*NURSING > QUESTIONS & ANSWERS > Fortis College, Orange NUR 201exam 1 questions and answers. Graded A (All)
Fortis College, Orange NUR 201exam 1 questions and answers. Graded A
Document Content and Description Below
1. Kyle, age 6 months, is brought to the clinic. His parent says, “I think he hurts. He cries and rolls his head from side to side a lot.” This most likely suggests which feature of pain? a. Typ... e c. Duration b. Severity d. Location The child is displaying a local sign of pain. Rolling the head from side to side and pulling at ears indicate pain in the ear. The child’s behavior indicates the location of the pain. The behavior does not provide information about the type, severity, or duration. PTS: 1 DIF: Cognitive Level: Comprehension REF: 835 OBJ: Nursing Process: Assessment MSC: Client Needs: Physiologic Integrity 2. Physiologic measurements in children’s pain assessment are: a. The best indicator of pain in children of all ages. b. Essential to determine whether a child is telling the truth about pain. c. Of most value when children also report having pain. d. Of limited value as sole indicator of pain. Physiologic manifestations of pain may vary considerably and may not provide a consistent measure of pain. Heart rate may increase or decrease. The same signs that may suggest fear, anxiety, or anger also indicate pain. In chronic pain the body adapts, and these signs decrease or stabilize. These signs are of limited value and must be viewed in the context of a pain-rating scale, behavioral assessment, and parental report. When the child states that pain exists, it does. That is the truth. PTS: 1 DIF: Cognitive Level: Application REF: 828-829 OBJ: Nursing Process: Assessment MSC: Client Needs: Physiologic Integrity 3. The pediatric nurse understands that nonpharmacologic strategies for pain management: a. May reduce pain perception. b. Make pharmacologic strategies unnecessary. c. Usually take too long to implement. d. Trick children into believing they do not have pain. Nonpharmacologic techniques provide coping strategies that may help reduce pain perception, make the pain more tolerable, decrease anxiety, and enhance the effectiveness of analgesics. Nonpharmacologic techniques should be learned before the pain occurs. With severe pain it is best to use both pharmacologic and nonpharmacologic measures for pain control. The nonpharmacologic strategy should be matched with the child’s pain severity and taught to the child before the onset of the painful experience. Some of the techniques may facilitate the child’s experience with mild pain, but the child will still know that discomfort is present. PTS: 1 DIF: Cognitive Level: Analysis REF: 840 OBJ: Nursing Process: Planning MSC: Client Needs: Physiologic Integrity 4. Which drug is usually the best choice for patient-controlled analgesia (PCA) for a child in the immediate postoperative period? a. Codeine c. Methadone b. Morphine d. Meperidine The most commonly prescribed medications for PCA are morphine, hydromorphone, and fentanyl. Parenteral use of codeine is not recommended. Methadone is not available in parenteral form in the United States. Meperidine is not used for continuous and extended pain relief. PTS: 1 DIF: Cognitive Level: Analysis REF: 843 OBJ: Nursing Process: Implementation MSC: Client Needs: Physiologic Integrity 5. A lumbar puncture is needed on a school-age child. The most appropriate action to provide analgesia during this procedure is to apply: a. 4% Liposomal Lidocaine (LMX) 15 minutes before the procedure. b. A transdermal fentanyl (Duragesic) patch immediately before the procedure. c. Eutectic mixture of local anesthetics (EMLA) 1 hour before the procedure. d. EMLA 30 minutes before the procedure. EMLA is an effective analgesic agent when applied to the skin 60 minutes before a procedure. It eliminates or reduces the pain from most procedures involving skin puncture. LMX must be applied 30 minutes before the procedure. Transdermal fentanyl patches are useful for continuous pain control, not rapid pain control. For maximal effectiveness, EMLA must be applied approximately 60 minutes in advance. PTS: 1 DIF: Cognitive Level: Analysis REF: 844 OBJ: Nursing Process: Implementation MSC: Client Needs: Physiologic Integrity 6. The nurse is caring for a child receiving intravenous (IV) morphine for severe postoperative pain. The nurse observes a slower respiratory rate, and the child cannot be aroused. The most appropriate management of this child is for the nurse to: a. Administer naloxone (Narcan). b. Discontinue the IV infusion. c. Discontinue morphine until the child is fully awake. d. Stimulate the child by calling his or her name, shaking gently, and asking the child to breathe deeply. The management of opioid-induced respiratory depression includes lowering the rate of infusion and stimulating the child. If the respiratory rate is depressed and the child cannot be aroused, IV naloxone should be administered. The child will be in pain because of the reversal of the morphine. The morphine should be discontinued, but naloxone is indicated if the child is unresponsive. PTS: 1 DIF: Cognitive Level: Analysis REF: 850 OBJ: Nursing Process: Implementation MSC: Client Needs: Physiologic Integrity 7. When pain is assessed in an infant, it is inappropriate for the nurse to assess for: a. Facial expressions of pain. c. Crying. b. Localization of pain. d. Thrashing of extremities. Infants are unable to localize pain. Frowning, grimacing, and facial flinching in an infant may indicate pain. Infants often exhibit high-pitched, tense, harsh crying to express pain. Infants may exhibit thrashing of extremities in response to a painful stimulus. PTS: 1 DIF: Cognitive Level: Comprehension REF: 829 OBJ: Nursing Process: Assessment MSC: Client Needs: Physiologic Integrity 8. Which myth may interfere with the treatment of pain in infants and children? a. Infants may have sleep difficulties after a painful event. b. Children and infants are more susceptible to respiratory depression from narcotics. c. Pain in children is multidimensional and subjective. d. A child’s cognitive level does not influence the pain experience. No data are available to support the belief that infants and children are at higher risk of respiratory depression when they are given narcotic analgesics. This is a myth. It is true that infants may have sleep difficulties after a painful event. Pain in children is multidimensional and subjective. The child’s cognitive level, along with emotional factors and past experiences, does influence the perception of pain. PTS: 1 DIF: Cognitive Level: Comprehension REF: 850 OBJ: Nursing Process: Evaluation MSC: Client Needs: Physiologic Integrity 9. The nurse caring for the child in pain understands that distraction: a. Can give total pain relief to the child. b. Is effective when the child is in severe pain. c. Is the best method for pain relief. d. Must be developmentally appropriate to refocus attention. Distraction can be very effective in helping to control pain; however, it must be appropriate to the child’s developmental level. Distraction can help control pain, but it is rarely able to provide total pain relief. Children in severe pain are not distractible. Children may use distraction to help control pain, although it is not the best method for pain relief. PTS: 1 DIF: Cognitive Level: Comprehension REF: 840 OBJ: Nursing Process: Planning MSC: Client Needs: Physiologic Integrity 10. What medication is the most effective choice for treating pain associated with sickle cell crisis in a newly admitted 5-year-old child? a. Morphine c. Ibuprofen b. Acetaminophen d. Midazolam Opioids, such as morphine, are the preferred drugs for the management of acute, severe pain, including postoperative pain, post-traumatic pain, pain from vaso-occlusive crisis, and chronic cancer pain. Acetaminophen provides only mild analgesic relief and is not appropriate for a newly admitted child with sickle cell crisis. Ibuprofen is a type of nonsteroidal antiinflammatory drug (NSAID) that is used primarily for pain associated with inflammation. It is appropriate for mild to moderate pain, but it is not adequate for this patient. Midazolam (Versed) is a short-acting drug used for conscious sedation, for preoperative sedation, and as an induction agent for general anesthesia. PTS: 1 DIF: Cognitive Level: Application REF: 858 OBJ: Nursing Process: Implementation MSC: Client Needs: Physiologic Integrity 11. In which developmental stage is the child first able to localize pain and describe both the amount and the intensity of the pain felt? a. Toddler stage c. School-age stage b. Preschool stage d. Adolescent stage The preschool stage is the period when the child is first able to describe the location and intensity of pain, by stating, for example, “Ear hurts bad,” when feeling pain. The toddler expresses pain by guarding or touching the painful area, verbalizes words that indicate discomfort such as “ouch” and “hurt,” and demonstrates generalized restlessness when feeling pain. The school-age child describes both the location of the pain and its intensity. The adolescent also describes the location and intensity of pain. PTS: 1 DIF: Cognitive Level: Application REF: 833 OBJ: Nursing Process: