NURSING > CASE STUDY > NURS 501 Labor and Delivery Case Study Cindy (All)
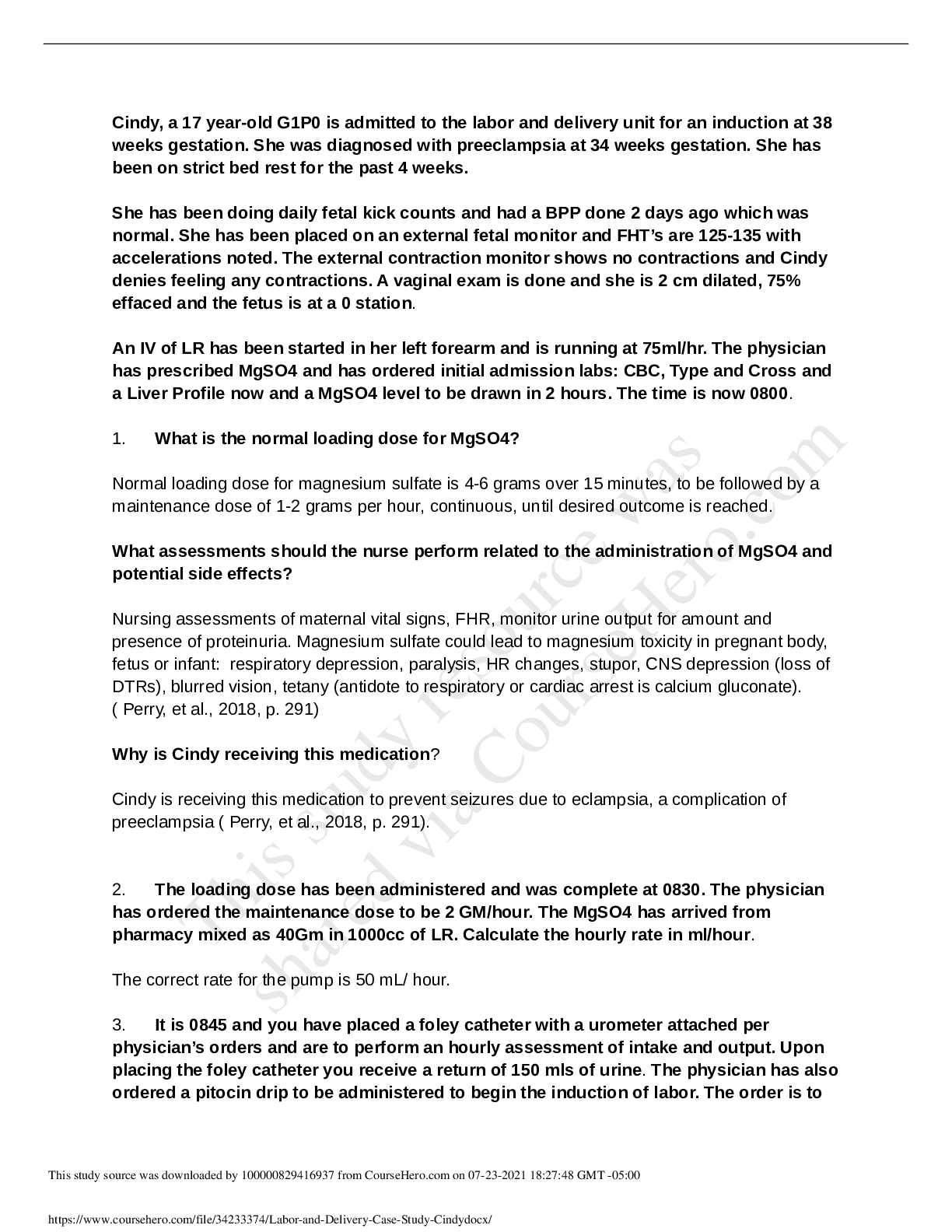
NURS 501 Labor and Delivery Case Study Cindy
Document Content and Description Below
Last updated: 3 years ago
Preview 1 out of 4 pages
Instant download
Buy this Document to get the Full Access Instantly
Provided by Students Who Aced it
We Verify Document Content to Gurantee Accuracy
Reviews( 0 )
Document information
Connected school, study & course
About the document
Uploaded On
Jul 24, 2021
Number of pages
4
Written in
All

Additional information
This document has been written for:
Uploaded
Jul 24, 2021
Downloads
0
Views
97
Document Keyword Tags
Recommended For You
Get more on CASE STUDY »
NURS 501 ADVANCED PHYSIOLOGY AND PATHOPHYSIOLOGY : Ultimate Te...

NURS 501 Advanced Physiology and Pathophysiology Chapter 3 Flu...

