NR 602 Peds Quizzes Study Guide Week 2
Developmental Milestones (birth-adolescence)
Birth -1 month
-may lose 5-8% of birth wt but should regain in 10-14 days. >10% requires close
monitoring. Nutrition 110 kcal/kg/day
...
NR 602 Peds Quizzes Study Guide Week 2
Developmental Milestones (birth-adolescence)
Birth -1 month
-may lose 5-8% of birth wt but should regain in 10-14 days. >10% requires close
monitoring. Nutrition 110 kcal/kg/day
-sleep 16/24 hrs day
-Reflexes: sucking, rooting, asymmetric tonic neck, Moro, grasp- should be + and
symmetric.
-Head lag
-Should orient to light and sound, self soothe
-Vision 8-12in from face
1-3month
-Growth spurt 6-8 wks. More defined sleep patterns 15-16 hrs day.
-Fine motor skills: attempt to grasp, visible head control, lifting head off bed when
prone.
-More social, imitate parents expressions- social smile. Can self soothe @ 3 moExtension, non-directed hand swipes, rooting reflex
4-5 months
4-6 months, infant doubles birth weight.
-Social smile
-Begins babbling
-More consistent sleep w/ 5 feedings and 1 @ night. Grasping and holding bottle.
Roll, stronger head control with no head lag when pulled to sitting.
-Hands to mouth, swing @ toys
-Recognize parents meeting needs w/ breast or bottle.. Sleep thru night w/o feeding.
6-8 months
-Teething around 6 mo-8 mo, 1st illness can erupt at this time.
-Crawling. Growth may slow down with adding solids into diet.
-Vocalization increases. “mama” “dada”
-Use gestures (pointing, reaching). Stranger and separation anxiety may appear.
Understands cause and effect relationship.
-Introduce solid foods @ 6 mo.
-Palmar grasp, pass things from hand to hand
-Sits independently, rolls over, supports wt, bounces when held.
9-12 months
-child proof house.
-Separation anxiety/stranger
-Understands simple commands, imitation, gives to on request,
-Understands gestures like bye-bye/peek a boo-Feeds self/ Pincer grasp
-Crawls and cruises around furniture, pull to stand, bears weight
12 mo: 15 mo
-Can use sippy -Feeds self w/ spoon
-Stands & walks independently -Drinks from cup
-Points/clasps hands together -Follows commands
-Knows @ least 3-4 words, knows name w/ gestures
-Growth rate slows -knows 4-6 words
*Health maintenance: check for anemia and lead
18 mo. 24 mo (2yr)
-Turns page of book -Runs, throws, kicks
-Walk up steps -uses spoon, scribble
-Knows 10-20 words -2-3 word sentences
-Point @ body parts -up stairs w/ same
-Pushes & pulls toys foot
-Walks well independently -Temper, “No”
-Toilet training,
transitional toy
-Speech understood
by family
36 mo (3yr) 42 mo (4 yr)
-Full name, age, sex -Understand #
-Speaks in complete sent. 3-5 words -Hops on foot
-Knows 3 #’s and colors -Future & past tense
-Copies a circle -Tells stories
-Builds towers/rides tricycle -Copies a cross +
-Imagination play -Little help w/ dress
-“Oedipal stage”- interested in opposite sex
-Group play, does not like to take turns or share
-Speech understood by stranger
60 mo (5 yr) 6 yr (Kindergarten)
-Counts 10 or more things -Rides bike
-Speaks clearly -Copies triangle
-Puts shoes on and ties laces -Ties shoes
-Prints own name
-Bathes self
-Can draw person w/ 6 body parts
7-11( Middle Childhood)
-Succeed in school and interact w/ peer group
-Thinks of futurePURPLE cryingPeak of crying
Unexpected
Resists soothing
Pain-like face
Long lasting
Evening
Fontanelles- 12 months- not palpapble. Anterior closes by 18-19 months
Pediatric Physical Exam:
Gestational and birth history (including maternal gestational history, smoking,
and illicit drug use)
Immunizations
Hospitalizations
Major illnesses or trauma (includes fractures, stitches, et cetera)
Family history of disease
Social: who the child lives with, members of the household in the home and
ages, smoking in the home, electricity and clean water access, parents or
guardians education and reading level, current school attending if appropriate,
smoking,drug, or alcohol use in child, if appropriate, sexual activity in child, if
appropriate, piercings or tattoos, if appropriate.