Assessment MSC: Client Needs: Physiologic Integrity 12. Which assessment indicates to a nurse that a 2-year-old child is in need of pain medication? a. The child is lying rigidly in bed and not moving. b. The child’s current vital signs are consistent with vital signs over the past 4 hours. c. The child becomes quiet when held and cuddled. d. The child has just returned from the recovery room. Behaviors such as crying, distressed facial expressions, certain motor responses such as lying rigidly in bed and not moving, and interrupted sleep patterns are indicative of pain in children. Current vital signs that are consistent with earlier vital signs do not indicate that the child is feeling pain. Response to comforting behaviors does not suggest that the child is feeling pain. A child who is returning from the recovery room may or may not be in pain. Most times the child’s pain is under adequate control at this time. The child may be fearful or having anxiety because of the strange surroundings and having just completed surgery. PTS: 1 DIF: Cognitive Level: Application REF: 833 OBJ: Nursing Process: Assessment MSC: Client Needs: Physiologic Integrity 13. When assessing pain in any child, the nurse should consider that: a. Any pain assessment tool can be used to assess pain in children. b. Children as young as 1 year old use words to express pain. c. The child’s behavioral, physiologic, and verbal responses are valuable when assessing pain. d. Pain assessment tools are minimally effective for communicating about pain. Children’s behavioral, physiologic, and verbal responses are indicative when assessing pain. The use of pain measurement tools greatly assists in communicating about pain. The child’s age is important in determining the appropriate pain assessment tool to use. Developmentally appropriate assessment tools need to be used to effectively identify and determine the level of pain felt by a child. Toddlers may use words such as “ouch” or “hurt” to identify pain, but infants and young children may not have the language or cognitive abilities to express pain. Pain assessment tools when used appropriately are successful and efficient in identifying and quantifying pain with children. Behavioral and physiologic signs and symptoms in combination with pain assessment tools are most effective in diagnosing pain levels in children. PTS: 1 DIF: Cognitive Level: Application REF: 840 OBJ: Nursing Process: Assessment MSC: Client Needs: Physiologic Integrity 14. A 2-year-old child has been returned to the nursing unit after an inguinal hernia repair. Which pain assessment tool should the nurse use to assess this child for the presence of pain? a. FACES pain rating tool c. Oucher scale b. Numeric scale d. FLACC tool A behavioral pain tool should be used when the child is preverbal or does not have the language skills to express pain. The FLACC (face, legs, activity, cry, consolability) tool should be used with a 2-year-old child. The FACES, numeric, and Oucher scales are all self-report pain rating tools. Self-report measures are not sufficiently valid for children younger than 3 years of age because many children are not able to self-report their pain accurately. PTS: 1 DIF: Cognitive Level: Application REF: 830 OBJ: Nursing Process: Assessment MSC: Client Needs: Physiologic Integrity 15. A nurse is gathering a history on a school-age child admitted for a migraine headache. The child states, “I have been getting a migraine every 2 or 3 months for the last year.” The nurse documents this as which type of pain? a. Acute c. Recurrent b. Chronic d. Subacute Pain that is episodic and that recurs is defined as recurrent pain. The time frame within which episodes of pain recur is at least 3 months. Recurrent pain in children includes migraine headache, episodic sickle cell pain, recurrent abdominal pain (RAP), and recurrent limb pain. Acute pain is pain that lasts for less than 3 months. Chronic pain is pain that lasts, on a daily basis, for more than 3 months. Subacute is not a term for documenting type of pain. PTS: 1 DIF: Cognitive Level: Comprehension REF: 834 OBJ: Nursing Process: Communication, Documentation MSC: Client Needs: Physiologic Integrity MULTIPLE RESPONSE 16. Which medications are the most effective choices for treating pain associated with inflammation in children (Select all that apply)? a. Morphine b. Acetaminophen (Tylenol) c. Ibuprofen (Advil) d. Ketorolac (Toradol) e. Aspirin , D Ibuprofen, naproxen/naproxen sodium, and ketorolac are all types of NSAIDs, which are used primarily for pain associated with inflammation. Opioids, such as morphine, are the preferred drugs for the management of acute, severe pain, including postoperative pain, post-traumatic pain, pain from vaso-occlusive crisis, and chronic cancer pain. Acetaminophen lacks the antiinflammatory effects of NSAIDs and provides only minimal antiinflammatory relief. Although aspirin is an antiinflammatory medication, because of its association with Reye’s syndrome, its use is not recommended in children. PTS: 1 DIF: Cognitive Level: Analysis REF: 844 OBJ: Nursing Process: Implementation MSC: Client Needs: Physiologic Integrity 17. An appropriate tool to assess pain in a 3-year-old child is the (Select all that apply): a. Visual Analog Scale (VAS) b. Adolescent and pediatric pain tool c. Oucher tool d. Poker Chip Tool e. FACES pain rating scale , D, E The Oucher Tool can be used to assess pain in children 3 to 12 years of age. The Poker Chip Tool can be used to assess pain in children 4 to 12 years of age. The FACES pain rating scale can be used to assess pain for children 3 years of age and older. The VAS is indicated for use with older school-age children and adolescents. It can be used with younger school-age children, although less abstract tools are more appropriate. The adolescent and pediatric pain tool is indicated for use with children 8 to 17 years of age. PTS: 1 DIF: Cognitive Level: Comprehension REF: 831-832 OBJ: Nursing Process: Assessment MSC: Client Needs: Physiologic Integrity 18. The nurse is monitoring a patient for side effects associated with opioid analgesics. Which side effects should the nurse expect to monitor for (Select all that apply)? a. Diarrhea b. Respiratory depression c. Hypertension d. Pruritus e. Sweating , D, E Side effects of opioids include respiratory depression, pruritus, and sweating. Constipation may occur, not diarrhea, and orthostatic hypotension may occur but not hypertension. PTS: 1 DIF: Cognitive Level: Comprehension REF: 850 OBJ: Nursing Process: Implementation MSC: Client Needs: Physiologic Integrity 19. Which dietary recommendations should a nurse make to an adolescent patient to manage constipation related to opioid analgesic administration (Select all that apply)? a. Bran cereal b. Decrease fluid intake c. Prune juice d. Cheese e. Vegetables , C, E To manage the side effect of constipation caused by opioids, fluids should be increased, and bran cereal and vegetables are recommended to increase fiber. Prune juice can act as a nonpharmacologic laxative. Fluids should be increased, not decreased, and cheese can cause constipation so it should not be recommended. PTS: 1 DIF: Cognitive Level: Application REF: 846 OBJ: Nursing Process: Implementation MSC: Client Needs: Physiologic Integrity COMPLETION 20. A dose of oxycodone (OxyContin) 2 mg/kg has been ordered for a child weighing 33 lb. The nurse should administer ______ milligrams of OxyContin. (Record your answer as a whole number.) ANS: 30 The child’s weight is divided by 2.2 to obtain the weight in kilograms. Kilograms in weight are then multiplied by the prescribed 2 mg. 33 lb/2.2 = 15 kg. 15 kg ´ 2 mg = 30 mg. PTS: 1 DIF: Cognitive Level: Application REF: 845 OBJ: Nursing Process: Implementation MSC: Client Needs: Physiologic Integrity 21. The nurse is using the FLACC scale to evaluate pain in a preverbal child. The nurse makes the following assessment: Face: occasional grimace; Leg: relaxed; Activity: squirming, tense; Cry: no cry; Consolability: content, relaxed. The nurse records the FLACC assessment as ________. (Record your answer as a whole number.) ANS: 2 The FLACC scale is recorded per the following table: 0 1 2 Face No particular expression or smile Occasional grimace or frown, withdrawn, disinterested Frequent to constant frown, clenched jaw, quivering chin Legs Normal position or relaxed Uneasy, restless, tense Kicking or legs drawn up Activity Lying quietly, normal position, moves easily Squirming, shifting back and forth, tense Arched, rigid, or jerking Cry No cry (awake or asleep) Moans or whimpers, occasional complaint Crying steadily, screams or sobs, frequent complaints Consolability Content, relaxed Reassured by occasional touching, hugging, or talking to; distractible Difficult to console or comfort PTS: 1 DIF: Cognitive Level: Application REF: 830 OBJ: Nursing Process: Implementation MSC: Client Needs: Physiologic Integrity MATCHING A patient receiving an intravenous opioid analgesic has become apneic. Match the nursing interventions with the step numbers in order from the highest priority (first intervention) to the lowest priority (last intervention). a. Place the patient on continuous pulse oximetry to assess SaO2. b. Administer the prescribed naloxone (Narcan) dose by slow IV push. c. Ensure oxygen is available. d. Prepare to calm the child as analgesia is reversed. 