NUR 3032 Pathophysiology Exam 1 Study Guide Latest updated
CHAPTER 5:
Cellular Adaptation:
• Cells adapt to changes in the internal environment when confronted with stress that endanger normal structure and func
...
NUR 3032 Pathophysiology Exam 1 Study Guide Latest updated
CHAPTER 5:
Cellular Adaptation:
• Cells adapt to changes in the internal environment when confronted with stress that endanger normal structure and function. These cells adapt to increase work demands by changing in:
1. Size (Atrophy and Hypertrophy)
2. Number (Hyperplasia)
3. Form (Metaplasia)
• These mechanisms depend largely on signals transmitted by chemical messengers that exert their affects by altering gene function. In general, the genes are expressed in two categories:
1. Operating genes that are necessary for normal function of a cell
2. Genes that determine the differentiating characteristics of a particular cell type
• In many adaptive cellular responses, the expression of the differentiation genes is altered but that of the operating genes remains unaffected. Thus, a cell is able to change size or form without compromising its normal function. Once the stimulus for adaptation is removed, the effect on expression of the differentiating genes is removed and the cell resumes its previous state of specialized function.
• Whether the adaptive cellular changes are normal or abnormal depends on whether the response was mediated by an appropriate stimulus
• Some adaptive changes include:
1. Intracellular accumulations
2. Storage of products in abnormal amounts
Lecture Notes:
• Anything that’s genetic can change the cell. Radiation as well. Any external factor. Cell injury can occur from genetic, chemical, immunoglobin or x-rays, etc. As a result you can have several different changes.
• Free Radicals: when the cells do not have an enough amount of electrons and protons therefore free ions are migrating because they don’t have a pair so it makes the cell at risk for more injury to occur.
o EX: if you have a negative and a positive and they are unpaired they are going to cause free radicals.
o These free radicals can also happen with radiation.
• Cells adapt with changes in their size, number and form.
Atrophy:
• Atrophy is a decrease in cell size
• EX: When you go regularly to the gym, and then all of a sudden you stop your muscles are going to atrophy, meaning they are going to decrease in size.
• When confronted with a decrease in word demands or adverse environmental conditions, most cells cam decrease in size in order to have a lower yet more efficient level of functioning that is compatible with their survival
• Causes of atrophy include:
1. Disuse: reduction in skeletal muscle use. EX: muscles of extremities that have been encased in plaster cast. Since atrophy is adaptive and reversible, the muscle size can be restored when cast is removed.
2. Denervation: a type of muscle atrophy that occurs in the muscles of paralyzed limbs.
3. Loss of endocrine stimulation: loss of estrogen stimulation during menopause results in atrophic changes in the reproductive organs.
4. Inadequate nutrition
5. Ischemia or decrease blood flow
• With Malnutrition and decreased blood flow, cells decrease their size and energy requirements as a means of survival.
• Cells that are atrophies reduce their oxygen consumption and other cellular functions by decreasing the number and size of their organelles and other structures.
• EX: cell size in muscle tissue is related to work load. As the work load of a cell declines, oxygen consumption and protein synthesis will both decrease
• Insulin levels and insulin growth factor-1 is what maintains proper muscle mass. If these levels are low or catabolic signals are present, the muscle atrophy occurs by mechanisms
that reduce synthetic processes, increased proteolysis by the ubiquitin proteasome system and apoptosis or cell death.
Lecture Notes:
• Ischemia: anything that causes hypoxia or decreased oxygenation to an organ.
o EX: ischemia to the brain will cause a stroke
• Atrophy can be both pathological (disease causing) and physiological (something normal).
• Physiological atrophy:
o EX: the thymus. As we get older, our thymus shrinks naturally. It doesn’t mean there is something wrong, its just normal a normal physiological response.
o EX: the adenoids. You can remove them and be completely okay without them.
• Pathological atrophy:
o EX: a spinal cord injury and its cause from a trauma
o EX: paralytic, extremities will become smaller, you wont use your muscles as much, no blood flow
Hypertrophy:
• Hypertrophy is an increase in cell size and also with it an increase in the amount of functioning use of tissue mass.
• IMP: Left ventricular hypertrophy is caused by uncontrolled long term hypertension.
• Results from an increased workload imposed on an organ or body part and is commonly seen in cardiac and skeletal muscle tissue, which CANNOT adapt to an increase in workload through mitotic division and formation of cells.
• Hypertrophy can result from a normal physiologic condition or an abnormal physiologic condition.
1. Physiologic hypertrophy: increases in muscle mass associated with exercise.
2. Pathologic hypertrophy: occurs as a result of disease conditions that can be either adaptive or compensatory.
• Hypertrophy can occur as a result of disease conditions and can either be:
1. Adaptive: an example is the thickening of the urinary bladder from long continued obstruction of the urinary outflow and the myocardial hypertrophy that results from vascular heart disease or hypertension.
2. Compensatory: an example would be the enlargement of a remaining organ or tissue after a portion has been surgically removed or rendered inactive. An example of this is one of the kidneys are removed; the other becomes enlarged to compensate for the other kidney.
• Signals of hypertrophy appear to be complex and related to ATP depletion, mechanical forces such as stretching of the muscle fibers, activation of cell degradation products and hormonal factors.
Hyperplasia:
• Hyperplasia refers to an increase in the number of cells in an organ or tissue. Occurs in tissues with cells that are capable of mitotic division.
o EX: Epidermis, interstitial epithelium, and glandular tissue
• Evidence suggests that hyperplasia involves activation of genes controlling cell proliferation and the presence of intracellular messengers that control cell replication and growth.
• Normal response: hyperplasia is controlled in response to an appropriate stimulus and ceases after the stimulus has been removed.
• The stimulus that induce hyperplasia may be physiologic or non-physiologic:
1. Physiologic: hormonal and compensatory.
o EX: hormonal would be the breast and uterine enlargements during pregnancy are examples of physiologic hyperplasia that result from estrogen stimulation.
o EX: compensatory would be when the liver regenerates after having a part removed.
• Although hypertrophy and hyperplasia are two distinct processes, they may occur together and are often triggered by the same mechanism.
• Non-physiologic: due to excessive hormonal stimulation or the effects of growth factors on target tissues.
o Endometrial hyperplasia is caused by excess estrogen and leads to abnormal menstrual bleeding. It is considered high risk for developing endometrial cancer.
• Prostatic hyperplasia: common disorder found in men older than 50 years of age, related to the action of androgens. Causes lower urinary tract infections and are non- malignant.
Lecture Notes:
• Plasia refers to the amount of cells NOT the size.
• Hyper= a lot of cells
• Not very common
• So many cells start to grow and the patient starts growing taller and their jaws get bigger and their hormones are increased gigantism
• Liver regeneration can be a positive thing fro hyperplasia
Metaplasia:
• Reversible change in which one adult cell type is replaced by another adult cell type.
• Occurs in response to chronic irritation and inflammation and allows for substitution of cells that are better able to survive under circumstances in which a more fragile cell type might succumb.
• Stratified squamous epithelium is replacing the ciliated columnar epithelial cells in the trachea and large airways of smoker.
• Barrett esophagus: premalignant condition that occurs in the esophagus of people with chronic gastro esophageal reflux disease (GERD). It is a character by normal squamous epithelium in the lower esophagus transforming into columnar-lined epithelium. This is the primary risk for developing esophageal adenocarcinoma.
Lecture Notes:
• Cigarette smoking is the most common… the good cells become replaced by an immature cell. The change in cell is from the actual smoking. This does not mean cancer but it puts them in a much higher risk of cancer.
• Metaplasia can ultimately become malignant.
Dysplasia:
• Characterized by deranged cell growth of a specific tissue that results in cells that vary in size, shape and organization.
• Associated with chromic inflammation and irritation.
• The pattern is most frequently encountered in areas of metaplastic squamous epithelium of the respiratory tract and uterine cervix.
• Although dysplasia is adaptive, it is potentially reversible after the irritation has been removed.
• This is an implication of a strong precursor of cancer, In cancers of the respiratory tract and uterine cervix, dysplastic changes have been found adjacent to the foci of cancerous transformation.
o PAP smears have shown that epithelial changes range from severe dysplasia to invasive cancer. Yet dysplasia is adaptive and does not necessarily lead to cancer.
• Bronchopulmonary dysplasia (BPD): pre term babies that have been ventilated for long period of time due to their prematurity and lack of surfactant or term infants that require intubation and ventilated oxygen in the first month of life tend to have this.
o More preterm babies survive therefore there is more BPD.
o Many infants with BPD end up having long-term alveolar destruction for the rest of their lives.
• Skin warts are another example caused by growth factors produced by viruses.
Lecture Notes:
• Dysplasia: disorganized irregular cell growth. Also at risk for malignancy
• PAP smears are important because they work you up for HPV in the cervical area. HPV is the number one cause for cervical cancer.
Intracellular accumulation:
• Intracellular accumulations represent the build up of substances that cells cannot immediately use or eliminate. These substances can accumulate in the cytoplasm or nucleus.
• There are 3 sources of intracellular accumulation:
1. Normal body substances: lipids, proteins, carbohydrates, melanin
2. Abnormal endogenous products: those resulting from inborn errors of metabolism
3. Exogenous products: environmental agents and pigments not broken down by the cell
• Accumulation of normal cellular constituents occurs when a substance is produced at a
rate that exceeds its metabolism or removal.
o EX: fatty changes in the liver due to intracellular accumulation of triglycerides.
o Abnormal accumulation occurs when the delivery of fatty acids in the liver is increase, as in starvation and diabetes mellitus, or when the intrahepatic metabolism of lipids is disturbed.
• Jaundice: yellow dis-coloration of tissue due to the retention of bilirubin, and endogenous bile pigment. This condition may result from an increased bilirubin production from red blood cell destruction, obstruction of a bile passage into the intestine, or toxic diseases that affect the livers ability to remove bilirubin from the blood. (ENDOGENOUS EXAMPLE)
• Carbon in the form of coal dust. Miners or people exposed to heavy polluted environments accumulate carbon dust that blackens the lung tissue and may cause serious lung disease. (EXOGENOUS EXAMPLE)
Lecture Notes:
• Intracellular accumulation is also known as infiltration
• It is basically an accumulation of genetic sources or toxins. What it does is it disorganizes the cell structure.