-The American Academy of Pediatrics recommends well-child visits at 2 weeks
and then at 2, 4, 6, 9, 12, 15, 18, and 24 months, annually up to age 6, and every
2 years from age 6 through adolescence
2. Puberty (pg 121)
-Biologic process that ultimately leads to fertility
-Adolescence defintion: psychosocial & emotional transition from childhood to
adulthood
-onset of puberty until sexual maturity
Females: earlier than males
-ovaries increase in size, breast budding btw 9-10, breast buds 6 months
before pubic hair, menstrual cycle 10-.5-14.5 yrs. Decrease in lean body mass and
increase body fat.
Males: initial sign is testicular enlargement avg age 11. Release sperm age 13.5-14.5,
elong and widening of penis, rapid height growth, hair growth, increase muscle
mass and lose body fat.
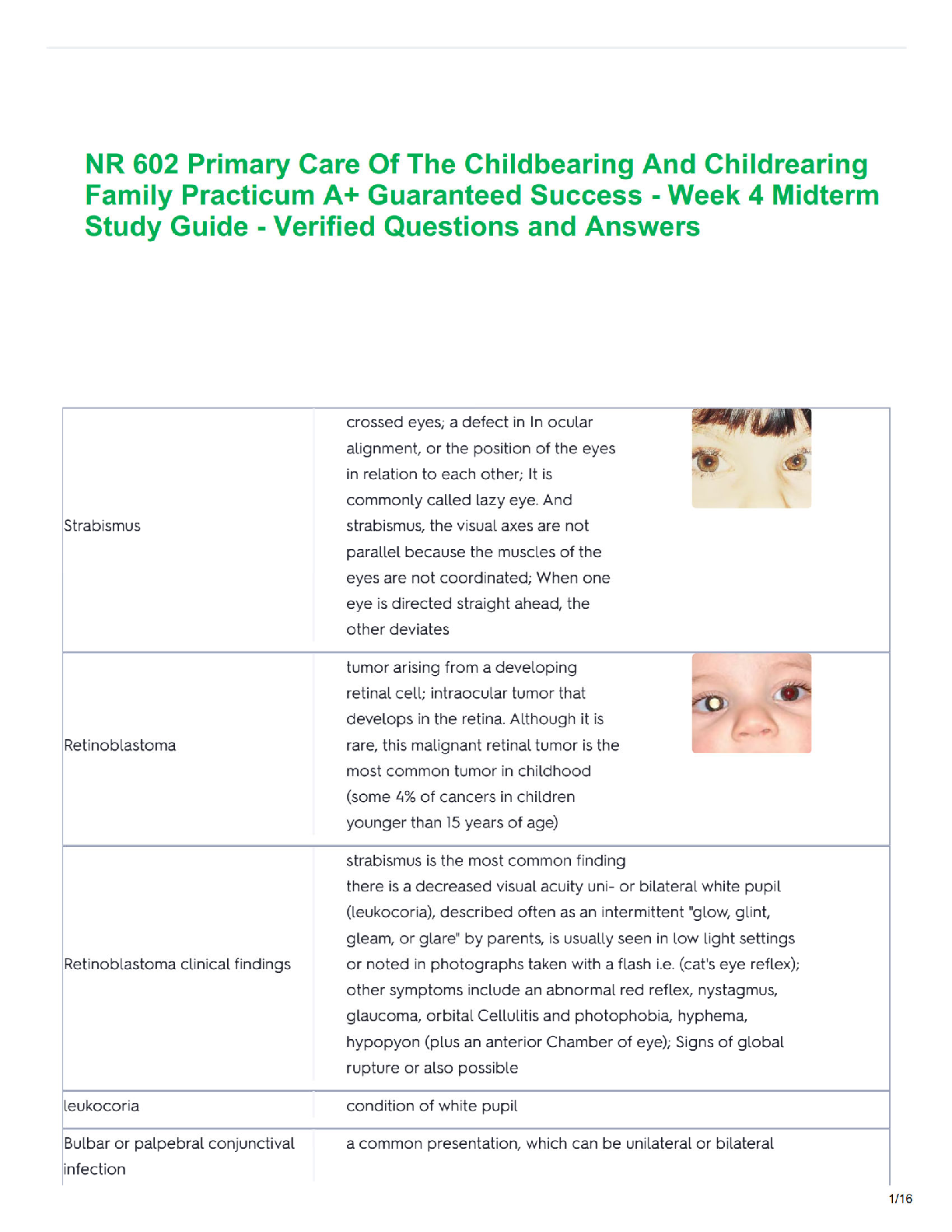
3. Tanner Stages[Leik Book pg 427]
Stage Girls Boys Pubic Hair
I Prepuberty Prepuberty None
II Breast bud Testes enlarge
Rugae on
scrotum
Sparse, few
straight
III Breast & areola-
1 mound
Penis lengthens
Tests continue to
grow
Darker, starts to
curl
IV Breast & areolasecondary
mound
Penis widens Thicker, curly,
dark, coarseV Adult pattern Adult pattern Adult pattern,
spreads to inner
thigh and lower
abd
Adolescence
1. Early Adolescence (11-14yrs)
2. Middle Adolescence (15-17)
3. Late Adolescence (18-21)
4. Growth and Development (birth-17)
-infant loses 5-8% of birth wt but should regain in 2 wks., double birth wt by 6
mo and triple birth wt by 12 mo.
-Infant Weight: 0-6 mo- 6-8 oz/wk and 1 inch per month