22. Step 1 23. Step 2 24. Step 3 25. Step 4 22. PTS: 1 DIF: Cognitive Level: Application REF: 850 OBJ: Nursing Process: Implementation MSC: Client Needs: Physiologic Integrity NOT: The Narcan prescribed dose should be given first by slow IV push every 2 minutes until the effect is obtained. The second intervention should be assessment of the patientÆs SaO2 status. Oxygen should be made available and administered if the SaO2 status indicates hypoxemia. Finally, the child should be calmed as the analgesia is reversed. 23. PTS: 1 DIF: Cognitive Level: Application REF: 850 OBJ: Nursing Process: Implementation MSC: Client Needs: Physiologic Integrity NOT: The Narcan prescribed dose should be given first by slow IV push every 2 minutes until the effect is obtained. The second intervention should be assessment of the patientÆs SaO2 status. Oxygen should be made available and administered if the SaO2 status indicates hypoxemia. Finally, the child should be calmed as the analgesia is reversed. 24. PTS: 1 DIF: Cognitive Level: Application REF: 850 OBJ: Nursing Process: Implementation MSC: Client Needs: Physiologic Integrity NOT: The Narcan prescribed dose should be given first by slow IV push every 2 minutes until the effect is obtained. The second intervention should be assessment of the patientÆs SaO2 status. Oxygen should be made available and administered if the SaO2 status indicates hypoxemia. Finally, the child should be calmed as the analgesia is reversed. 25. PTS: 1 DIF: Cognitive Level: Application REF: 850 OBJ: Nursing Process: Implementation MSC: Client Needs: Physiologic Integrity NOT: The Narcan prescribed dose should be given first by slow IV push every 2 minutes until the effect is obtained. The second intervention should be assessment of the patientÆs SaO2 status. Oxygen should be made available and administered if the SaO2 status indicates hypoxemia. Finally, the child should be calmed as the analgesia is reversed. Chapter 29: Communication, History, and Physical Assessment MULTIPLE CHOICE 1. The nurse is seeing an adolescent boy and his parents in the clinic for the first time. What should the nurse do first? a. Introduce himself or herself. c. Explain the purpose of the interview. b. Make the family comfortable. d. Give an assurance of privacy. The first thing that nurses must do is to introduce themselves to the patient and family. Parents and other adults should be addressed with appropriate titles unless they specify a preferred name. During the initial part of the interview the nurse should include general conversation to help make the family feel at ease. Next, the purpose of the interview and the nurse’s role should be clarified. The interview should take place in an environment as free of distraction as possible. In addition, the nurse should clarify which information will be shared with other members of the health care team and any limits to the confidentiality. PTS: 1 DIF: Cognitive Level: Application REF: 771 OBJ: Nursing Process: Implementation MSC: Client Needs: Psychosocial Integrity 2. Which action is most likely to encourage parents to talk about their feelings related to their child’s illness? a. Be sympathetic. c. Use open-ended questions. b. Use direct questions. d. Avoid periods of silence. Closed-ended questions should be avoided when attempting to elicit parents’ feelings. Open-ended questions require the parent to respond with more than a brief answer. Sympathy is having feelings or emotions in common with another person rather than understanding those feelings (empathy). Sympathy is not therapeutic in the helping relationship. Direct questions may obtain limited information. In addition, the parent may consider them threatening. Silence can be an effective interviewing tool. It allows sharing of feelings in which two or more people absorb the emotion in depth. Silence permits the interviewee to sort out thoughts and feelings and search for responses to questions. PTS: 1 DIF: Cognitive Level: Application REF: 773 OBJ: Nursing Process: Implementation MSC: Client Needs: Psychosocial Integrity 3. What is the single most important factor to consider when communicating with children? a. The child’s physical condition b. The presence or absence of the child’s parent c. The child’s developmental level d. The child’s nonverbal behaviors The nurse must be aware of the child’s developmental stage to engage in effective communication. The use of both verbal and nonverbal communication should be appropriate to the developmental level. Although the child’s physical condition is a consideration, developmental level is much more important. The parents’ presence is important when communicating with young children, but it may be detrimental when speaking with adolescents. Nonverbal behaviors vary in importance based on the child’s developmental level. PTS: 1 DIF: Cognitive Level: Comprehension REF: 774 OBJ: Nursing Process: Implementation MSC: Client Needs: Psychosocial Integrity 4. What is an important consideration for the nurse who is communicating with a very young child? a. Speak loudly, clearly, and directly. b. Use transition objects such as a doll. c. Disguise own feelings, attitudes, and anxiety. d. Initiate contact with the child when the parent is not present. Using a transition object allows the young child an opportunity to evaluate an unfamiliar person (the nurse). This facilitates communication with this age child. Speaking loudly, clearly, and directly tends to increase anxiety in very young children. The nurse must be honest with the child. Attempts at deception lead to a lack of trust. Whenever possible, the parent should be present for interactions with young children. PTS: 1 DIF: Cognitive Level: Comprehension REF: 775 OBJ: Nursing Process: Implementation MSC: Client Needs: Psychosocial Integrity 5. When introducing hospital equipment to a preschooler who seems afraid, the nurse’s approach should be based on which principle? a. The child may think the equipment is alive. b. The child is too young to understand what the equipment does. c. Explaining the equipment will only increase the child’s fear. d. One brief explanation is enough to reduce the child’s fear. Young children attribute human characteristics to inanimate objects. They often fear that the objects may jump, bite, cut, or pinch all by themselves without human direction. Equipment should be kept out of sight until needed. The child should be given simple concrete explanations about what the equipment does and how it will feel to the child. Simple, concrete explanations help alleviate the child’s fear. The preschooler will need repeated explanations as reassurance. PTS: 1 DIF: Cognitive Level: Analysis REF: 791 OBJ: Nursing Process: Implementation MSC: Client Needs: Psychosocial Integrity 6. Which age group is most concerned with body integrity? a. Toddler c. School-age child b. Preschooler d. Adolescent School-age children have a heightened concern about body integrity. They place importance and value on their bodies and are overly sensitive to anything that constitutes a threat or suggestion of injury. Body integrity is not as important a concern to children in the toddler, preschooler, and adolescent age groups. PTS: 1 DIF: Cognitive Level: Comprehension REF: 776 OBJ: Nursing Process: Planning MSC: Client Needs: Health Promotion and Maintenance 7. An 8-year-old girl asks the nurse how the blood pressure apparatus works. The most appropriate nursing action is to: a. Ask her why she wants to know. b. Determine why she is so anxious. c. Explain in simple terms how it works. d. Tell her she will see how it works as it is used. School-age children require explanations and reasons for everything. They are interested in the functional aspect of all procedures, objects, and activities. It is appropriate for the nurse to explain how equipment works and what will happen to the child. A nurse should respond positively to requests for information about procedures and health information. By not responding, the nurse may be limiting communication with the child. The child is not exhibiting anxiety, just requesting clarification of what will be occurring. The nurse must explain how the blood pressure cuff works so the child can then observe during the procedure. PTS: 1 DIF: Cognitive Level: Comprehension REF: 776 OBJ: Nursing Process: Implementation MSC: Client Needs: Health Promotion and Maintenance 8. When the nurse interviews an adolescent, it is especially important to: a. Focus the discussion on the peer group. b. Allow an opportunity to express feelings. c. Emphasize that confidentiality will always be maintained. d. Use the same type of language as the adolescent. Adolescents, like all children, need an opportunity to express their feelings. Often they will interject feelings into their words. The nurse must be alert to the words and feelings expressed. Although the peer group is important to this age group, the focus of the interview should be on the adolescent. The nurse should clarify which information will be shared with other members of the health care team and any limits to confidentiality. The nurse should maintain a professional