• An example of this would be somebody that has paint intoxication, uric acid buildup, or gout pacification. Normal body substances such as triglycerides can cause intracellular accumulations.
• This becomes a problem when there is too much intracellular accumulation. We need protein for muscles build up and carbohydrates for energy.
• Jaundice- caused by abnormal hemolysis of red blood cells.
• Overall, the major problem is when there is too much!!!
QUESTION: Which of the following best describes the cellular adaptation seen in chronic cigarette smokers?
ANSWER: Metaplasia. As cells are damaged, a hardier version replaces the normal strata of cells.
Pathological Calcifications:
• Abnormal tissue deposition of calcium salts, together with smaller amounts of iron, magnesium and other mineral.
• There are two types:
1. Dystrophic calcification: when it occurs in dead or dying tissue
o Dystrophic calcification represents the macroscopic deposition of calcium salts in injured tissue. It can be visible to the naked eye.
o This involves the intracellular or extracellular formation of crystalline calcium phosphate.
o The components of the calcium are derived from the bodies of dead or dying cells as well as from the circulation and intestinal fluid.
o This is commonly seen in athermanous lesions of advanced atherosclerosis, areas of injury to the aorta, large blood vessels, and damaged heart valves.
2. Metastatic calcification: when it occurs in normal tissue
o Occurs as a result of increased serum calcium levels (Hypercalcemia). Almost any condition that increases these levels can lead to calcification in inappropriate sites.
o Paget Disease: a type of breast cancer (ex on the nipple)
Lecture Notes:
• Dystrophic calcification: when valves become calcified, the cardiac output would become compromised. Regurgitation or decreased cardiac output.
• Metastatic calcification: something referring to cancer.
• Hypercalcemia: high levels of calcium therefore the patient needs to be worked up for cancer.
QUESTION: Is the following statement true or false? Dystrophic calcification can result from prolonged ischemia.
ANSWER: True. Ischemia stresses the tissue, it dies, and calcium precipitates out of solution.
***Ischemia is low O2 and hypoxia***
***Ischemia EX: edema, having edema will mean you have liquid… for example in the arm, liquid in the arm will cause constriction of the vessels putting stress to the extremities***
Causes of cell injury:
1. Injury from physical agents:
o Mechanical forces: trauma from body impact with another object. These injuries split and tear tissues, fracture bones, injure blood vessels, and disrupt blood flow.
o Extremes of temperature: too hot or too cold temperatures
o Electrical forces: affects the body through extensive tissue injury and disruption of neural and cardiac impulses. Alternating current is more dangerous than direct current because it causes violent muscle contractions, preventing the person from releasing the electrical source and sometimes results in fractures/dislocation. Can cause fatal cardiac arrhythmias.
2. Radiation injury:
o Ionizing radiation: releases free radicals and destroy the cells and by directly hitting the target molecules in the cell. Can result in increased risks of cancers. Directly breaks chemical bonds.
o Ultraviolet radiation: causes sunburn and increases the risk of skin cancer.
o Nonionizing radiation: infrared light, ultrasound, microwaves, and lase energy. Causes vibration and rotation of atoms and molecules that is then converted to thermal energy. Used widely in television, microwaves, etc.
3. Chemical injury:
o Drugs: alcohol can harm the gastric mucosa, liver, developing fetus and other organs. Other drugs produce metabolic end products that are toxic to cells. When large amounts of drugs are ingested, the pathways become overwhelmed and toxic metabolites accumulate causing massive liver necrosis.
o Carbon tetrachloride: causes little damage until it is metabolized by liver enzymes to a highly reactive free radical and can be extremely toxic to liver cells.
o Lead toxicity: a deficiency in calcium, iron or zinc increases lead absorption. In children most lead is absorbed through the lungs and they are more vulnerable to toxicity. Lead has the ability to inactive enzymes, compete with calcium for incorporation into bone, and interfere with nerve transmission and brain development. The major targets of lead toxicity are red blood cells, GI tract, kidneys and the nervous system
o Mercury: toxicity involves the central nervous system and the kidney. Some fish have a large concentration of mercury.
4. Injury from biologic agent:
o Virus, parasites, and bacteria: viruses take over a host and incorporate its own DNA. Certain bacteria elaborate exotoxins that interfere with cellular production of ATP. Other bacteria, release endotoxins that cause cell injury and increased capillary permeability.
5. Injury from nutritional imbalances:
o Excess and deficiencies: obesity and diets high in saturated fats are though to predispose people atherosclerosis. Dietary deficiencies can occur in the form of starvation, or because of a selective deficiency of a single nutrient or vitamin.
o EX: iron deficiency anemia. The protein and calorie deficiencies that occur with starvation cause widespread tissue damage.
Lecture Notes:
• When your cold your blood will thicken and vessel constrict and flow is going to be slow because of the viscosity in the blood. This puts patients at risk for blood clots and hypoxia so oxygen is perfused to organs. ENVIROMENT PLAYS A BIG ROLE!
• Iron deficiency anemia will manifest issues with perfusion. Too much or too little. Both cause cell injury.
• Very hard to treat a thermal injury because you are not aware of damage on the inside. (EX: thermal injury can be like a burn)
Mechanisms of Cell Injury:
• Free radical and reactive oxygen species (ROS) formation
o Free radicals are highly reactive chemical species; having an unpaired electron causes them to be unstable and highly reactive.
o Free radicals can establish a chain of events that generate new free radicals.
o In cells and tissues, free radicals react with proteins, lipids, carbohydrates, and therefore cause damage to the cell membrane, can inactive enzymes, and damage nucleic acids that make up DNA.
o Reactive oxygen species (ROS): molecules that include free radicals such as superoxide and hydroxyl radical and non-radicals such as hydrogen peroxide. These molecules are produced endogenously by normal metabolic processes or cell activities, such as the metabolic burst that accompanies phagocytosis.
o Exogenous causes including ionizing and UV radiation can cause ROS production.
o Antioxidants: natural and synthetic molecules that inhibit the reaction of ROS with biologic structures or prevent the uncontrolled formation of ROS.
• Free radical injury
1. Lipid peroxidation
2. Oxidative modifications of proteins
3. DNA effects
Lecture Notes:
• Free radicals: if you have an unpaired molecule or positive and negative ions are unpaired, the cell can become unstable. This is because the cell is more at risk for genetic mutation and this is why people take antioxidants to prevent this from happening. As a result of un-pairing, the cell is at risk for injury.
• Free radicals can be as a result of radiation, x-ray, and UV.
• Lipid peroxidation: destruction of the unsaturated fat (plaque). What ultimately causes cardio diseases is hypertension and plaque formation in the vessels (which is lipids/triglycerides). If too much pressure occurs, the plaque can dislodge and you’re going to bleed. (Think of this like when you fall and scrape your knee, you’re going to bleed). The immediate response is for platelets to migrate to the area to stop the bleeding. This then leads to clot building up so much that it blocks the blood flow going to the heart that causes the MI.
• Reactive oxygen species (ROS): oxygen-containing molecules with free radicals present. The problem with these free radicals is that they react with things in the environment. You can have genetic mutations; they react to proteins and enzymes. Acid starts to build up and make changes in DNA. Ultimately, the DNA is affected.
Hypoxic Cell Injury:
• Deprives cell of oxygen and interrupts oxidative metabolism and the generation of ATP.
o Acute cellular swelling (edema)
• The longer the tissue is hypoxic, the greater the chance of irreversible cellular injury.
• Causes of hypoxia:
1. Inadequate amount of oxygen in the air
2. Respiratory disease
3. Inability of the cells to use oxygen
4. Edema
5. Ischemia: decreased blood flow due to vasoconstriction or vascular obstruction. Impaired oxygen delivery and impaired removal of metabolic end products such as lactic acid.
Lecture notes:
• Hypoxia cell injury is the most common
• When you don’t have O2 present, there is no oxidative phosphorylation so no production of pyruvic oxygen. If this doesn’t happen, it affects your ATP. You’ll then have an insufficient amount of energy when you don’t have ATP/oxygen present. Your body then goes to anaerobic sources to try to get as much energy as it can. When this happens your body builds up lactic acids and it depletes the glycogen resource of the cell (this is because it uses its limited glycogen stores in attempt to maintain vital ell functions) and so the cell dies. Overall, hypoxia deprives oxygen and disrupts oxidative metabolism so anaerobic resources are used and lactic acid is formed and this deprives the cell from glucose/sugar/energy and results in death.
• When you have cardiac disease, it ultimately leads to ATP reduction. What causes this is too much accumulation of sodium, calcium and potassium. Na+/K+ pump fails – sodium out and potassium in. Too much sodium accumulates in the cell therefore water will follow and the heart will swell and this causes the heart to not pump very well.
• Hypoxia: any respiratory disease in the heart or lungs. In ability of cell to use oxygen.
• Edema: too much fluid in an organ that constricts flow.
• Edema doesn’t only occur in organs but it can also occur outside of the vessels. It pulls fluid out into the interstitial. We want enough volume in the circulatory system to keep our respiratory system going and pumping therefore this is bad because this can decrease blood pressure in the vessel if the fluids are leaving the vessel and going out into the interstitial.
• Interstitial edema= 3rd spacing
• ATP/glucose/oxygen leads to CO2 being released Impaired calcium homeostasis:
• Calcium functions as an important second messenger and cytosolic signal for many cell responses.
• Cytosolic calcium levels are kept low by energetic mechanisms.
o Ischemia- induced calcium disruption
o Inappropriate activation of enzymes
• Ischemia and certain toxins lead to an increase in cytosolic calcium because of an increased influx across the cell membrane and the release of calcium from intracellular stores.
• The increase calcium level inappropriately activates enzymes that can have damaging effects.