6-12 mo- 3-4 oz/wk and ½ inch per month
- Head circumference measured til 36 months , will increase by 12 cm first 12
months
5. Vaccinations
Common side effects of vaccinations are as follows.
Localized erythema, swelling, and pain, particularly with DTaP and Varicella
vaccines
Pain with injection
Low grade fever (Note that activation of the immune system will cause low
grade fever, which is desired in vaccinations.) Currently, there is not enough
evidence to establish that antipyretic use prior to vaccination has benefit and it
may harm antibody response
Vaccine contraindications in childhood:
Any secondary dose of a vaccine after severe allergic reaction to a prior
vaccination.
If the patient has severe combined immunodeficiency (SCID), they should not
have rotavirus, Varicella, measles mumps rubella (MMR), zoster, or live
influenza virus vaccines.
Live influenza virus should also not be used in children with asthma, diabetes,
or cardiac or renal disease. Influenza inactivated injectable vaccine (IIV) can be
used.
-Live viruses not given until 12 months (not effective r/t immature immune system) EX: MMR and
varicella
(Vaccine Breakdown)
Hep B: 1. Birth 2. 1-2 mo 3. 6-18 mo.Rotavirus: 1. 2 mo 2. 4 mo 3. 6 mo
Dtap: 1. 2 mo 2. 4 mo 3. 6 mo 4. 16-18 mo 5. 4-6 yrs
Hib: 1. 2 mo 2. 4 mo 3. 6 mo 4. 12 mo
Pneumoccal (PC4): 1. 2 mo 2. 4 mo 3. 6 mo 4. 12-15 mo
Inactivated polio (IPV) 1. 2 mo 2. 4 mo 3. 6-18 mo 4. 4-6 yrs
MMR 1. 12 mo 2. 4-6 yr
Varicella 1. 12 mo 2. 4-6 yr
----Flu vaccine can be given @ 6 mo.