relationship with adolescents. To avoid misinterpretation of words and phrases that the adolescent may use, the nurse should clarify terms frequently. PTS: 1 DIF: Cognitive Level: Comprehension REF: 776 OBJ: Nursing Process: Planning MSC: Client Needs: Psychosocial Integrity 9. The nurse is having difficulty communicating with a hospitalized 6-year-old child. What technique may be most helpful? a. Suggest that the child keep a diary. b. Suggest that the parent read fairy tales to the child. c. Ask the parent whether the child is always uncommunicative. d. Ask the child to draw a picture. Drawing is one of the most valuable forms of communication. Children’s drawings tell a great deal about them because they are projections of the child’s inner self. It would be difficult for a 6-year-old child to keep a diary because the child is most likely learning to read. Reading fairy tales to the child is a passive activity involving the parent and child. It would not facilitate communication with the nurse. The child is in a stressful situation and is probably uncomfortable with strangers, not necessarily uncommunicative. PTS: 1 DIF: Cognitive Level: Application REF: 778 OBJ: Nursing Process: Implementation MSC: Client Needs: Psychosocial Integrity 10. The nurse is taking a health history on an adolescent. What best describes how the chief complaint should be determined? a. Ask for a detailed listing of symptoms. b. Ask the adolescent, “Why did you come here today?” c. Use what the adolescent says to determine, in correct medical terminology, what the problem is. d. Interview the parent away from the adolescent to determine the chief complaint. The chief complaint is the specific reason for the child’s visit to the clinic, office, or hospital. Because the adolescent is the focus of the history, this is an appropriate way to determine the chief complaint. A listing of symptoms will make it difficult to determine the chief complaint. The adolescent should be prompted to tell which symptom caused him or her to seek help at this time. The chief complaint is usually written in the words that the parent or adolescent uses to describe the reason for seeking help. The parent and adolescent may be interviewed separately, but the nurse should determine the reason the adolescent is seeking attention at this time. PTS: 1 DIF: Cognitive Level: Application REF: 779 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance 11. Where in the health history should the nurse describe all details related to the chief complaint? a. Past history c. Present illness b. Chief complaint d. Review of systems The history of the present illness is a narrative of the chief complaint from its earliest onset through its progression to the present. The focus of the present illness is on all factors relevant to the main problem, even if they have disappeared or changed during the onset, interval, and present. Past history refers to information that relates to previous aspects of the child’s health, not to the current problem. The chief complaint is the specific reason for the child’s visit to the clinic, office, or hospital. It does not contain the narrative portion describing the onset and progression. The review of systems is a specific review of each body system. PTS: 1 DIF: Cognitive Level: Comprehension REF: 779 OBJ: Nursing Process: Implementation MSC: Client Needs: Health Promotion and Maintenance 12. The nurse is interviewing the mother of an infant. She reports, “I had a difficult delivery, and my baby was born prematurely.” This information should be recorded under which heading? a. Birth history c. Chief complaint b. Present illness d. Review of systems The birth history refers to information that relates to previous aspects of the child’s health, not to the current problem. The mother’s difficult delivery and prematurity are important parts of the past history of an infant. The history of the present illness is a narrative of the chief complaint from its earliest onset through its progression to the present. Unless the chief complaint is directly related to the prematurity, this information is not included in the history of present illness. The chief complaint is the specific reason for the child’s visit to the clinic, office, or hospital. It would not include the birth information. The review of systems is a specific review of each body system. It does not include the premature birth. Sequelae such as pulmonary dysfunction would be included. PTS: 1 DIF: Cognitive Level: Comprehension REF: 780 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance 13. When interviewing the mother of a 3-year-old child, the nurse asks about developmental milestones such as the age of walking without assistance. This should be considered because these milestones are: a. Unnecessary information because the child is age 3 years. b. An important part of the family history. c. An important part of the child’s past growth and development. d. An important part of the child’s review of systems. Information about the attainment of developmental milestones is important to obtain. It provides data about the child’s growth and development that should be included in the history. Developmental milestones provide important information about the child’s physical, social, and neurologic health. The developmental milestones are specific to this child. If pertinent, attainment of milestones by siblings would be included in the family history. The review of systems does not include the developmental milestones. PTS: 1 DIF: Cognitive Level: Comprehension REF: 780 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance 14. The nurse is taking a sexual history on an adolescent girl. The best way to determine whether she is sexually active is to: a. Ask her, “Are you sexually active?” b. Ask her, “Are you having sex with anyone?” c. Ask her, “Are you having sex with a boyfriend?” d. Ask both the girl and her parent if she is sexually active. Asking the adolescent girl if she is having sex with anyone is a direct question that is well understood. The phrase sexually active is broadly defined and may not provide specific information to the nurse to provide necessary care. The word anyone is preferred to using gender-specific terms such as boyfriend or girlfriend. Because homosexual experimentation may occur, it is preferable to use gender-neutral terms. Questioning about sexual activity should occur when the adolescent is alone. PTS: 1 DIF: Cognitive Level: Application REF: 782 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance 15. When doing a nutritional assessment on an Hispanic family, the nurse learns that their diet consists mainly of vegetables, legumes, and starches. The nurse should recognize that this diet: a. Indicates that they live in poverty. b. Is lacking in protein. c. May provide sufficient amino acids. d. Should be enriched with meat and milk. The diet that contains vegetable, legumes, and starches may provide sufficient essential amino acids, even though the actual amount of meat or dairy protein is low. Many cultures use diets that contain this combination of foods. It does not indicate poverty. Combinations of foods contain the essential amino acids necessary for growth. A dietary assessment should be done, but many vegetarian diets are sufficient for growth. PTS: 1 DIF: Cognitive Level: Application REF: 785 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance 16. Which parameter correlates best with measurements of the body’s total protein stores? a. Height c. Skin-fold thickness b. Weight d. Upper arm circumference Upper arm circumference is correlated with measurements of total muscle mass. Muscle serves as the body’s major protein reserve and is considered an index of the body’s protein stores. Height is reflective of past nutritional status. Weight is indicative of current nutritional status. Skin-fold thickness is a measurement of the body’s fat content. PTS: 1 DIF: Cognitive Level: Comprehension REF: 790 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance 17. An appropriate approach to performing a physical assessment on a toddler is to: a. Always proceed in a head-to-toe direction. b. Perform traumatic procedures first. c. Use minimal physical contact initially. d. Demonstrate use of equipment. Parents can remove the child’s clothing, and the child can remain on the parent’s lap. The nurse should use minimal physical contact initially to gain the child’s cooperation. The head-to-toe assessment can be done in older children but usually must be adapted in younger children. Traumatic procedures should always be performed last. These will most likely upset the child and inhibit cooperation. The nurse should introduce the equipment slowly. The child can inspect the equipment, but demonstrations are usually too complex for this age group. PTS: 1 DIF: Cognitive Level: Comprehension REF: 793 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance 18. With the National Center for Health Statistics (NCHS) criteria, which body mass index (BMI)–for-age percentile indicates a risk for being overweight? a. 10th percentile c. 85th percentile b. 9th percentile d. 95th percentile Children who have BMI-for-age greater than or equal to the 85th percentile and less than the 95th