• These enzymes include:
1. Phospholipase: responsible for damaging the cell membrane
2. Proteases: damage the cytoskeleton and membrane proteins
3. ATPase’s: breakdown ATP and hasten its completion
4. Endonucleases: fragment chromatin
• It is known that injured cells accumulate calcium. It is unknown whether this is what causes irreversible cell injury.
• Decreased ATP production levels sodium and potassium pump fails no homeostasis increase of intracellular sodium and influx too much sodium so then water follow cell swells up and dies.
QUESTION: Which of the following can result in membrane damage?
ANSWER: All the above. Inactivation of Na+/k+ ATPase, oxidation of phospholipid, ischemic activation of Ca+2 –regulated protease.
Reversible cell injury:
• Impairing cell function does not result in cell death.
• There are two patterns of reversible cell injury:
1. Cellular swelling: impairment of the energy-dependent Na+/K+ ATPase membrane pump, usually as the result of hypoxic cell injury.
2. Fatty changes: linked to intracellular accumulation of fat.
Lecture Notes:
• Cell swelling usually has to do with swelling because of water. Cerebral edema. Give them sodium in order to draw fluid out of the brain.
Programmed Cell Death:
• Number of cells in tissues regulated by cell proliferation balanced with cell death
• This process is good because it eliminates cell that are:
1. Worn out
2. Have been produced in excess
3. Have developed improperly
4. Have genetic damage
• Cell death occurs via:
1. Necrosis
2. Apoptosis
• Apoptosis: (programmed cell death) highly selective process that eliminates injured and aged cells, thereby controlling tissue regeneration.
o Apoptosis is though to be responsible for several normal physiologic processes, including the programmed destruction of cells during embryonic
development hormone dependent involution of tissues, death of immune cells, cell death by cytotoxic T cells etc.
o Cytotoxic T cells and natural killer cells are though to destroy target cells by inducing apoptotic cell death.
o Apoptic cell death allows for the next stage of organ development such as the heart during embryogenesis.
• Necrosis: cell death in an organ or tissue that is still part of a living organism.
o Causes loss of cell membrane integrity and enzymatic breakdown of cell parts and triggers the inflammatory process.
o Unlike Apoptosis that functions in removing cells so new cells can replace them, Necrosis often interferes with cell replacement and tissue regeneration.
Lecture notes:
• Apoptosis: occur both in normal and pathological cells. Its affected by extrinsic (tumor necrosis factor) and intrinsic (the cells DNA or damage within the cell that causes decreased ATP production). Know that apoptosis is a NORMAL response. If you have a cell that’s viral, the body wants to attack that cell and replace it with a healthier cell. This is a good thing! This kills bad cells and replaces it with good cells. it also eliminates worn out cells that can have genetic damage.
• Necrosis: autolysis. The cell sets itself up. This can be caused by severe trauma that occurs to the cell. Unplanned cell death. NOT GOOD. Example: gangrene-diabetic patients that have minimal blood flow to a particular area and this causes ischemia. This is why you see amputations—the patients don’t have enough oxygen being sent to those areas. Or gout patients on their fat toe. If you don’t treat it, it can become necrotic. The tissue is dead when you’re necrotic.
Gangrene:
• The term gangrene is applied when a considerable mass of tissue undergoes necrosis.
• Can be classified in two ways:
1. Dry gangrene: the part becomes dry and shrinks, the skin wrinkles and its color changes to dark brown or black. The spread is slow and its symptoms are not as marked. The irritation is caused by the dead tissues producing inflammatory responses. Usually results from interference with the arterial blood supply to a part without interference with venous return and is form of coagulation necrosis.
2. Wet gangrene (moist gangrene): the area is cold, swollen and pulseless. The skin is moist, black and under tension. Liquefaction occurs and foul odor is caused by bacterial action. Spread of tissue damage is rapid. Systemic symptoms
are usually severe, and death may occur unless the condition is treated. Results from an interference of venous return to the part. Bacterial invasion is important in the development of wet gangrene because it plays a role in prominent symptoms. Dry gangrene is almost only for the extremities but wet gangrene can affect internal organs or the extremities. If bacteria invade, then dry gangrene can become wet gangrene.
CHAPTER 9:
• Stress: orchestrates set of bodily responses to any form of noxious stimulus.
Homeostasis:
• The body requires a level of homeostasis, or constancy, to be maintained during in internal and external environments (stressors)
• Homeostasis requires feedback control that:
1. Regulate cellular function
2. Integrate the function of other body systems
• Feedback systems
o Most control systems operate by negative feedback
o EX: in the negative feedback mechanism that controls blood glucose levels, an increase in blood glucose stimulates an increase in insulin, which enhances the removal of glucose from the blood. When glucose has been taken up by cells and blood glucose levels fall, insulin secretion is inhibited and glucagon and other counter regulatory mechanisms stimulate the release of glucose from the liver, which causes the blood glucose to return to normal.
Lecture notes:
• We have receptors in our body.
• Beta-receptors: help increase heart rate. Vasoconstriction occurs. Contractility as well as conduction
• Norepinephrine can cause vasodilation type of feedback.
• Homeostasis: the way the body responds to specific stressors
• Negative feedback: high glucose. Sends message to brain to make more insulin to decrease this. When you have stress then feedback won’t be efficient. If there’s an imbalance it takes away from our health.
• Stress responds in a way that tells us in anticipation that something is going wrong. The issue becomes when too much stress happens.
• Everyone responds to stress in different ways, no one is the same.
Negative Feedback System:
Lecture notes:
• If value decreases below. It tells the brain to increase it
• Hypothyroidism: low thyroid levels. Signal is sent to the brain to increase thyroid levels.
• When there is too much. Negative feedback system kicks in to maintain homeostasis and that would slow it down.
• Too much of something produces less and too little of something produces more.
Example: (diagram)
Lecture Notes:
• Blood glucose levels fall glucagon kicks in to make sugar levels increase
• Cortisol is important to know. In the release of glucose for energy. It’s good when you’re in an emergency situation. But if you have too much cortisol, it’s unhealthy. The key is to maintain homeostasis.
• Cortisol is good to be released in a time of need (being attacked). Too much cortisol can
lead to immunosuppression.
The Stress Response:
• Hans Selye: world-renowned endocrinologist that was the first to describe a group of specific anatomic changes that occurred in rats that were exposed to a variety of different experimental stimuli. He came to an understanding that these changes were manifestations of the body’s attempt to adapt to stimuli.
• Stress: a state manifested by a specific syndrome of the body developed in response to any stimuli that made an intense systemic demand on it
• General Adaptation Syndrome (GAS):
o General because the effect was a general systemic reaction
o Adaptive because the response was in reaction to a stressor
o Syndrome because the physical manifestations were coordinated and dependent on each other
Lecture notes:
• He believed stress happens primarily to a physiological response. We want our body to respond to a stressful event in some specific way. Eventually, it adapts to it and plateaus but if you don’t maintain homeostasis, the health status will decrease. We go on to try to maintain an adaptive state but if we can’t maintain homeostasis then we end up with a syndrome.
• He also discovered what’s called the triad stress effects.
General adaptation syndrome
• 3 stages
1. Alarm stage: general stimulation of SNS and HPA (hypothalamic-pituitary- adrenal) axis release of catecholamine’s and cortisol
2. Resistance stage: body selects most effective defense cortisol levels drop (no longer needed)
3. Exhaustion stage: resources are depleted, systemic damage occurs
Lecture notes:
• Alarm state: when your body reacts (fight or flight)
• Resistance state: when everything levels off. CNS is mostly aroused and body’s defense is mobilized
• Adaptation: not always a good adaptation because it means that you never got to maintain homeostasis. You lost the ability to adapt to that stress or the adrenal gland becomes insufficient. There’s only so much that the adrenal gland can function. If you go into overdrive, the adrenal slows down. And the adrenal is responsible for adrenaline, to increase heart rate and basically, to keep us going.
Hormones Involved in Neuroendocrine Response to Stress
• Catecholamine’s (Norepinephrine & Epinephrine): produces a decrease in insulin release and an increase in glucagon release that results in increased Glycogenolysis. Increase heart rate, cardiac contractility, vascular smooth muscle contraction, and relaxation of bronchial smooth muscle.
• Corticotropin-releasing factory (CRF): comes form the hypothalamus and stimulates the release of ACTH from the anterior pituitary
• Adrenocorticotropic hormone (ACTH): comes from the anterior pituitary and it stimulates the synthesis and release of cortisol from the adrenal cortex
• Glucocorticoid hormones (cortisol): released from the adrenal cortex. Potentiates actions of epinephrine and glucagon, inhibits the release and/or actions of reproductive hormones and thyroid stimulating hormones. Produces a decrease in immune cells and inflammatory mediators.
• Mineralcorticoid hormones (Aldosterone): Increases sodium absorption by the kidneys.
• Antidiuretic hormones (ADH, Vasopressin): comes from the hypothalamus and is stored in the posterior pituitary. Increases water absorption by the kidneys. Produces vasoconstriction of blood vessels and stimulates the release of ACTH.
Lecture notes:
• Epinephrine: important for cardiac and respiratory
• ACTH: to release catecholamine’s and aldosterone
• Cortisol: main course in glucose
• Aldosterone: sodium and water retention
• If you don’t have increased volume, you can have hypertension and it can collapse Sympathetic nervous system:
• Fight or flight response
• Rapid response to trauma and emergency
• SNS symptoms:
o Increased HR and RR
o Dilated pupils
o Decrease GI activity
o Pale, cool skin
o Decreased kidney function
• Stress hypothalamus SNS activated SNS neurons norepinephrine adrenal medulla epinephrine released into blood
Lecture notes:
• Stress sends signal to the hypothalamus to tell the pituitary gland to signal the adrenal gland to increase epinephrine and its going to do this in a state of stress. This happens regardless of what the blood pressure is. Norepinephrine is released when there is a decrease in blood pressure.
• Epinephrine: causes indirect increase of pancreatic function which results in increase of glucagon to cause gluconeogenesis increases glucose to have energy.