6. Dermatology
A. Contact Dermatitis- acute or chronic inflammation resulting from a
hypersensitive reaction to a substance.
a. Dry skin, nickel, lip licker, plants, latex
b. Diaper dermatitis, allergic dermatitis
-TX: recognize and eliminate agent, tx inflammation. Refer to derm
if not cleared up in 2-3 wks.-burrow solution, oatmeal bath, cool compress, topical
corticosteroid, oral corticosteroids, antihistamines.
B. Diaper Dermatitis- most frequent contact dermatitis
-Erythema, edema and vesiculation
-TX: Clean and dry diaper area, frequent diaper changes, greasy
lubricant if skin is dry, protective barrier, sitz baths, air diaper area, burrow
solution, hydrocortisone TID for 5 days, increase fluids, if no response after 3
days, add topical antifungal (clotrimazole)
C. Seborrheic Dermatitis- (cradle cap) overproduction of sebum
-erythematous, flaky to thick crusts of yellow, greasy scales predomin on
the scalp, face, behind the ears, neck, trunk, and diaper area
-TX: antifungal (azoles/selenium sulfide), anti-inflammatories (topical
steroids, topical calcineurin inhibitiors) keratolytics (topical salicylic acid, urea),
mineral oil, ketoconazole shampoos
D. Atopic Dermatitis (eczema)- chronic, pruritic inflamm skin disorder w/
acute and chronic eruptions. Skin cannot act as protective barrier, therefore
excessive dryness, cracking, lichenification, and susceptibility to bacteria, virus,
and fungal infection.
-Sx: dry skin, Acute (itching, redness, papules, vesicles, edema, serous
d/c, crusts, lichenification not usually seen) Chronic ( lichenification, scratch
marks) Dennie lines, allergic shiners, keratosis pilaris (chicken skin)
-Tx: Lubrication, low dose topical steroid for maintenance, high dose
topical steroid for exacerbation, topical calcineurin inhibitors (tacrolimus &
pimecrolimus). Diluted bleach bath, phototherapy
E. Pediculosis (lice)
Tx- pediculides are 1st line. Permethrin 1% (can be used on children 1 mo
and older).
F. Scabies- contagious infestation spread thru close contact and shared
clothing/linen.
Sx- intense itching, worse @ night, rubbing of hands and feet
Tx- Permethrin 5 %- thin layer entire body and rinse 8-14 hrs later, can
repeat in 1 wk. Antihistamines, tx family, wash linens, clothingHives (urticaria)-
Urticaria- usually involves superficial dermis. Result of complex of
immunologically mediated antigen-antibody response to release of histamine
from mast cells and other vasoactive mediators.
Sx- mild, erythematous, annular raised wheals w/ pale center from 2mm to
several in diameter, blanch w/ pressure, intensify w/ heat, papulovesicular
lesions
Tx- remove offending agent, oral histamines, topical antiprutics, aqueous epi,
prednisone
Ticks- transferred by infected ticks. 3 stages of Lyme disease
1. Stage 1- 1-2 wks after bite, rash @ site. EM rash begins as red annular
macule or pauple @ site of bite that progresses in 24-48 hrs and
makes a bulls eye. Flu like sx, fever, malaise, HA, arthralgia, myalgia,
and stiff neck.
2. Stage 2- early disseminated disease. Neurologic: frequent HA,
lethargy, neck ain, mood swing, irritability, neuralgia, paraesthesia,
motor or sensory impairment, cardiac, and general illness
manifestisation.
3. Stage 3- late disease. Arthritis, chronic neuro sx- memory loss, tingling
of hands and feet
Tx- doxycycline, amoxicillin
Tinea Capitis- ringworm of the head. Fungus invades scalp and hair shaft
causing inflamm response and hair shaft fragility.
-caused by sharing hats, combs, brushes, cats/dogs.