percentile are at risk for being overweight. Children in the 9th and 10th percentiles are within normal limits. Children who are greater than or equal to the 95th percentile are considered overweight. PTS: 1 DIF: Cognitive Level: Comprehension REF: 790 OBJ: Nursing Process: Diagnosis MSC: Client Needs: Health Promotion and Maintenance 19. The nurse is using the NCHS growth chart for an African-American child. The nurse should consider that: a. This growth chart should not be used. b. Growth patterns of African-American children are the same as for all other ethnic groups. c. A correction factor is necessary when the NCHS growth chart is used for non-Caucasian ethnic groups. d. The NCHS charts are accurate for U.S. African-American children. The NCHS growth charts can serve as reference guides for all racial or ethnic groups. U.S. African American-children were included in the sample population. The growth chart can be used with the perspective that different groups of children have varying normal distributions on the growth curves. No correction factor exists. PTS: 1 DIF: Cognitive Level: Comprehension REF: 791 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance 20. Which tool measures body fat most accurately? a. Stadiometer c. Cloth tape measure b. Calipers d. Paper or metal tape measure Calipers are used to measure skin-fold thickness, which is an indicator of body fat content. Stadiometers are used to measure height. Cloth tape measures should not be used because they can stretch. Paper or metal tape measures can be used for recumbent lengths and other body measurements that must be made. PTS: 1 DIF: Cognitive Level: Comprehension REF: 795 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance 21. By what age do the head and chest circumferences generally become equal? a. 1 month c. 1 to 2 years b. 6 to 9 months d. 2.5 to 3 years Head circumference begins larger than chest circumference. Between ages 1 and 2 years, they become approximately equal. Head circumference is larger than chest circumference at ages 1 month and 6 to 9 months. Chest circumference is larger than head circumference at age 2.5 to 3 years. PTS: 1 DIF: Cognitive Level: Comprehension REF: 795 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance 22. The earliest age at which a satisfactory radial pulse can be taken in children is: a. 1 year c. 3 years b. 2 years d. 6 years Satisfactory radial pulses can be used in children older than 2 years. In infants and young children the apical pulse is more reliable. The radial pulse can be used for assessment at ages 3 and 6 years. PTS: 1 DIF: Cognitive Level: Comprehension REF: 796 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance 23. Where is the best place to observe for the presence of petechiae in dark-skinned individuals? a. Face c. Oral mucosa b. Buttocks d. Palms and soles Petechiae, small distinct pinpoint hemorrhages, are difficult to see in dark skin unless they are in the mouth or conjunctiva. PTS: 1 DIF: Cognitive Level: Comprehension REF: 803 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance 24. When palpating the child’s cervical lymph nodes, the nurse notes that they are tender, enlarged, and warm. The best explanation for this is: a. Some form of cancer. b. Local scalp infection common in children. c. Infection or inflammation distal to the site. d. Infection or inflammation close to the site. Small nontender nodes are normal. Tender, enlarged, and warm lymph nodes may indicate infection or inflammation close to their location. Tender lymph nodes do not usually indicate cancer. A scalp infection usually does not cause inflamed lymph nodes. The lymph nodes close to the site of inflammation or infection would be inflamed. PTS: 1 DIF: Cognitive Level: Analysis REF: 805 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance 25. The nurse has just started assessing a young child who is febrile and appears very ill. There is hyperextension of the child’s head (opisthotonos) with pain on flexion. The most appropriate action is to: a. Refer for immediate medical evaluation. b. Continue the assessment to determine the cause of neck pain. c. Ask the parent when the child’s neck was injured. d. Record “head lag” on the assessment record and continue the assessment of the child. These symptoms indicate meningeal irritation and need immediate evaluation. Continuing the assessment is not necessary. No indication of injury is present. This is not descriptive of head lag. PTS: 1 DIF: Cognitive Level: Analysis REF: 805 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance 26. The nurse should expect the anterior fontanel to close at age: a. 2 months c. 6 to 8 months b. 2 to 4 months d. 12 to 18 months Ages 2 through 8 months are too early. The expected closure of the anterior fontanel occurs between ages 12 and 18 months; if it closes at these earlier ages, the child should be referred for further evaluation. PTS: 1 DIF: Cognitive Level: Comprehension REF: 805 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance 27. During a funduscopic examination of a school-age child, the nurse notes a brilliant, uniform red reflex in both eyes. The nurse should recognize that this is: a. A normal finding. b. An abnormal finding; the child needs referral to an ophthalmologist. c. A sign of a possible visual defect; the child needs vision screening. d. A sign of small hemorrhages, which usually resolve spontaneously. A brilliant, uniform red reflex is an important normal and expected finding. It rules out many serious defects of the cornea, aqueous chamber, lens, and vitreous chamber. PTS: 1 DIF: Cognitive Level: Knowledge REF: 806 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance 28. Binocularity, the ability to fixate on one visual field with both eyes simultaneously, is normally present by what age? a. 1 month c. 6 to 8 months b. 3 to 4 months d. 12 months Binocularity is usually achieved by ages 3 to 4 months. Age 1 month is too young for binocularity. If binocularity is not achieved by 6 months, the child must be observed for strabismus. PTS: 1 DIF: Cognitive Level: Comprehension REF: 806 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance 29. The most frequently used test for measuring visual acuity is the: a. Denver Eye Screening test. c. Ishihara vision test. b. Allen picture card test. d. Snellen letter chart. The Snellen letter chart, which consists of lines of letters of decreasing size, is the most frequently used test for visual acuity. Single cards (Denver—letter E; Allen—pictures) are used for children age 2 years and older who are unable to use the Snellen letter chart. The Ishihara vision test is used for color vision. PTS: 1 DIF: Cognitive Level: Comprehension REF: 806 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance 30. The nurse is testing an infant’s visual acuity. By what age should the infant be able to fix on and follow a target? a. 1 month c. 3 to 4 months b. 1 to 2 months d. 6 months Visual fixation and following a target should be present by ages 3 to 4 months. Ages 1 to 2 months are too young for this developmental milestone. If the infant is not able to fix and follow by 6 months of age, further ophthalmologic evaluation is needed. PTS: 1 DIF: Cognitive Level: Comprehension REF: 807 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance 31. The appropriate placement of a tongue blade for assessment of the mouth and throat is the: a. The center back area of the tongue. c. Against the soft palate. b. The side of the tongue. d. On the lower jaw. The side of the tongue is the correct position. It avoids the gag reflex yet allows visualization. Placement on the center back area of the tongue elicits the gag reflex. Against the soft palate and on the lower jaw are not appropriate places for the tongue blade. PTS: 1 DIF: Cognitive Level: Comprehension REF: 812 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance 32. What type of breath sound is normally heard over the entire surface of the lungs, except for the upper intrascapular area and the area beneath the manubrium? a. Vesicular c. Adventitious b. Bronchial d. Bronchovesicular Vesicular breath sounds are heard over the entire surface of lungs, with the exception of the upper intrascapular area and the area beneath the manubrium. Bronchial breath sounds are heard only over the trachea near the suprasternal notch. Adventitious breath sounds are not usually heard over the chest. These sounds occur in addition to normal or abnormal breath sounds. Bronchovesicular breath sounds are heard over the manubrium and in the upper intrascapular regions where trachea and bronchi bifurcate. PTS: 1 DIF: Cognitive Level: Comprehension REF: 815 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance 33. What term is used to describe breath sounds that are produced as air passes through narrowed passageways? a. Rubs c. Wheezes b. Rattles d. Crackles Wheezes are produced as air passes through narrowed passageways. The sound is similar when the narrowing is caused by exudates, inflammation, spasm, or tumor. Rubs are the sound created by the friction of one surface rubbing over another. Pleural friction rub is caused by inflammation of the pleural space. Rattles is the term formerly used for crackles. Crackles are