EMT FISDAP Midterm Exam Study Guide (Latest 2022/2023)
Document Content and Description Below
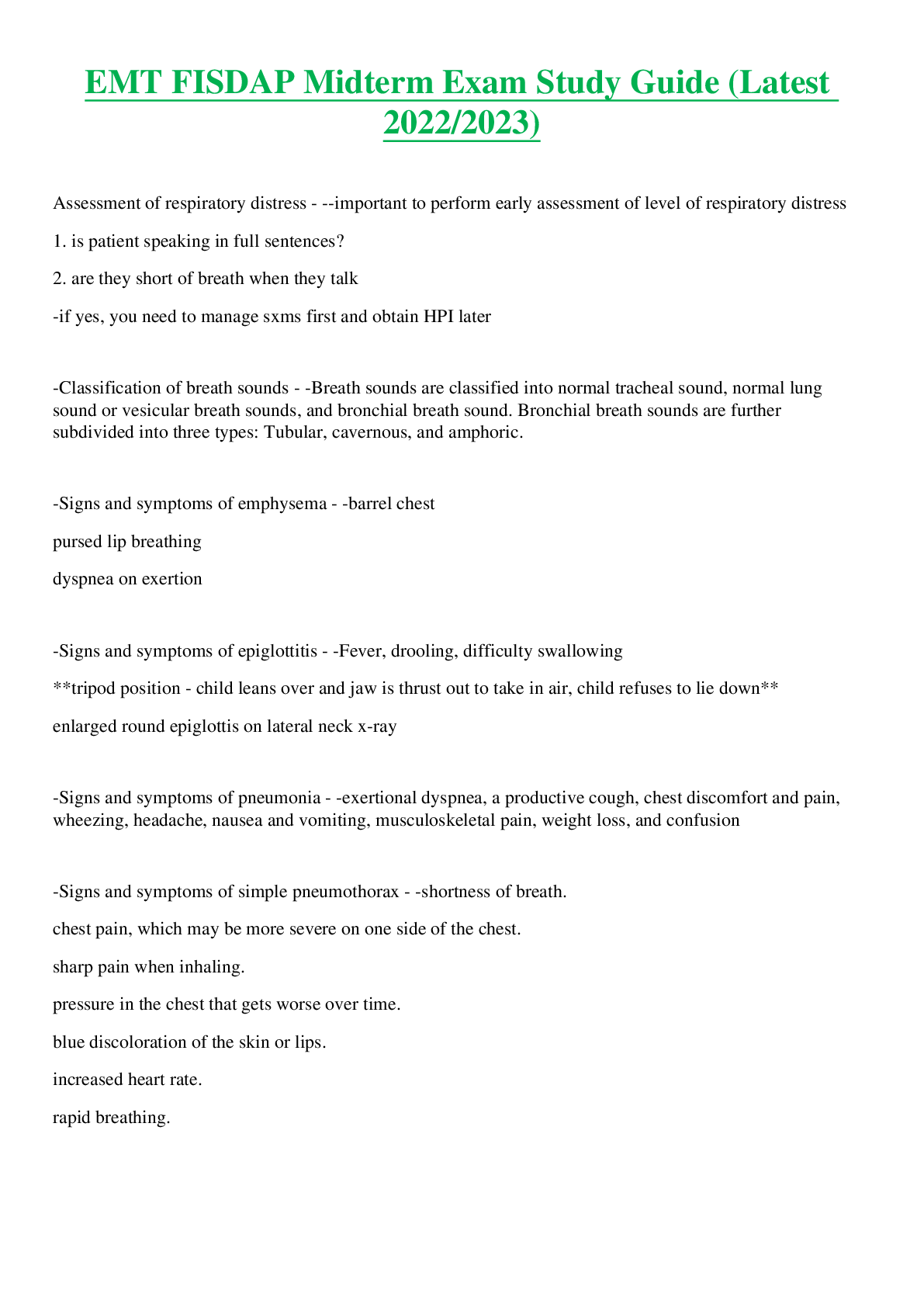
Assessment of respiratory distress - --important to perform early assessment of level of respiratory distress
1. is patient speaking in full sentences?
2. are they short of breath when they talk
-if yes, you need to m
...
[Show More]
Last updated: 3 years ago
Preview 1 out of 11 pages
Instant download
Buy this Document to get the Full Access Instantly
Provided by Students Who Aced it
We Verify Document Content to Gurantee Accuracy
Reviews( 0 )
Document information
Connected school, study & course
About the document
Uploaded On
Apr 10, 2023
Number of pages
11
Written in
All