-SX- scaling, erythema, or crusting, bald patches or areas of broken hair,
black-dot tinea, occipital or posterior cervical adenopathy
TX- griseofulvin ultramicrosize 10-15 mg/kg/day 6-8 wks w/ fatty food (ice
cream/milk to enhance absorpt),shampoo w/ selenium sulfide 2.5% or
econazole/ketoconazole, prednisone for keroin
Hemangioma- superficial, deep, or mixed. Present @ birth but emerge 2-3 wks,
SX- Pale macule, telangiectatic lesion or bright red nodular papule. Later go thru
proliferative stage where they grow and form a nodular mass.TX- steroids during prolif stage (because of interference of physiologic fx),
surgery, cryo, radiation, or sclerosing agent.
Upper Resp Infection- common cold
Viral infection of nasal mucosa initiates host response and produces sx of a cold.
SX- nasal congestion, cough, sneezing, rhinorrhea, fever, hoarseness, and
pharyngitis. Should decrease @ 10 days.
-Gradual onset, rhinorrhea is key, sore throat, mild cough/poor sleep, low grade
fever, reddened conjunctiva, red nose, red throat, ant cervical lymphadenopathy
with movable nodes.
TX- supporative tx….NO ABX, saline nose drops, increase fluids, bulb syringe
Dacryocystitis- nasaolacrimal duct obstruction, prevents tears from flowing into
opening in the nasal mucosa, infection can result. Occurs in neonates but can occur
secondary to trauma to the duct or by complicated URI. More common in those w/
craniofacial disorder, Downs. **Resolves spontaneously.
SX- continuous or intermit tearing, stickiness, blepharitis, tender and swelling over
lacrimal duct, eyelids stuck shut, fever, conjunctival injection.
TX- massage lacrimal sac 10 x 2-3x day, erythromycin, tobramycin, or
fluoroquinolones, saline nasal drops followed by aspiration before feeding and
bedtime.
Otitis externa- (swimmers ear)- inflamm of EAC that can involve pinna or TM. Result
from damaged mechanical or chemical mechanisms, retained moisture acidc
environment, chronic swimming pool, excessive cleaning of ears
SX- pain with movement of tragus, swollen EAC making visualization of TM
impossible, occasional regional lymphadenopathy, raised area of induration that can
be deep and diffuse or superficial, red crusty or spreading lesions, thick otorrhea
TX- ear drops with acetic acid or abx w/ or w/o corticosteroid, should improve in 7
days. Do not use neomycin, polymyxin or hydrocortisone drops if TM is not intact
(can damage cochlea) Quinolones are effective against pseudomonas, aureus &
pneumonia.
Acute Otitis Media- acute infection of the middle ear. RSV and influenza 2 viruses
most responsible
SX- rapid onsent of sx, ear pain, irritability, otorrhea, fever, bulging TM, decreased
translucency of TM, erythema or amber is indicitve of effusion
Risk factors- prematurity, unimmunized, breastfeeding less than 6 months,
overweight, parental smoking, feeding in supine position
TX- Tylenol or ibuprofen, topical analgesics (benzocaine/antipyrine otic drops), abx
(amoxicillin or if amox in the last 30 days augmentin) watchful waiting for 48-72 hrs
before prescribing
OM w/ effusion- can occur after AOM, viral illness, barotrauma, allergies, or
anatomic abnormalities. SX- fullness in the hear, hearing loss, dizziness, popping
TX-3 month watchful waitingQuiz Week 3—
Respiratory infections
URI- iral infection of rhinovirus or coronaviruses. Peak winter and spring.
Sx- congestion, sore throat, rhinorrhea
Tx- hydration, OTC pyretics, normal saline rineses of the nares
Complications—OM and sinusitis
Foreign body aspiration- know sx; interpret scenario
Hx- rapid onset of hoarseness, sudden episode of cough, unilateral wheeze and
recurrent pneumonia.
Dx- CXR- local emphysema- area that does not inflate or deflate, suspect FB
aspiration. Bronchoscopy or direct laryngoscopy
Refer to pulmon.