the sounds made when air passes through fluid or moisture. PTS: 1 DIF: Cognitive Level: Comprehension REF: 815 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance 34. The nurse must assess a child’s capillary filling time. This can be accomplished by: a. Inspecting the chest. b. Auscultating the heart. c. Palpating the apical pulse. d. Palpating the skin to produce a slight blanching. Capillary filling time is assessed by pressing lightly on the skin to produce blanching and then noting the amount of time it takes for the blanched area to refill. Inspecting the chest, auscultating the heart, and palpating the apical pulse will not provide an assessment of capillary filling time. PTS: 1 DIF: Cognitive Level: Comprehension REF: 816 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance 35. What heart sound is produced by vibrations within the heart chambers or in the major arteries from the back-and-forth flow of blood? a. S1, S2 c. Murmur b. S3, S4 d. Physiologic splitting Murmurs are the sounds that are produced in the heart chambers or major arteries from the back-and-forth flow of blood. S1 is the closure of the tricuspid and mitral valves, and S2 is the closure of the pulmonic and aortic valves, and both are considered normal heart sounds. S3 is a normal heart sound sometimes heard in children. S4 is rarely heard as a normal heart sound. If heard, medical evaluation is required. Physiologic splitting is the distinction of the two sounds in S2, which widens on inspiration. It is a significant normal finding. PTS: 1 DIF: Cognitive Level: Comprehension REF: 818 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance 36. The nurse has a 2-year-old boy sit in “tailor” position during palpation for the testes. The rationale for this position is that: a. It prevents cremasteric reflex. b. Undescended testes can be palpated. c. This tests the child for an inguinal hernia. d. The child does not yet have a need for privacy. The tailor position stretches the muscle responsible for the cremasteric reflex. This prevents its contraction, which pulls the testes into the pelvic cavity. Undescended testes cannot be predictably palpated. Inguinal hernias are not detected by this method. This position is used for inhibiting the cremasteric reflex. Privacy should always be provided for children. PTS: 1 DIF: Cognitive Level: Comprehension REF: 821 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance 37. During examination of a toddler’s extremities, the nurse notes that the child is bowlegged. The nurse should recognize that this finding is: a. Abnormal and requires further investigation. b. Abnormal unless it occurs in conjunction with knock-knee. c. Normal if the condition is unilateral or asymmetric. d. Normal because the lower back and leg muscles are not yet well developed. Lateral bowing of the tibia (bowlegged) is common in toddlers when they begin to walk, not an abnormal finding. It usually persists until all of their lower back and leg muscles are well developed. Further evaluation is needed if it persists beyond ages 2 to 3 years, especially in African-American children. PTS: 1 DIF: Cognitive Level: Comprehension REF: 822 OBJ: Nursing Process: Diagnosis MSC: Client Needs: Health Promotion and Maintenance 38. Kimberly is having a checkup before starting kindergarten. The nurse asks her to do the “finger-to-nose” test. The nurse is testing for: a. Deep tendon reflexes. c. Sensory discrimination. b. Cerebellar function. d. Ability to follow directions. The finger-to-nose-test is an indication of cerebellar function. This test checks balance and coordination. Each deep tendon reflex is tested separately. Each sense is tested separately. Although this test enables the nurse to evaluate the child’s ability to follow directions, it is used primarily for cerebellar function. PTS: 1 DIF: Cognitive Level: Comprehension REF: 823 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance 39. The nurse is meeting a 5-year-old child for the first time and would like the child to cooperate during a dressing change. The nurse decides to do a simple magic trick using gauze. This should be interpreted as: a. Inappropriate, because of child’s age. b. A way to establish rapport. c. Too distracting, when cooperation is important. d. Acceptable, if there is adequate time. A magic trick or other simple game may help alleviate anxiety for a 5-year-old. It is an excellent method to build rapport and facilitate cooperation during a procedure. Magic tricks appeal to the natural curiosity of young children. The nurse should establish rapport with the child. Failure to do so may cause the procedure to take longer and be more traumatic. PTS: 1 DIF: Cognitive Level: Analysis REF: 778 OBJ: Nursing Process: Communication, Documentation MSC: Client Needs: Psychosocial Integrity 40. The nurse must assess 10-month-old infant. The infant is sitting on the father’s lap and appears to be afraid of the nurse and of what may happen next. Which initial action by the nurse would be most appropriate? a. Initiate a game of peek-a-boo. b. Ask the father to place the infant on the examination table. c. Undress the infant while he is still sitting on his father’s lap. d. Talk softly to the infant while taking him from his father. Peek-a-boo is an excellent means of initiating communication with infants while maintaining a safe, nonthreatening distance. The child will most likely become upset if separated from his father. As much of the assessment as possible should be done while the child is on the father’s lap. The nurse should have the father undress the child as needed for the examination. PTS: 1 DIF: Cognitive Level: Application REF: 777 OBJ: Nursing Process: Communication, Documentation MSC: Client Needs: Psychosocial Integrity 41. During a routine health assessment, the nurse notes that an 8-month-old infant has significant head lag. Which is the nurse’s most appropriate action? a. Teach the parents appropriate exercises. b. Recheck head control at the next visit. c. Refer the child for further evaluation. d. Refer the child for further evaluation if the anterior fontanel is still open. Significant head lag after age 6 months strongly indicates cerebral injury and is referred for further evaluation. Reduction of head lag is part of normal development. Exercises will not be effective. The lack of achievement of this developmental milestone must be evaluated. PTS: 1 DIF: Cognitive Level: Application REF: 805 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance MULTIPLE RESPONSE 42. The nurse must check vital signs on a 2-year-old boy who is brought to the clinic for his 24-month checkup. Which criteria should the nurse use in determining the appropriate-size blood pressure cuff (Select all that apply)? a. The cuff is labeled “toddler.” b. The cuff bladder width is approximately 40% of the circumference of the upper arm. c. The cuff bladder length covers 80% to 100% of the circumference of the upper arm. d. The cuff bladder covers 50% to 66% of the length of the upper arm. , C Research has demonstrated that cuff selection with a bladder width that is 40% of the arm circumference will usually have a bladder length that is 80% to 100% of the upper arm circumference. This size cuff will most accurately reflect measured radial artery pressure. The name of the cuff is a representative size that may not be suitable for any individual child. Choosing a cuff by limb circumference more accurately reflects arterial pressure than choosing a cuff by length. PTS: 1 DIF: Cognitive Level: Comprehension REF: 800 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance 43. Which data would be included in a health history (Select all that apply)? a. Review of systems b. Physical assessment c. Sexual history d. Growth measurements e. Nutritional assessment f. Family medical history , C, E, F The review of systems, sexual history, nutritional assessment, and family medical history are part of the health history. Physical assessment and growth measurements are components of the physical examination. PTS: 1 DIF: Cognitive Level: Application REF: 779 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance 44. A school nurse is screening children for scoliosis. Which assessment findings should the nurse expect to observe for scoliosis (Select all that apply)? a. Complaints of a sore back b. Asymmetry of the shoulders c. An uneven hemline d. Inability to bend at the waist e. Unequal waist angles , C, E The assessment findings associated with scoliosis include asymmetry of the shoulder and hips, trouser pant leg length appearing shorter on one side, or an uneven hemline on a skirt, indicating unequal leg length. The child may also complain of a sore back. The child is able to bend at the waist adequately. PTS: 1 DIF: Cognitive Level: Application REF: 822 OBJ: Nursing Process: Evaluation MSC: Client Needs: Health Promotion and Maintenance 45. A nurse is performing an assessment on a school-age child. Which findings suggest the child is receiving an excess of vitamin A (Select all that apply)? a. Delayed sexual development b. Edema c. Pruritus d. Jaundice e. Paresthesia , C, D Excess vitamin A can cause delayed sexual development, pruritus, and jaundice. Edema is seen with excess sodium. Paresthesia