Cortisol –The “Stress Hormone”:
• Central to the neuroendocrine response to stress
• Small peptide hormone that regulates pituitary and adrenal activity
Hypothalamus
CRH
Anterior pituitary
ACTH
Adrenal cortex
fat, and protein,
Cortisol
inflammatory and
metabolis m
Lecture notes:
• Cortisol increased blood pressure, cardiac output and
amino acid levels which are big in muscle formation
• This helps promote gastric secretions which too much is not good because it can give you ulcers
• Cortisol can have a negative affect. Too much can lead to pro-inflammatory state of mind. High levels for too long can suppress immune system and cause sepsis (inability for body to oxygenate organs) and die.
Angiotensin II:
• Stimulation of SNS
o Activates the peripheral renin-angiotensin-aldosterone system (RAAS)—Renal retention of sodium and water
ADH:
• Released from the posterior pituitary
• Hypotensive stress or fluid volume loss
o Increases water retention
o Produces vasoconstriction
Lecture notes:
• Kidneys release renin.
• Renin makes ACE that turns angiotensin 1 (that doesn’t do anything) to angiotensin 2.
• ADH (vasopressin): increases water retention. To increase blood volume and more cardiac output and flow to someone in stress.
• RAAS- results in the retention of sodium and water. Prolonged may cause pathological changes. Initial response is ok but then too long is bad. Sodium causes retention of bicarbonate and water.
• ACE is the angiotensin converting enzyme between angiotensin 1 and 2.
Immune Response:
• Stress is known to suppress the immune system
• Neuroendocrine and immune system share common signal pathways (this is why it can suppress the immune system)
• HPA axis activated by cytokines (interlukin-1, interlukin-6, tumor necrosis factor) released for of immune cells
• SNS releases catecholamine’s
• T helper cell subtypes secrete cytokines and stimulate different aspects of the immune response
Lecture notes:
• Stress in the upside: normally can increase blood pressure and volume. Blood flow shifts away from organs and kidneys and goes to vital organs such as the heart, brain, and lungs.
• Downside: elevated blood glucose. Initially great but not good long term.
• Hyperglycemic state. Increase in lipid formation. This causes atherosclerosis (the build- up of fats, cholesterol, and other substances in and on the artery walls). This can depress immune response therefore can increase risk of infections. The patient is going to be more fatigued with too much stress response. They will have fewer lymphocytes and have inflammation.
Factors Affecting the Ability to Adapt:
• What helps us adapt?
o Environmental control (air conditioning, heat)
o Antiseptic agents
o Immunizations
o Antibiotics
• What creates new challenges?
o Noise/air pollution
o Increased exposure to harmful chemicals
o Changes in biologic rhythms imposed by shift work
o Global travel Adaptation Depends on:
• Physiologic and anatomic reserves: the ability of body systems to increase their functions given the need to adapt (physiologic reserve). Being able to live with one kidney, one lung etc.
• Time: adaptation is more efficient when changes occur gradually rather than suddenly. Ex. Losing a liter or more of blood through a week rather than fast and going into signs of shock and hypotension.
• Acute vs. chronic
• Genetics: genetics can ensure that systems that are essential to adaptation function adequately. Ex. Genes with sickle cell anemia persists in some populations but it also provides those people to be resistant to infections with the parasite that causes malaria.
• Age: the capacity to adapt is decreased at the extremes of ages. Either too young or too old.
• Health status: having physical and mental health is a strong determinant for the ability to adapt.
• Nutrition: malnutrition can lead to immunodeficiency. Any deficiency or excess can impair a person’s ability to adapt.
• Sleep-wake cycle: sleep is a restorative function in which energy is restored and tissues are regenerated.
• Psychosocial environment: psychosocial factors and negative events have been correlated to illness.
• Individuals perception of stressor
Stressor and Adaptation:
• The ability to adapt is influenced by previous learning, physiologic reserve, time, genetic endowment, age, health status and nutrition
• Physiologic stress: controlled on a moment to moment basis by feedback control
• Psychological stress: not regulated with the same degree of specificity and feedback control
o Effect may be inappropriate and sustained
Lecture notes:
• Psychological has to do with genetics and social support Physiologic Stress:
• Stress-induced changes in body functions
• Detected by body’s normal regulatory sensors
• The body alters function to restore normal balance
• When normal balance is restored, negative feedback stops the reaction
Lecture notes:
• Physio=body
• Body tries to maintain homeostasis Psychological Stress:
• Directly affects the central nervous system
• Turns on the stress responses, even when the body’s internal sensors have not detected an imbalance
• Question: do the stress responses solve the person’s problem? NO
• Question: will negative feedback tell them when to turn off? YES
Adaptation:
• Depends on:
o Physiologic and anatomic reserves
o Acute vs chronic
o Genetics
o Age
o Health status
o Nutrition
o Sleep-wake cycle
o Psychosocial environment
o Individuals perception of stressor
Possible Stress-Induced Health Problems:
• Anxiety
• Depression
• PTSD
• Eating disorders
• Sleep disorders
• Drug and alcohol misuse
• Suicide
• Diabetes Type II
• Infection
• HTN
• GI Problems
• Obesity
• Cancer
• Atherosclerosis
•
• k
• CHAPTER 61:
•
• Types of Ultraviolet Rays:
•
• UVC Rays
o Short (100 to 289 nm); do not pass through the earth’s atmosphere. Can be produced artificially and can be damaging to a persons eyes.
•
• UVB Rays
o 290 to 320 nm; responsible for nearly all the skin effects of sunlight. Responsible for all skin effects of sunlight including photoaging (wrinkles), pigmentary changes, dryness and loss od skin tone that occurs with enhances of sunlight exposure. Artificial sources such as tanning salons and therapeutic solar interventions for certain skin conditions, also produce the same effects as UVB.
•
•
• UVA Rays
o 321 to 400 nm; can pass through window glass, are more commonly referred to as sun tanning rays.
•
• Lecture Notes:
•
• As we begin to get older the skin obviously becomes more fragile, thinner, so you have problems with thermoregulation.
•
• As you get older wound healing is definitely more difficult.
•
• Someone who is not diabetic will heal more easily then someone who is diabetic.
•
• Erythema= redness
•
• IMPORTANT: As we get older our skin gets thinner and dryer and there’s a decrease in melanocytes that are there for our protection. Therefore, we have a decrease in pigmentation. Older people also have difficulty in wound healing. They’re also more at risk for any thermoregulatory issue (having difficulty maintaining themselves warm) They have the capability of being cold, but sometimes they aren’t able to sweat as much so sometimes they have a risks of heat strokes because they’re not able to thermo- regulate.
•
• There’s also a decrease in fatty tissue and subcutaneous fat.
•
• Effects of Ultraviolet Rays of Sunlight:
•
• Acute affects for UVA and UVB
•
o Short-lived and reversible
o Erythema: UVA erythema occurs immediately and fades within 2 hours, it is believed that it is due to the “heat load”. UVB erythema has a delayed response— about 6-24 hours after exposure to sunlight and fades over 1 or 2 days.
o Pigmentation: due to the delayed increase in the number of melanocytes
o Injury to Langerhans cells (help protect against infection) and keratinocytes
•
• Chronic affects
•
o Directly damaging skin cells
o Accelerating the effect of aging on skin
o Producing changes that predispose to development of skin cancer
• Treatments
• Relaxation techniques
• Guided imagery
• Music therapy
• Massage therapy
• Biofeedback
•
• Lecture Notes:
•
• Acute affects are for both UVA and UVB.
•
• Pigmentation: tanning
•
• Keratinocytes: like a protein for nails and hair
•
• Increase in capillary permeability and fragility as chronic changes hence why you have fluid accumulation or blister formation.
•
• Reversible short lived AKA a sunburn, you get darker when you do go to the beach; long term effects: you should protect your face because too much sun can cause you to age more easily
•
• Capillary permeability: when fluid going into the third space (with really bad burns people develop blisters and that what it means it deals with hydrostatic pressure)
•
• Sunburn:
•
• Excessive exposure of the epidermal and dermal layers of the skin to ultraviolet radiation
• Resulting in an erythematous inflammatory reaction
• Inflammation, blistering, weakness, chills, fever, malaise, and pain often accompany severe forms of sunburn
•
• Lecture notes:
•
• First-degree burns are more superficial.
•
• Second degree, deep partial fitness
•
• You can have necrosis from long-term sunburn due to insufficient blood supply.
•
• The pain depends on if it’s a first, second, or third degree burn (you may find someone with a very bad burn, the person with third degree might not feel it because all those nerves are going to be dead).
•
•
• Measures of Protection from the Sun:
•
• Avoidance of sun exposure
• Use of protective clothing
• Use of sunscreens
o Chemical agents absorb UVR
o Physical agents reflect UVR
o Biological agents reduce inflammation
o Broad-spectrum suntan lotions protect against both UVA and UVB.
•
• The Development of Skin Cancer:
•
• Nevi (moles)—common congenital or acquired benign tumors of the skin that can predispose individuals to cancer. Can be flat or elevates, pigmented or non-pigmented, hairy or non-hairy.
•
o Nevocellular nevi: pigmented skin lesions resulting from proliferation of melanocytes in the epidermis or dermis. Tan to deep brown, uniformly pigmented, small papules that are well defined, have rounded borders.
•
o Dysplastic nevus: larger than other nevi and have great tendency to transform into malignant melanoma. Appearance is flat, slightly raised plaque with a pebbly surface or target like lesion with a darker, raised center and irregular borders.
•
• Lecture Notes:
•
• Pigmented= color
•
• Nevi’s can be pigmented or non-pigmented
•
• Can be congenital (born with it) or something you acquire
•
• Dysplastic (more geared towards malignancy—more at risk towards cancer). Tends to be larger in size than Nevocellular. They’re flat and have target like leisure.
