scarring of the liver, usually caused by chronic reaction
to hepatic inflammation and necrosis. Common causes are alcoholism, viral hepatitis, nonalcoholic
steatohepatitis, bile duct disease, and genetic diseases. Ascites is the collection of free fluid within the
peritoneal cavity caused by increased hydrostatic pressure from portal hypertension. It causes a type of
3
rd spacing which has edema and hypovolemia. Ascites is considered edema. Hesi 106-108 Saunder 695
[Show More]
![Preview of Medsurg Hesi Topics.docx[VERIFIED100%]](https://scholarfriends.com/storage/docx (82).png)





![Preview of Western Governors University[C468 Informatics Study Guide]](https://scholarfriends.com/storage/C468_Study_Guide_2020.png)

.png)
![Preview of Focused Exam_ Pediatric GAS Pharyngitis Transcript[latest 2021]](https://scholarfriends.com/storage/Focused_Exam__Pediatric_GAS_Pharyngitis_Transcript.png)
![Preview of Galen College of Nursing [NUR 242 Exam 4 Study Guidelines rated A]](https://scholarfriends.com/storage/Nur_242_Exam_4_study_guide.png)