occurs with excess riboflavin. PTS: 1 DIF: Cognitive Level: Application REF: 787 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance 46. A nurse is planning to use an interpreter during a health history interview of a non-English speaking patient and family. Which nursing care guidelines should the nurse include when using an interpreter (Select all that apply)? a. Elicit one answer at a time. b. Interrupt the interpreter if the response from the family is lengthy. c. Comments to the interpreter about the family should be made in English. d. Arrange for the family to speak with the same interpreter, if possible. e. Introduce the interpreter to the family. , D, E When using an interpreter, the nurse should pose questions to elicit only one answer at a time, such as: “Do you have pain?” rather than “Do you have any pain, tiredness, or loss of appetite?” Refrain from interrupting family members and the interpreter while they are conversing. Introduce the interpreter to family and allow some time before the interview for them to become acquainted. Refrain from interrupting family members and the interpreter while they are conversing. Avoid commenting to the interpreter about family members because they may understand some English. PTS: 1 DIF: Cognitive Level: Application REF: 774 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance MATCHING Match the assessment examination techniques used when performing an abdominal assessment with the sequential step numbers. Begin with the first technique and end with the last. a. Auscultation c. Inspection b. Palpation d. Percussion 47. Step 1 48. Step 2 49. Step 3 50. Step 4 47. PTS: 1 DIF: Cognitive Level: Application REF: 818 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance NOT: The correct order of abdominal examination is inspection, auscultation, percussion, and palpation. Palpation is always performed last because it may distort the normal abdominal sounds. 48. PTS: 1 DIF: Cognitive Level: Application REF: 819 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance NOT: The correct order of abdominal examination is inspection, auscultation, percussion, and palpation. Palpation is always performed last because it may distort the normal abdominal sounds. 49. PTS: 1 DIF: Cognitive Level: Application REF: 827 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance NOT: The correct order of abdominal examination is inspection, auscultation, percussion, and palpation. Palpation is always performed last because it may distort the normal abdominal sounds. 50. PTS: 1 DIF: Cognitive Level: Application REF: 819 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance NOT: The correct order of abdominal examination is inspection, auscultation, percussion, and palpation. Palpation is always performed last because it may distort the normal abdominal sounds. Chapter 27: Family, Social, Cultural, and Religious Influences on Child Health Promotion MULTIPLE CHOICE 1. What type of family is one in which all members are related by blood? a. Consanguineous c. Family of origin b. Affinal d. Household A consanguineous family is one of the most common types and consists of members who have a blood relationship. The affinal family is one made up of marital relationships. Although the parents are married, they may each bring children from a previous relationship. The family of origin is the family unit that a person is born into. Considerable controversy has been generated about the newer concepts of families (i.e., communal, single-parent or homosexual families). To accommodate these other varieties of family styles, the descriptive term household is frequently used. PTS: 1 DIF: Cognitive Level: Knowledge REF: 732 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance 2. The nurse is teaching a group of new parents about the experience of role transition. Which statement by a parent indicates a correct understanding of the teaching? a. “My marital relationship can have a positive or negative effect on the role transition.” b. “If an infant has special care needs, the parents’ sense of confidence in their new role is strengthened.” c. “Young parents can adjust to the new role more easily than older parents.” d. “A parent’s previous experience with children makes the role transition more difficult.” If parents are supportive of each other, they can serve as positive influences on establishing satisfying parental roles. When marital tensions alter caregiving routines and interfere with the enjoyment of the infant, the marital relationship has a negative effect. Infants with special care needs can be a significant source of added stress. Older parents are usually more able to cope with the greater financial responsibilities, changes in sleeping habits, and reduced time for each other and other children. Parents who have previous experience with parenting appear more relaxed, have less conflict in disciplinary relationships, and are more aware of normal growth and development. PTS: 1 DIF: Cognitive Level: Application REF: 732 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance 3. A 3-year-old girl was adopted immediately after birth. The parents have just asked the nurse how they should tell the child that she is adopted. Which guideline concerning adoption should the nurse use in planning her response? a. Telling the child is an important aspect of their parental responsibilities. b. The best time to tell the child is between ages 7 and 10 years. c. It is not necessary to tell the child who was adopted so young. d. It is best to wait until the child asks about it. It is important for the parents not to withhold information about the adoption from the child. It is an essential component of the child’s identity. There is no recommended best time to tell children. It is believed that children should be told young enough so they do not remember a time when they did not know. It should be done before the children enter school to keep third parties from telling the children before the parents have had the opportunity. PTS: 1 DIF: Cognitive Level: Analysis REF: 734 OBJ: Nursing Process: Implementation MSC: Client Needs: Health Promotion and Maintenance 4. The mother of a school-age child tells the school nurse that she and her spouse are going through a divorce. The child has not been doing well in school and sometimes has trouble sleeping. The nurse should recognize this as: a. Indicative of maladjustment. b. Common reaction to divorce. c. Suggestive of lack of adequate parenting. d. Unusual response that indicates need for referral. Parental divorce affects school-age children in many ways. In addition to difficulties in school, they often have profound sadness, depression, fear, insecurity, frequent crying, loss of appetite, and sleep disorders. Uncommon responses to parental divorce include indications of maladjustment, the suggestion of lack of adequate parenting, and the need for referral. PTS: 1 DIF: Cognitive Level: Application REF: 735 OBJ: Nursing Process: Assessment MSC: Client Needs: Psychosocial Integrity 5. A mother brings 6-month-old Eric to the clinic for a well-baby checkup. She comments, “I want to go back to work, but I don’t want Eric to suffer because I’ll have less time with him.” The nurse’s most appropriate answer is: a. “I’m sure he’ll be fine if you get a good babysitter.” b. “You will need to stay home until Eric starts school.” c. “You should go back to work so Eric will get used to being with others.” d. “Let’s talk about the child care options that will be best for Eric.” “Let’s talk about the child care options that will be best for Eric” is an open-ended statement that will assist the mother in exploring her concerns about what is best for both her and Eric. “I’m sure he’ll be fine if you get a good babysitter,” “You will need to stay home until Eric starts school,” and “You should go back to work so Eric will get used to being with others” are directive statements and do not address the effect of her working on Eric. PTS: 1 DIF: Cognitive Level: Application REF: 738 OBJ: Nursing Process: Implementation MSC: Client Needs: Psychosocial Integrity 6. Which term best describes a group of people who share a set of values, beliefs, practices, social relationships, law, politics, economics, and norms of behavior? a. Race c. Ethnicity b. Culture d. Social group Culture is a pattern of assumptions, beliefs, and practices that unconsciously frames or guides the outlook and decisions of a group of people. A culture is composed of individuals who share a set of values, beliefs, and practices that serve as a frame of reference for individual perceptions and judgments. Race is defined as a division of humankind that possesses traits transmissible by descent and sufficient to characterize it as a distinct human type. Ethnicity is an affiliation of a set of persons who share a unique cultural, social, and linguistic heritage. A social group consists of systems of roles carried out in groups. Examples of primary social groups include the family and peer groups. PTS: 1 DIF: Cognitive Level: Knowledge REF: 748 OBJ: Nursing Process: Assessment MSC: Client Needs: Psychosocial Integrity 7. Which term best describes the emotional attitude that one’s own ethnic group is superior to others? a. Culture