•
• 3 Major Types of Skin Cancer:
•
• Malignant melanoma: rapidly progressing malignant tumor of the melanocytes. It is a metastatic form of cancer. Those that are at greatest risk are fair-skinned people, particularly with blonde or red hair who sunburn and freckle easily. Those that are also in risk are people who’ve had 3 or more blistering sunburns before 20 years od age. In darker skinned toned people, melanomas occur in non-exposed sun areas, such as the
mucous membranes, palmar and plantar surfaces. Most come from pre-existing Nevis (moles). Surrounded by erythema (due to inflammation and the body’s response in trying to destroy the tumor), tenderness, growth (blue color), inflammation and scar tissue formation (white).
• Basal cell carcinoma: neoplasm of the non- keratinizing cells of the basal layer of the
epidermis; most common skin cancer in white-skinned people. These are non- metastasizing tumors that extend wide and deep if left untreated. These tumors are frequently seen in the head and neck or areas of skin that have hair.
•
• Squamous cell carcinomas: second most frequent occurring malignant tumors of the outer epidermis. Those in contact with industrial tars, coal, and paraffin have an increased likelihood of contracting SCC.
•
• Lecture notes:
•
• Malignant melanoma: rise in this because of more sun exposure. This is the one we are mostly concerned with.
•
• Melanomas: malignant tumors of the melanocytes
•
• Basal cell carcinoma: do not tend to metastasize. In arms or forearms. Less aggressive.
•
• Squamous cell carcinomas: affects more males than females. Also due to an increase in UV exposure. This is also linked to some occupations such as things related to arsenic, tar, or coal. This type of skin cancer is most often seen in the face, nose, ears, lower lip, and back of hand.
•
• Four types of melanomas:
•
• Superficial spreading (most are this type)
o Raised edges, grow horizontally and vertically
o Ulcerate and bleed
•
• Nodular
o Dome-shaped; blue and black
o Almost looks like a cyst
•
• Lentigo maligna
o Slow growing, flat
•
• Acral lentiginous
o On palms, soles of feet, nail beds, mucous membranes
•
• Lecture notes:
•
• Melanomas are malignant tumors of the melanocytes (purpose of melanocytes are to protect us from the sun)
• There are different sizes and shapes of melanomas
• Asymmetry is different
• Border is different
• Color is different
• Diameter of the actual lesion
• There are risks factors of melanoma:
o Fair skin
o If you were majorly sunburned and had blister formation before the age of 20, you’re really at risk for melanoma
o Atypical nevis will also put you at risk for melanoma
o People who freckle easily
•
• Degrees of Burns:
•
• First-degree burns (superficial partial-thickness burns): involve only the outer layers of the epidermis. They are red, pink, dry and painful. No blister formation. Ex. Mild sunburn. The skin maintains its ability to function as a water vapor and bacterial barrier and heals within 3-10 days. Require only palliative treatment such as pain relief and adequate fluid intakes.
•
• Second-degree partial-thickness burns: involve the epidermis and various degrees of the dermis. These are painful, moist, red, and blistered. Underneath the blisters is weeping, bright pink or red skin that is sensitive to temp. Changes, air exposure and touch. These blisters prevent loss of body water and superficial dermal cells. It is important to maintain intact blisters after injury because they serve as a good bandage and promote wound healing. Heals in approximately 1-2 weeks.
•
• Second-degree full-thickness burns: involve the entire epidermis and dermis. Hair follicles and sweat glands remain intact. These burns can be very painful because the pain sensors remain intact. Tactile sensation may be absent or diminished. Mottled pink, red or waxy white areas with blisters and edema. Blisters are flat, and dry. Healing takes about 1 month. Burns maintain softness and elasticity—but sensation may be lost. Scar formation is usual. Burns heal with supportive medical care aimed at preventing further tissue damage, provide adequate hydration.
•
• Third-degree full-thickness burns: extend into the subcutaneous tissue and may involve muscle and bone. Waxy white or yellow to tan, brown, deep red, or black. These burns are hard, dry and leathery. Edema is extensive. No pain because nerve endings are destroyed. No pure 3rd degree because they are all surrounded by 2nd and 1st degree burns. There’s permanent scar.
•
• Lecture notes:
•
• First degree: are superficial. Mild sunburn. There’s redness. Involves the outer layer (epidermis) EX: sunburn only epidermis is involved.
•
• Second degree: there are two. Partial and full thickness. These are the one that are more painful. These also have blisters
• Third degree: these are black and leathery. No blister formation with this type of burn.
When you have patient who burn victim. They wont really have a lot of pain because their nerve ending is dead. (Subcutaneous and involves the tissue and the bone, looks leathery)
•
• Estimation of total body surface area in involved in burn:
•
• Rule of nines
• Multiple of 9%
o Perineum 1%
o Arm 9%
o Leg 18%
o Anterior trunk 18%
o Posterior trunk 18%
o Head 9%
•
• Lund and Browder chart
• American Burn Association classification of burns
•
•
• Lecture notes:
•
• By this we can determine the percentage of the patient’s burn
•
• The number one treatment for burn victims is IV fluid. LOTS of liters. 10-12 liters back to back. Hydration is key as well as pain management
•
• Make sure airways is protected at all times: ANY burn patient you need to consider airway- they could have just burned their hand and have them internally)
• Sepsis- your skin is your first line of defense and if its not working and open to air then
obviously bacteria gets in extremely easily
•
• Systemic Complications of Burn Tissue:
•
• Magnitude of the response is proportional to the extend of injury
•
o Hemodynamic instability: this is because burning lets a lot of fluids out. We lost fluids from our vasculature, interstitial and cellular compartments. This can lead to hypovolemic shock—also known as burn shock. The person will have decreased cardiac output, increased peripheral vasculature resistance, impaired vital organ perfusion. Electrical injuries that cause burns can also produce cardiac arrhythmias and it requires immediate attention.
•
o Impaired respiratory function: especially if the patient inhaled smoke. People are often trapped in a place where they inhale large amounts of smoke, carbon monoxide, and other toxic fumes. There also may be thermal injury to the respiratory passage. Always have an intubation/crash cart near by!
•
o Hyper-metabolic response: increase in basal metabolic rate due to an increase in oxygen demand that the patient has and nutritional requirements. Catecholamine’s (epinephrine and norepinephrine) and cortisol are increased to maintain homeostasis. Heat production is increased in order to manage heat loss from the burned area. Patient will also have an increase glucose use. Therefore, nutritional support is essential for patients recovery.
•
o Major organ dysfunction: due to hypovolemic shock and organs not being able to be perfused. Renal insufficiency can occur in people with burns as a result of hypovolemic state. Gastric ulceration also occurs from ischemia to the gastro intestinal tract.
•
o Sepsis: complication of burn injury. May arise from burn wound, pneumonia, UTI, infection somewhere else in the body. The patient lost its 1st border line of defense (the skin) therefore they’re highly susceptible to infection that can spread.
•
• Lecture notes:
•
• Any time there’s any burn, it affects any part of the body.
•
• We become hemodynamic instable because burning lets out a lot of fluids. We lost fluids from our vasculature (hypovolemic shock). Cardiac output will be compromised.
•
• Patients can also from impaired respiratory function especially if they inhaled smoke. This is why it is important to have an intubation cart near by. The patients will have a dry cough
• The patient will also have a hyper-metabolic response—increase in basal metabolic rate
due to an increase oxygen demand that the patient has. Everything is going to go up.
•
• Increase glucose is going to be used to help us with prevention of protein wasting.
•
• GI wise—ulceration will occur because everything is going to vital organs such as the heart, lungs, and brain but not the kidneys or GI system. These patients will be on protein pump inhibitors.
•
• Sepsis: inability for body to oxygenate organs
•
• Treatment of Burns:
•
• Immediately submerge area to cool tissue
• Emergency care
o Resuscitation
o Stabilization
o Maintaining cardiac and respiratory function
•
• Intermediate and long-term treatment is dependent on the extent of the injury
o Protection from desiccation
o Escharotomy/fasciotomy:
•
• Circumferential burns: burns that encircle the entire surface of the body or a body part (legs, arms, torso) and act like tourniquets and can cause major tissue damage to muscles, tendons and vascular under the leathery burned skin. This puts pressure on whatever area its located and can cause tissue damage. Pressure needs to be relieved via Escharotomy or surgically via fasciotomy.
•
• Lecture notes:
•
• IV FLUIDS—for treatment
•
• Stabilization: maintain cardiac and respiratory. These are your priority patients
•
• Escharotomy/fasciotomy: scarring or dead tissue puts pressure on the area for example on the stomach and the dead tissue needs to be removed to relieve the pressure.
•
• When a patient has a burn, the eschar tissue, they start to develop necrosis and the skin begins to look leathery (almost looks like a tunicate) EX: chest cavity, that will not allow expansion of the lungs, so when that happens they have to literally cut it to allow the patients to breathe (escharotomy)
•
• Local & Systemic Responses:
•
• Minor burns heal with inflammatory response
• Larger wounds heal with scar tissue formation
•
• Loss of normal skin function; stress response; release of cytokines; dysrhythmias (v-fib); damage to the alveolar capillary membrane related to inhalation of toxins; all body systems are affected.
•
• Lecture notes:
•
• The patient will also have an electrolyte imbalance because of the amount of fluid were losing this can lead to dysrhythmias ... V-fib.
•
• Dysthymias: can happen with electrical type of burns.
•
• Complications of Burns:
•
• hemodynamic instability: begins immediately with injury to capillaries in the burned area. Fluid is lost from vasculature, interstitial and cellular compartments. Because of loss of vascular volume, they can go into hypovolemic shock aka burn shock. The person has a decrease in cardiac output, increased peripheral vascular resistance, and impaired perfusion of vital organs. Electrical injuries that cause burns can produce cardiac arrhythmias that require immediate attention.
•
• Respiratory system dysfunction: smoke inhalation and post-burn lung injury. They inhale smoke, carbon monoxide, and other toxic fumes. Hoarsenesss, drooling, inability to handle secretions, hacking cough, and labored/shallowed breathing.
•
• Hyper-metabolic response: stress of burn injury can increase metabolic and nutritional requirements. Catecholamine’s and cortisol is increased in an effort to balance heat losses from burned area. Hyper-metabolism—increased oxygen consumption increased glucose use, protein and fat wasting. Nutritional support is essential for wound healing.