Restrictive airway disease- decrased lung compliance with relatively normal flow
rates. Key findings are rapid RR and decreased tidal volume/capacity.
Sinusitis- cannot be dx until 10-14 days w/ lack of symptom improvement or dev or
new sx such as facial pain. Severe onset of worsening course after 10 days w/o
clinical improvement requires oral abx.
Tx- watchful wait or amoxicillin w/ or w/o clauvunate
Pneumonia-pg 823- Sx
-lower resp tract infect ass w/ fever and resp sx involving the parenchyma of the
lung.
Risk factors- male gender, low SES, poor nutrition, lack of breast feeding, smoke
exposure, drug/alcohol use, GERD, tracheosophageal fistula, immunodeficiency.
Sx- fever, cough, tachypnea,….60 breaths/min infant’s <2, 50 breaths/min in
children 2 to 11 months, 40 breaths/min age 1-5increased work of breathing,
hypoxia, nasal flaring, rales, retraction, rhonchus lung sounds
Dx- CXR for 3 yrs and > who does not improve in 72 hrs on standard tx.
Tx- azithromycin or amoxicillin
Bronchiolitis-pg 817- disease that causes inflamm, necrosis, and ededma of resp
epithelial cells in lining of aiways. Most commonly caused by respiratory syncytial
virus (RSV). Common in children < 2. Contagous, spread thu droplet.
Sc- URI sx of cough coryza, rhinorrhea, progresses over 3-7 days, gradual resp
distress noisy raspy breathing, audible exp wheeze, low grade to mod fever,
decrease in appetite. Worsening fever with bacterial infection.
Tachypnea, retractions, exp wheeze, fine/coarse crackeles
Dx- CXR if needed.
Tx- supportive care, supplemental O2
Asthma-chronic resp disease characterized by periods of coughing, wheezing, resp
distress, and bronchospasm. Pathophys: result of immunohistopathologi responsesthat produce shedding of airway epithelium and collagen deposits beneath the
basement membrane.
Factors that precipitate- viral/bacterial infections, exposure to known irritants,
GERD, tobacco smoke, environmental changes, exercise, AR/sinusitis, drugs, food,
allergies- dust, mites
Sx- wheezing, continuous/persistent cough, long expiratory phase, diminished
breath sounds, signs of resp distress- tachypnea, retractions, nasal flaring, accessory
muscles, apprehension, drowsiness, tachycardia, cyanosis of lips
Dx- o2 sat, PFT- spirometry
FEV1- amount of air expelled in 1 sec FVC
>75%- normal 80-120%- normal
60-75 mild obstruct 70-79%- mild
50-59% moderate obstruct 50-69%- moderate
<49% severe obstruct <50%- severe
Levels of Severity pg 567
Mild -Wheezing @ end of expiration or no
wheezing
-No or minimal intercostal retraction
along posterior axillary line
-slight prolongation of expiratory phase
-normal aeration in al lung fields
-can talk in sentences
Moderate -Wheezing throughout expiration
-Intercostal retractions
-Prolonged expiratory phase
-Decreased breath sounds at the base
Severe -Use of accessory muscles plus lower rib
and suprasternal retractions, nasal
flaring
-inspir and expir wheezing or no
wheezing heard w/ poor air exchange
-suprasternal retractions w/ abd
breathing
-decreased breath sounds throughout
base
Impending resp arrest -Diminished breath sounds over entire
lung field
-tiring, inability to maintain resp
-severely prolonged expiration if breath
sounds are heard
-drowsy, confused
See pg 572/573 for table and stepwise treatment.
Rotavirus-viral gastroenteritisTransmit- fecal-oral, inanimate objects
Dx-enzyme immunoassay and latex agglutination
Duration- 3-8 days
Sx- acute-onset of fever vomiting and watery diarrhea occur 2-4 days later in
children older than 5 and those 3-24 mo.