501 Study Guides NURS 501 Advanced Physiology and Pathophysiol...

NURS 501 Advanced Physiology and Pathophysiology STUDY GUIDE
NURS 501 ADVANCED PHYSIOLOGY AND PATHOPHYSIOLOGY (A GUARANTE...
NURS 501final guide GRADED A document. download to passing
NURS 501 Advanced Physiology and Pathophysiology Chapter 1-11...

NURS 501 ADVANCED PHYSIOLOGY AND PATHOPHYSIOLOGY (ASSURED A)...
NURS 501 Advanced Physiology and Pathophysiology STUDY GUIDE S...
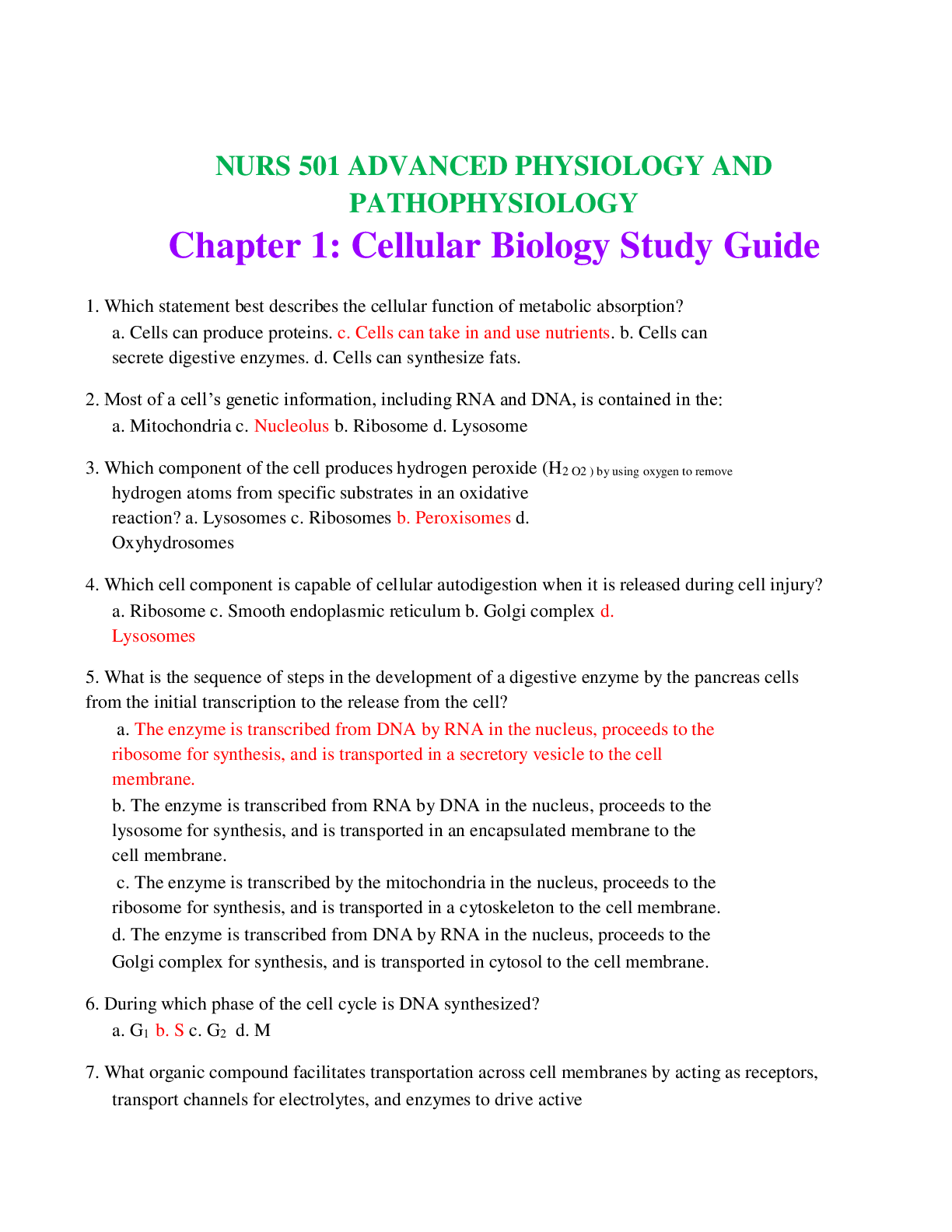
NURS 501 Advanced Physiology and Pathophysiology Chapter 1: Ce...
NURS 501 Advanced Physiology and Pathophysiology Chapter 1: C...
NURS 501 Advanced Physiology and Pathophysiology (All Chapter...

.png)



 (1).png)

.png)