•
• Renal insufficiency: as a result of hypovolemic state, damaged to the kidneys at the time of burn. Urine output is increased.
•
• Gastric ulceration: gastric dilation and decreased peristalsis. Due to gastric ischemia from the stress.
•
• Sepsis: arises from burn wound, pneumonia, UTI, infection elsewhere in the body. When the skin is no longer intact, the person is open to bacterial infection.
•
• Constriction of areas under circumferential burns
•
• Systemic infection
•
•
•
• Lecture notes:
•
• Burn shock—hypovolemic shock (condition in which the liquid portion of the blood plasma is too low)
•
• Gastric ulceration: you will get this because everything goes to the organs, leaving the GI tract.
•
• Respiratory function: can have alveolar collapse because of inhalation of smoke
•
• Increase metabolic rate
•
• Renal insufficiency due to hypovolemic shock. If you don’t have enough fluid in the vascular you won’t use your kidneys. If you have decreased blood flow to your kidneys you can have something called anuria—decrease in urine production. This will change later because the main treatment is IV fluid.
•
• Constriction of areas under circumferential burns—when a specific area is burned, it’ll put pressure of the dead scar tissue on a specific part of the body. It is like having a tourniquet. This usually occurs in the torso.
•
• The leading cause of complications is systemic infection—these patients will be in protective isolation because they are at really high risk of sepsis. You need a lot of training because you’re dealing with open wounds and so everything needs to be sterile. Thermoregulation is very important in these patients because they lost their skin that is the main organ in our body that keeps us warm. They usually die from systemic infection. Its not breaking issues or renal issues. Its because they become septic (infection spreading to other parts of your body)
•
• Burn Complications (continued):
•
• Fluid imbalances: during post-burn period that capillaries reach their maximal dilation and permeability in relation to release of histamine, prostaglandins and kinins
•
• Intravascular fluid: shifts into interstitial space. Fluids are lost through evaporation 10 times normal rate
•
• Hypovolemic shock: (“burn shock”) results
o Manifests as less cardiac output, hypotension, tachycardia, oliguria, massive edema (watch out for airway!)
o Treat with large doses of isotonic fluid (Ringer’s lactate)
•
• Lecture notes:
•
• Hypovolemic— no fluid in vasculature (the causes to have hypotension)
•
• Tachycardia because its trying to compensate.
•
• Edema—watch out for the airway, you want an intubation cart close by.
•
• Isotonic—fluids identical to normal saline.
•
• First Degree—Superficial:
• Partial thickness
• Epidermis only
• Sunburn
• No treatment required
•
•
• Lecture notes:
•
• No blisters for 24 hours
• Aspirin/Tylenol
• Heal within 3-5 days
• Localized pain and erythema
• Palliative care—pain management as treatment
•
• Second Degree--Superficial partial thickness burn:
•
• Scalding
• Thin-walled, fluid filled blisters
• Blisters arise within minutes
• Severe pain
• Heals in 3-4 weeks • Scarring common
•
•
•
•
• Lecture notes:
•
• There are blisters in these burns!!
•
• Goal—prevent further damage from occurring.
• Its important to hydrate this patient and try to support the growth of the skin. You’ll have a wound care nurse involved with this patient.
•
• Second Degree-Deep Partial Thickness Burn:
•
• Example is a fire burn
• Epidermis, reticular dermis
• Only pressure perceived
• Pallor—unhealthy pale appearance
• Scar formation
•
•
• Lecture notes:
•
• There is scar formation here
•
•
• Third Degree Burn- Full thickness burn:
•
• Epidermis, deep underlying tissues
• Only perceives deep pressure
• Dry, leathery appearance
• Hard, black or purple
• Requires hospitalization
•
• Severe scarring
• Fluid replacement
• Narcotics
• Contractures
•
•
•
• Lecture notes:
•
• This type of burn requires skin re-graphing
•
• Although these 3rd degree patients don’t feel pain because their nerve endings are damaged they do receive narcotics because all of their burns may not be third degree and they may have pain. Some of their burns can be a mixed. Also, if they do the procedure to remove the skin to release pressure—they would need pain meds.
•
• Remember: if you’re not sure what kind of burn it is always rate it higher.
•
• Scenario Question:
•
• A woman was severely burned and she has been in the hospital for eight days
• Question: why would she be developing:
o Increased urine production? Because of treatment of IV
o Weight loss? Because of metabolic increase
o Increased temperature? Can have infection and lack of thermoregulation
o GI Bleeding?
•
• Pressure Ulcers (Bedsores):
•
• Ischemic lesions of the skin and underlying structures caused by unrelieved pressure
•
• 4 factors that contribute to the development of pressure ulcers:
1. Pressure
2. Shear forces
3. Friction
4. Moisture
•
• Lecture notes:
•
• Critical patients or obese patients don’t move.
• Diabetics also don’t move because they have neuropathy that doesn’t feel as much.
• Pressure
• Shear force: from sliding from one seat to another
• Friction: usually in the elbows from sliding yourself up
• Moisture: if they sit in urine or stool or if they didn’t dry up well after a bath. Also if they’re sweating because they’ve had fevers
• These ulcers usually occur between bony prominences. For example, the greater
trochanter, the patient's heels can also have skin breakdown.
• THE KEY IS PREVENTION. ULCERS ARE PREVENTABLE. –move your patients, change their position.
• If you have pressure ulcer stage 1: we’re going to rotate them more often
•
• Pathophysiology:
•
• Pressure on tissues:
o Capillaries collapse
o Regional edema
o Tissue ischemia
o Cellular death (necrosis)
o Toxins released
•
• Lecture notes:
•
• Capillaries collapse because initially you’ll have swelling
• Tissue ischemia: because of the edema. So blood flow is going to be compromised. Initially there is an inflammatory response that leads to edema and then to ischemia.
•
• Pressure ulcers:
•
• Ischemic lesions of the skin and underlying structures caused by unrelieved pressure
• Ischemic ulcers as a result of shearing force and/or pressure that impairs the flow of blood and lymph.
•
• 4 factors that contribute to development of pressure ulcers:
1. Pressure
2. Shearing force: caused by the sliding of one tissue layer over another with stretching and angulation of blood vessels, causing injury and thrombosis (clotting). This happens when the skeleton moves, but the skin remains fixed to an external surface. Ex. Pulling a person up in a bed or moving a person from a stretcher to bed.
3. Friction: contributes to pressure ulceration by damaging the skin at the epidermal-dermal interface.
4. Moisture: contributes to pressure ulcer formation bu changing the protective pH of the skin. This makes the skin more susceptible to pressure, shear and friction injury.
• Most likely to develop over a bony prominence, but may be subject to anything that
exerts external pressure, friction or shearing forces.
• People with impaired circulation will require less pressure to interrupt circulation so they are at higher risk for ulceration.
• Factors:
o Immobilized elders in SNF are at higher risk
o Incontinence, lying on an O.R. table for long periods
o Longer length of hospital stay, spinal cord injuries
•
• Ulceration Stages: IMPPPPPPP!
•
• Stage 1: non-blanchable erythema of intact skin. Persistent redness in lightly pigmented skin or an area of persistent redness with blue or purple hues in darker skin.
• Stage 2: partial-thickness skin loss (epidermis and/or dermis). This ulcer is superficial
and presents clinically as an abrasion, a blister or a shallow crater.
•
• Stage 3: full-thickness skin loss involving damage or necrosis of subcutaneous tissue that may extend down to but not through underlying fascia. These ulcers manifest as a deep crater with or without undermining of adjacent tissue.
•
• Stage 4: full-thickness skin loss with extensive destruction, tissue necrosis, damage to muscle, bone, or supporting structures.
•
• Lecture notes:
•
• Stage 1: intact skin. No wound cares because the skin is intact.
• Stage 3: full thickness. Involves some subcutaneous tissue and muscle
• Stage 4: you can see the bone. If it is unidentifiable or you have black leathery tissue or you can’t see below it, you have to categorize it as the highest level.
• Stage 2 & 3: have little exudate and are treated with semipermeable or occlusive
dressing. This occlusive dressing can assist with epithelial cell migration by keeping the wound fluid. Wound fluid is thought to contain growth factors that enhance wound healing.
•
• Where do pressure ulcers form? Pressure points (Where you’re putting the pressure and you have boney prominences that’s where you are at higher risk)
•
• Risk Factors
• Elderly
• Neurological deficits
• Incontinence (urinary and fecal)
• Fractures
• Lying on hard surface, wrinkled sheets
• Lecture notes:
•
• Chronic diseases
• Malnutrition
• Any kind of immobilization
•
• Neurological deficits: dementia patient’s sometime pee on themselves.
• Myasthenia gravis patients are immobile
• Malnutrition: specifically, protein. Check albumin we having wound issues. Consider patient’s nutritional status for wound healing
•
• Classification of skin ulcers:
• Stages 1-4
• Once tissue becomes necrotic, bacterial infections sets in.
• Nursing assessment:
o Warm, foul smelling?
o Discharge or drainage?
o Pain?
• Stage 1 Ulcer:
•
• Non-blanchable erythema of intact skin
•
•
• Lecture notes:
•
• Might complain of discomfort
• Treatment: frequent turning. Since there is no open wound it can still be salvaged. Document patient came in with stage 1. If patient gets worse under our care, we do not get reimbursed.
•
• Stage 2 Ulcers:
•
• Partial-thickness skin loss involving epidermis or dermis
•
• Lecture notes:
•
• There IS skin break. Abrasions, blisters and can have shallow craters
• You will treat this with something. Also, you will need to use dressings on the patients.
• There is going to be gunk coming out of it that’s why you would use a dressing. But you don’t want to keep the skin a little bit moist helps with the healing. You don’t want it to be try.
• If the patient is in pain—give them something for the pain.