Additional information
This document has been written for:
Uploaded
Apr 10, 2023
Downloads
0
Views
173
Document Keyword Tags
Recommended For You
Get more on EXAM »
$12
3 Pages
ASM 275 / ASM275 Exam #1 Answers Latest 2022 Already Passed
$16.5
39 Pages
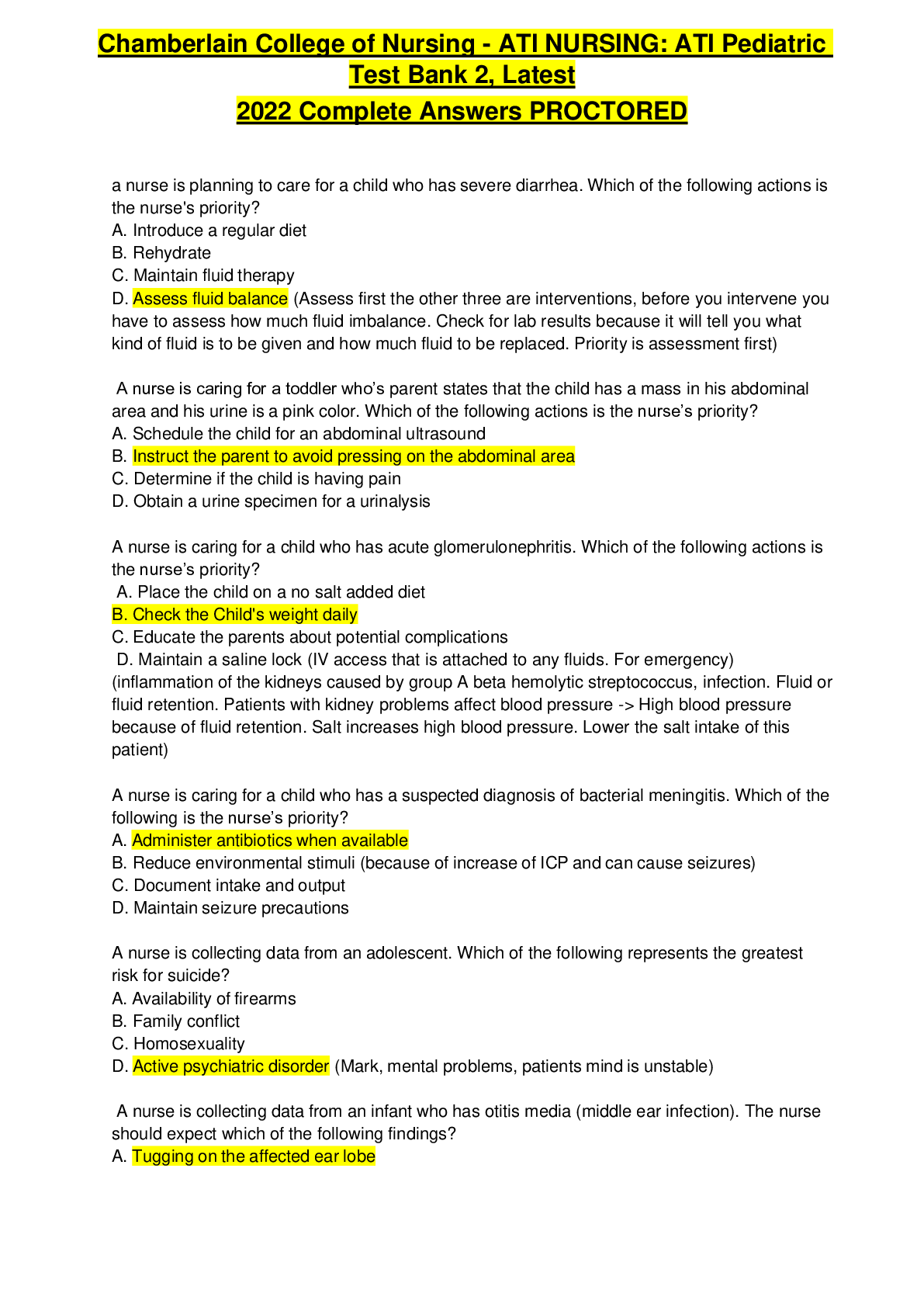
ATI Pediatric Test Bank 2, Latest 2022 Complete Answers PROCTO...


$16
30 Pages
ATI PEDS PROCTORED EXAM | A nurse is preparing to assess a 4-...


$14
23 Pages
NR 511 / NR511 MIDTERM EXAM STUDY GUIDE LATEST 2022 ALREADY PA...
$33
15 Pages
i-human Case Week 7: 57-year-old Cardiovascular High Blood Pre...
More related documents below