Tx- supportive, replace electrolytes
Rotavirus vaccine, hygiene and diapering
SalmonellaTransmit- contaminated eggs, poultry, unpasteurized milk, juice, cheese, raw fruits,
veggies, fecal contam of water
Dx-stool cultures- + leukocytes gross blood
Duration-1-3 days
Sx- diarrhea, fever, abd cramps, rebound tenderness, vomiting
Tx- supportive care- Abx for infants < 3 mo. Use ampicillin, amoxicillin, azithromycin
or bactrim
Clostridium difficile
-Transmission- environment or stool of other colonized or infected ppl by fecal-oral
route.
Sx- mild to explosive diarrhea, bloody stools, abd pain, fever, N/V, watery diarrhea
low grade fever/abd pain
Dx- stool cultures, enzyme immunoassay for toxin a, or A and B, gross blood,
leukocytes
Tx- D/c current Abx, Fluid and electrolyte replacement, supplement w/ probiotics
Complications- pseudomembranous colitis, toxic megacolon, colonic perf, relapse,
intractable proctitis
Cryptosporidium- illness caused by protozoan parasaite cryptosporidium
Sx- watery diarrhea, abd cramps, loss of appetite, low-grade fever, N/V. Sx can last
for up to 2 wks sometimes 4.
Tx- supportive
Pyloric stenosis- pg 1102 *hungry after vomiting
-narrowed pyloric sphincter r/t hypertrophied pyloric muscle
-first born Caucasian males, familial in nature
Hx- regurg and non-projectile vomit in first few wks of life, 2-3 wks old then
projectile, insatiable appetite w/ wt loss, dehydration, and constipation
-May feel olive mass in the epigastrium, right of midline
Dx-US
Tx- surgical intervention
Pinworms- pg 884 Know Sx
Transmission-Fecal-oral contact w/ eggs or cytsts excreted from the initial vector
via ingestion of contaminated food or waterSx- perirectal/vaginal pruritus, nervous irritability, yperactivity, insominia,
urthritis, vaginitis, salpingitis, pelvic peritonitis
Can cause chronic health and nutritional problems that impair physical and mental
growth
Tx- mebendazole, pyrantel pamoate repeat in 2 wks, morning baths, change
bedding, hand hygiene, clip fingernail,s avoid scratching
GERD- pg 845- Sx, Education, Tx
-passage of gastric contents into esophagus from stomach through LES.
Sx-esophagitis, irritability, arching, choking, gagging, feeding aversion, FTT sx,
stridor lower airway disease, sinusitis, hoarseness, dysphagia, odoynophagia,
halitosis
DX- endoscopy, barium upper GI, radionuclide scan
Tx- PPIs- promote mucosal healing
HR2
Thickening agents, avoid eating 2 hrs before bed, weight management
Surgery- fundoplication
EDU- usually self-limiting and sx improve as child grows, may temporarily worsen
during illness
UTI pg 915
-asymptomatic bacteruria- bacteria in urine w/o other sx, benign, no renal injury
-cystitis- infection of the bladder that produces lower tract sx but does not cause
fever or renal injury
-pyelonephritis- most severe, involving renal parenchyma or kidney, must be tx to
prevent irreversible renal damage
Physical exam- flank pain/CVA tenderness, suprapubic tenderness, bladder
distendtion, mass from fecal impaction, vaginal erythema, edema, irritation, labial
adhesion, uncircumcised male, urethral ballooning
Sx- fever, irritability, vomiting
Dx-sterile bag, straight cath or CC UA, > 100,000 colonies of single pathogen via CC,
>50,000 in a cath spec then +
Tx- Bactrim > 2 mos
Amoxicillin
[Show More]





![Preview of WEEK **5 [Chamberlain university]NR 602 IHUMAN Case Week #5 Deborah Arnaudin 54 Year Old](https://browseimages.nyc3.digitaloceanspaces.com/paper-images/2026/03/31/zbQKePwt2026-03-31-11-4669cc328fcad96.png)






.png)