•
•
•
•
• Stage 3 Ulcers:
•
• Full-thickness skin loss involving damage or necrosis of subcutaneous tissue that extends to (but not through) underlying fascia
•
• Lecture notes:
•
• Can go down to subcutaneous tissue. May require decrement (scrape off dead skin). If its big then they go to the OR.
•
• Stage 4 Ulcers:
•
• Full-thickness skin loss with extensive destruction, tissue necrosis, or damage to muscle, bone, or supporting structures
•
• Lecture notes:
•
• Necrosis death of skin.
• Decrement (scrubbing off skin) is going to be needed surgically.
• Usually requires graphing of skin
• These are the ones that don’t have the pain so much because nerve endings are dead.
•
• Prevention of Pressure Ulcers (Bedsores):
•
• Identifying at-risk persons who need preventative measures and the specific factors placing them at risk
• Maintain and improving tissue tolerance to prevent injury
• Protecting against the adverse effects of external mechanical forces (ex. Pressure, friction, and shear)
• Reducing the incidence of pressure ulcers through education programs
•
• Treatment of Skin Ulcers-Explain rationale:
•
• Nutrition
• Oxygenation
• Frequent turning
• Fluid balance
• Antibiotics
• Flat, non-bulky dressings
• Wound packing
• Pressure mattresses
•
• Lecture notes:
•
• Protein is super crucial to the patients wound healing
• Frequent turning and fluid balance is necessary
• You may need antibiotics
• You want to assess the patient frequently
• Pressure mattresses that inflate and deflate
•
• CHAPTER 8:
•
• Cancer:
•
• Second leading cause of death in the US
• Not a single disease; originates in almost any organ
• 5-year survival rates have improved
•
• Lecture notes:
•
• Neoplasia: abnormal growth that can be benign or malignant
•
• Anaplasia: an alteration of the actual structure of the actual cell. This occurs in cancer. But cell loses the ability to function as it should. It has altered its function. WBC and RBC aren’t doing what its supposed to do so its undifferentiated
•
• The key with cancer is that it inhibits apoptosis from happening.
•
• Classification:
1. Sight of origin: is it the epithelium? Adenocarcinomas rise from the edema
•
• As we age, we are at more increased risk because our cells start to mutate as we age just because we’re trying to get older. There is more accumulation of toxins. We have more exposure to things out of the atmosphere. Heredity and hormones play a role. Immunology—immune system starts to go down as we get older.
•
• HPV- were having more sex, or multiple partners therefore this is linked to cervical cancer.
•
•
• Obesity is also linked to cancer. As well as radiation, exposure.
•
• H. Pylori—a bacterial infection is a known fact that this bacteria puts people at risk for gastric cancer.
•
• Characteristics of Cancer:
•
• Disorder of altered cell differentiation and growth
o Results in neoplasia (“new growth”)
•
• Growth is uncoordinated and relatively autonomous
o Lacks normal regulatory controls over cell growth and division
o Tends to increase in size and grow after stimulus ceases or needs of the organism are met
•
• Lecture notes:
•
• Malignant tumors—poorly differentiated because it doesn’t do its function
•
• Cancer—growth that is uncoordinated and autonomous. They’re multiplying like crazy but aren’t doing their role
•
• Malignant neoplasm is invasive
•
• Metastasis occurs through vessels or lymph nodes.
1. Loss of cell differentiation
2. Cell structure
3. Irregularity of size of cell
4. Ongoing proliferation (apoptosis has ceased/stopped)
5. Sustained angiogenesis (there are vessels feeding it for its growth)
•
• Components of Tissue Renewal and Repair:
•
• Cell proliferation: process of cell division that is an adaptive process for new cell growth to replace old cells or when additional cells are needed.
•
• Cell differentiation: the mechanism by which cells become increasingly more specialized with each mitotic division.
o Process of specialization
o New cells acquire the structure and function of cells they replace
•
• Apoptosis
o A form of programmed cell death to eliminate unwanted cells
•
•
• Lecture notes:
•
• Proliferation: when cell division occurs. It’s an adaptive mechanism of our body. Old cells die and new ones take its place (multiplication)
•
• Differentiation: a specialization where new cells acquire the structure and function of the cells they replace. Dying RBC are replaced by new RBC.
•
• Apoptosis: programmed cell death
•
• Cell Proliferation:
•
• Process of increasing cell numbers by mitotic cell division
• In normal tissue it is regulated
o The number of cells dividing = the number of cells dying
•
• Cell Differentiation:
•
• Process by which proliferating cells become more specialized
• Results in fully differentiated adult cells
o Stimuli to induce mitosis become more limited as cells become more highly differentiated (Ex. Neurons)
•
• Lecture notes:
•
• Differences between benign and malignant
•
• Benign: slow growing, well differentiated, only cause death if they grow to the point where they put pressure on an organ or something. They’re surrounded by capsules
•
• Malignant: fast growing, less differentiated, disorganized and uncontrolled cell growth and the cells break easily because they aren’t encapsulated therefore they travel to other organs hence why they metastasize.
•
• The cell cycle:
•
• An orderly sequence of events that occur as cell duplicates its contents and divides
• Genetic information is duplicated
• Checkpoints in cell cycle provide opportunities for monitoring the accuracy of deoxyribonucleic acid (DNA) replication
•
• Lecture notes:
•
• We have different types of stem cells and they give rise to other stem cells. one daughter cell then becomes diverse cell types
• The key is that when you’re treating cancer patients is that you’re target stem cells that
are involved. This is the process of chemotherapy.
•
• Proliferation and Differentiation:
•
• Well differentiated cells
o Limited in division and reproduction
➢ Well differentiated neurons
➢ Cells of skeletal and cardiac muscle
•
• Parent or progenitor cells
o Cells that continue to divide and reproduce
➢ Blood cells, skin cells, liver cells
•
• Stem cells
o Undifferentiated
o Can be triggered to enter cell cycle and produce large numbers of progenitor cells when needed
•
• Lecture notes:
•
• Stem cells are capable of giving rise to different cell types in the body
• Well differentiated cell that continues to divide
• Erythroblast becomes a RBC
•
• QUESTION: which of the following cell types is more likely to have arisen from a stem cell in an adult?
• ANSWER: Epithelial cells such as skin, organ lining, and vessel lining cells are
constantly being replaced
•
• Lecture notes:
•
• We need to have a carcinogenic agent or something that’s going to cause us to have changes. This can be a virus, bacteria, smoking, anything!
•
• Carcinogenesis: tumor development that can be described as initiation and progression of the actual cancer. The initiation of any type of cancer is damage to the DNA. This tends to be unrepaired or irreversible damage. There are factors that once there is DNA damage, there are factors or proteins that help stimulate the replication of the DNA that’s damaged. This progression cannot always progress to what we’d like it to be. And in that causes it to becomes a malignant cell.
•
• Cancer malignancies are named on the base of where it arises
•
• Carcinoma: arise from the epithelial tissue
•
• Tumors:
•
• Body organs composed of 2 types of tissues:
•
1. Parenchymal: functional components of an organ
•
2. Supporting tissue: includes the extracellular matrix and connective tissue that surrounds the parenchymal cell (lymphatic’s, blood vessels)
•
• The term anaplasia is used to describe the loss of cell differentiation in cancerous tissue
•
• A mass of cells that arises because of overgrowth
•
• Tumor=mass of cells
•
• Neoplasm
1. Benign: well differentiated cells that are clustered together in a single mass. (Grow slowly, well-defined capsule low mitosis, there’s no metastasis, well differentiated.)
•
2. Malignant: less well differentiated and have the ability to break loose, enter the circulatory or lymphatic system and form secondary malignant tumors at other sites. (Malignant, grows rapidly, no encapsulated, invades local tissue, don’t know where it came from AKA poorly differentiated, constantly recreating, metastasizes.)
•
• • Benign • Malignant
• Cell characteristics • Well differentiated
• Resemble tissue of origin • Undifferentiated
• Anaplasia, atypical structure
• No resemblance to
tissue of origin
• Rate of growth • Progressive, still • Variable
• More differentiated= faster growth
• Mode of growth • Grows by expansion without invading surrounding tissues
• Encapsulates • Grows by invasion
• Infiltrates surrounding tissues
• Metastasis • None • Gains access to blood and lymph channels to metastasize to other
areas
•
•
• Other Characteristics of Malignant Neoplasms:
•
• Tend to grow rapidly and spread widely
• Have the potential to kill regardless of their original location
• Tend to compress blood vessels and outgrow their blood supply, causing ischemia and tissue necrosis
• Rob normal tissues of essential nutrients
• Liberate enzymes and toxins that destroy tumor tissue and normal tissue
o Solid or hematologic
•
• Lecture notes:
•
• Malignant cells go faster and also compress organs. They can travel and metastasize. Normal tissues are robbed of their essential nutrients.
•
• Radiation therapy: purpose is to shrink or kill the cancer. You can try to shrink the tumor first to relieve pressure and then go into surgery to remove it. They’ll also give therapy (adjuvant therapy)
•
• Lactic acid buildup occurs because dead cells are everywhere. The treatment itself can have implications.
•
• Chemotherapy: attacks good and bad cells hence why you lose your hair. It doesn’t differentiate whether it’s a cancer cell or not. This is why you have so many side effects. There is more immunomodulation therapies that target just specific cells therefore patients can have less side affects or complications.
•
• Tumors develop their own capillaries and blood supply for growth so they rob nutrients from other places so they maintain itself by causing its own vasculature.
•
• Types of tumors:
•
• Adding the suffix –oma to the parenchymal tissue type from which the growth originated
•
• Adenoma: benign tumor of glandular epithelial tissue
•
• Adenocarcinoma: malignant tumor of glandular epithelial tissue
•
• Carcinoma: malignant tumor of epithelial tissue
•
• Osteoma: benign tumor of bone tissue
•
• Sarcoma: malignant tumors of mesenchymal origin
•
• Papilloma’s: benign microscopic or macroscopic finger-like projections growing on a surface
•
• Question: Which of the following does not apply to benign tumor cells?
A. A slow, progressive rate of growth that may come to a standstill or regress
B. An expansive manner of growth
C. Liberate enzymes and toxins that destroy tumor tissue and normal tissue
D. Composed of well-differentiated cells that resemble the cells of the tissue of origin
•
• Answer: C. – liberating enzymes and toxins that destroy tumor tissue and normal tissue is an ability that characterizes metastatic tumor cells
•
• Methods by which Cancer Spreads:
•
• Direct invasion and extension
• Seeding of cancer cells in body cavities
• Metastatic spread through the blood or lymph pathways
o Sentinel node: the initial lymph node to which the primary tumor drains. Breast cancer metastasis Is always almost through lymphatic, therefore the extent of the disease is done through lymphatic mapping and sentinel lymph node biopsy.
•
• Lecture notes:
•
• Metastasis: spread of cancer cells from original site. Metastasis spread through blood or lymph nodes.
•
• Common: colon cancer goes to lungs and liver. Liver cancer to lungs. Lung cancer to breast and brain
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
• Mechanism of Tumor Metastasis
•
•
• Lecture notes:
•
• Carcinoma in situ= local invasion of tissue. No spread
• In order for metastasis to occur, the cancer needs to go from local to distant and it must go through the blood supply or lymph nodes
• Digestion of barriers: it eats up everything around it
• Change of cell adhesion that occurs: the cell that starts to supply the tumor is getting its nutrition from elsewhere
• Increase in mobility as well as it enters the lymph nodes that cause it to metastasize.
•
• Factors Affecting Tumor Growth:
•
• Number of cells that are actively dividing
• Duration of the cell cycle
• Number of cells that are being lost compared with the number of new cells being produced
o Cancer cells do not die on schedule, thus, a greater percentage of cells are actively engaged in cycling than in normal tissue.
•
• Lecture notes:
•
• Duration: where in the cell cycle is the multiplication occurring and how long is the cell cycle occurring per cell because each cell cycle is different for each type of cell.
•
• Genes that Control Cell Growth and Replication:
•
• Proto-oncogenes
o Normal genes that become cancer-causing oncogenes
• Tumor suppressor genes
o When less active creates an environment in which cancer is promoted
• Genes that control programmed cell death or apoptosis
• Genes that regulate repair of damage DNA
•
• Lecture notes:
•
• Tumor suppressor genes: also helpful in decreasing the likelihood or replication from occurring. They are essential for the proper functioning of T-lymphocytes that help maintain the immune system. This tries to protect the cell from becoming cancerous.
• Important: in order for cancer to occur, the tumor suppressor genes must be
INACTIVATED.
•
• Host Environmental Factors Leading to Cancer:
•
• Heredity
• Hormones
• Carcinogens
o Chemical
o Radiation
• Oncogenic viruses
• Immunologic mechanisms
• Micro-environmental effects
o Multiple cell types, cytokines, and growth factors
•
• Lecture notes:
•
• Oncogenic viruses—example: HPV
• Bacterial infections—example: H. Pylori
• Cytokines are proteins that serve as messengers. They tell for example, if you’re feeling burned therefore you need to move your hand
• All of these things can cause tumor suppressor genes to become inactive
•
• Clinical Manifestation of Cancer:
•
• Tissue integrity
o Cancer leads to tissue integrity because as it grows, it compresses and erodes blood vessels. This can lead to ulceration and necrosis; frank bleeding and hemorrhage
o Ex. Warning sign for colorectal cancer is blood in the stool.
• Cancer cachexia
o Weight loss and wasting of body fat and muscle tissue; profound weakness, anorexia, and anemia
o People with cancer cachexia respond less to chemotherapy and are more prone to toxic side effects.
• Paraneoplastic Syndromes
o Inappropriate hormone release, circulating hematopoietic, neurological, and dermatological factors
o Can be the earliest indicator that a person has cancer.
•
• Lecture notes:
•
• Cancer cachexia: they are like bones. They have a wasting of complete muscle, fat and profound weakness
• Anorexia= the desire to not eat
• There is a direct correlation with lung cancer and that syndrome. Specific cancers can cause syndromes.
• These syndromes are triggered by the cancer, but they are not caused by the actual cancer
itself
• EX: pancreatic.. They tend to have Cushing syndrome, cancer is not cause it but the symptoms are happening because the cancer is triggering it
•
• Cancer Screening and Health Promotion:
•
• Secondary prevention measure for early recognition of cancer in an otherwise asymptomatic population
o Mammography
o Pap smear
o Colon and rectal exams
o PSA
• Tumor markers
o AFP: liver cancers
o CEA: colorectal, pancreas, lung cancers
o PSA: prostate cancer
o
o Lecture notes:
o
• Secondary prevention: any time you screen. It measures for early recognition of cacner
• Primary prevention: why are you exercising every day? Because I want to stay healthy, keep normal weight. Doing things now to prevent for the future
• Biopsy is the only definitive for diagnosing cancer.
• Tertiary: treatment
o
o Staging and Grading Cancer:
o T (Tumor) o Size and local spread of pr
o N (Nodes) o Involvement of regional lym
o M (Metastasis) o Extend of metastasis
o
o Lecture notes:
o
• Stage is to determine if there is spread
• Grading tells me the size of the tumor and degree of which it is invaded. It also tells me the extent of the spread (is it metastasis or not)
• Tumor staging: (0-3)
o Level 0: no tumor
o Level 1: the tumor is located in one area
o Level 2: there is somewhat of a spread to the neighboring areas
o Level 3: there is tissue involvement
• When I’m looking at nodes: (0-1)
o Level 0: no involvement that are mobile
o Level 1: if its fixed it is scary. This one is fixed.
• Its either 0 or 1. Either you have metastasis or not.
o
o Cancer:
o
• Goals of cancer treatment:
o Curative
o Control
o Palliative
o
• Cancer management
o Surgery
o Radiation
pressure of tumor on organ or surgically remove.
• Goals:
o Chemotherapy
o Hormonal therapy
o Stem cell transplant
o
o Lecture notes:
o
• Hormone targeted: trying to do more
immunomodulation for specific types of cell rather than to affect the entire body
• Stem cell: patients that need bone
marrow transplants
• Ways to give chemo/radiation:
1. Cure
2. Control growth hence why we do radiation or chemo. We look for quality of life
3. Palliative- pain management. Give radiation to relieve
o Induction: shrink tumor
o Adjunct: given after surgical procedures
o Neoadjunct: given before surgery.
[Show More]

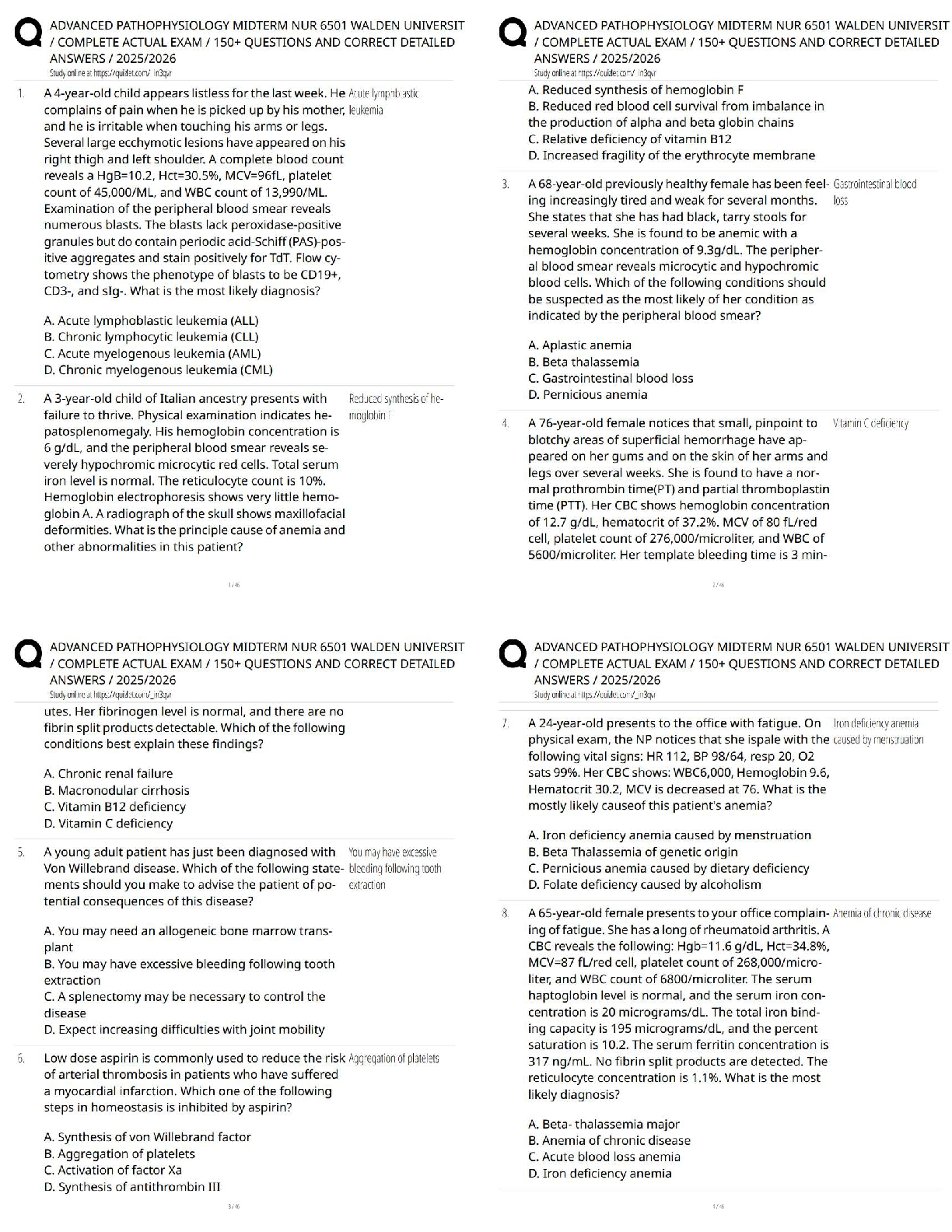

.png)