c. Superiority b. Ethnicity d. Ethnocentrism Ethnocentrism is the belief that one’s way of living and behaving is the best way. This includes the emotional attitude that the values, beliefs, and perceptions of one’s ethnic group are superior to those of others. Culture is a pattern of assumptions, beliefs, and practices that unconsciously frames or guides the outlook and decisions of a group of people. A culture is composed of individuals who share a set of values, beliefs, and practices that serve as a frame of reference for individual perception and judgments. Ethnicity is an affiliation of a set of persons who share a unique cultural, social, and linguistic heritage. Superiority is the state or quality of being superior; it does not include ethnicity. PTS: 1 DIF: Cognitive Level: Comprehension REF: 746 OBJ: Nursing Process: Assessment MSC: Client Needs: Psychosocial Integrity 8. The Vietnamese mother of a child being seen in the clinic avoids eye contact with the nurse. Considering cultural differences, the best explanation for this is that the parent: a. Feels responsible for her child’s illness. b. Feels inferior to nurse. c. Is embarrassed to seek health care. d. Is showing respect for nurse. In some ethnic groups eye contact is avoided. In the Vietnamese culture an individual may not look directly into the nurse’s eyes as a sign of respect. The nurse providing culturally competent care would recognize that the mother does not feel responsible for her child’s illness, she does not feel inferior to the nurse, and she is not embarrassed to seek health care as reasons for the mother to avoid eye contact with the nurse. PTS: 1 DIF: Cognitive Level: Analysis REF: 748 OBJ: Nursing Process: Assessment MSC: Client Needs: Psychosocial Integrity 9. Health beliefs vary among the cultural groups living in the United States. The belief that health is “a state of harmony with nature and the universe” is common in which culture? a. Japanese c. Native American b. African-American d. Hispanic American Many cultures ascribe attributes of health to natural forces. Many individuals of the Native American culture view health as a state of harmony with nature and the universe. This belief is not consistent with Japanese, African-American, or Hispanic American cultural groups. PTS: 1 DIF: Cognitive Level: Comprehension REF: 747 OBJ: Nursing Process: Planning MSC: Client Needs: Psychosocial Integrity 10. A Hispanic toddler has pneumonia. The nurse notices that the parent consistently feeds the child only the broth that comes on the clear liquid tray. Food items such as Jell-O, Popsicles, and juices are left. What would best explain this? a. The parent is trying to feed child only what child likes most. b. The parent is trying to restore normal balance through appropriate “hot” remedies. c. Hispanics believe that the “evil eye” enters when a person gets cold. d. Hispanics believe that an innate energy called chi is strengthened by eating soup. In several groups, including Filipino, Chinese, Arabic, and Hispanic cultures, hot and cold describe certain properties completely unrelated to temperature. Respiratory conditions such as pneumonia are “cold” conditions and are treated with “hot” foods. This may be true, but it is unlikely that a toddler would consistently prefer the broth to Jell-O, Popsicles, and juice. The evil eye applies to a state of imbalance of health, not curative actions. Chinese individuals believe in chias an innate energy. PTS: 1 DIF: Cognitive Level: Application REF: 747 OBJ: Nursing Process: Implementation MSC: Client Needs: Psychosocial Integrity 11. The nurse discovers welts on the back of a Vietnamese child during a home health visit. The child’s mother says that she has rubbed the edge of a coin on her child’s oiled skin. The nurse should recognize that this is: a. Child abuse. b. A cultural practice to rid the body of disease. c. A cultural practice to treat enuresis or temper tantrums. d. A child discipline measure common in the Vietnamese culture. A cultural practice to rid the body of disease is descriptive of coining. The welts are created by repeatedly rubbing a coin on the child’s oiled skin. The mother is attempting to rid the child’s body of disease. The mother was engaged in an attempt to heal the child. This behavior is not child abuse, a cultural practice to treat enuresis or temper tantrums, or a disciplinary measure. PTS: 1 DIF: Cognitive Level: Comprehension REF: 743 OBJ: Nursing Process: Assessment MSC: Client Needs: Psychosocial Integrity 12. The father of a hospitalized child tells the nurse, “He can’t have meat. We are Buddhist and vegetarians.” The nurse’s best intervention is to: a. Order the child a meatless tray. b. Ask a Buddhist priest to visit. c. Explain that hospital patients are exempt from dietary rules. d. Help the parent understand that meat provides protein needed for healing. It is essential for the nurse to respect the religious practices of the child and family. The nurse should arrange a dietary consultation to ensure that nutritionally complete vegetarian meals are prepared by the hospital kitchen. The nurse should be able to arrange for a vegetarian tray. The nurse should not encourage the child and parent to go against their religious beliefs. Nutritionally complete, acceptable vegetarian meals should be provided. PTS: 1 DIF: Cognitive Level: Application REF: 744 OBJ: Nursing Process: Implementation MSC: Client Needs: Psychosocial Integrity 13. In which cultural group is good health considered to be a balance between yin and yang? a. Asians c. Native Americans b. Australian aborigines d. African-Americans In Chinese health beliefs, the forces termed yin and yang must be kept in balance to maintain health. This belief is not consistent with Australian aborigines, Native Americans, or African-Americans. PTS: 1 DIF: Cognitive Level: Comprehension REF: 746 OBJ: Nursing Process: Assessment MSC: Client Needs: Psychosocial Integrity 14. A young child from Mexico is hospitalized for a serious illness. The father tells the nurse that “the child is being punished by God for being bad.” The nurse should recognize this as: a. A health belief common in this culture. b. An early indication of potential child abuse. c. A misunderstanding of the family’s common beliefs. d. A belief common when fortune tellers have been used. A common health belief in the Mexican-American cultural group is that health is controlled by the environment, fate, and the will of God. This comment has no relation to child abuse. The father would not misunderstand the family’s beliefs. This is a cultural belief. Mexicans may use the services of curanderos (healers), not fortune tellers. PTS: 1 DIF: Cognitive Level: Application REF: 747 OBJ: Nursing Process: Assessment MSC: Client Needs: Psychosocial Integrity MULTIPLE RESPONSE 15. Children are taught the values of their culture through observation and feedback relative to their own behavior. In teaching a class on cultural competence, the nurse should be aware that which factor(s) may be culturally determined (Select all that apply)? a. Degree of competition b. Racial variation c. Determination of status d. Social roles e. Geographic boundaries , C, D Each of these factors is determined by the assumptions, beliefs, and practices of the members of the culture. In cultures that value individual resourcefulness, competition would be acceptable. Status is culturally determined and varies according to each culture. Some ascribe higher status to age or socioeconomic status. Social roles also are influenced by the culture. Race and culture are two distinct attributes. The racial grouping describes transmissible traits, whereas the culture is determined by the pattern of assumptions, beliefs, and practices that unconsciously frames or guides the outlook and decisions of a group of people. Cultural development may be limited by geographic boundaries. It is not the boundaries that are culturally determined. PTS: 1 DIF: Cognitive Level: Analysis REF: 739 OBJ: Nursing Process: Assessment MSC: Client Needs: Psychosocial Integrity 16. A nurse is working in a clinic that serves a culturally diverse population of children. The nurse should plan care, understanding that the following complementary and alternative practices may be used by this patient population(Select all that apply): a. Seeking another doctor’s opinion b. Seeking advice from a curandero or curandera c. Using acupuncture or acupressure as a therapy d. Consulting an herbalist e. Consulting a kahuna , C, D, E The curandero (male) or curandera (female) of the Mexican-American community is believed to have healing powers that are a gift from God. The Asian family may consult an herbalist, knowledgeable in medicines, or perhaps a specialized practitioner of Asian therapies, including acupuncture (insertion of needles) or acupressure (application of pressure). Native Hawaiians consult kahunas and practice ho’oponopono to heal family imbalance or disputes. The nurse may encounter use of these practices. Consulting another doctor would not be a complementary or alternative practice expected in a culturally diverse population. PTS: 1 DIF: Cognitive Level: Application REF: 747 OBJ: Nursing Process: Planning MSC: Client Needs: Psychosocial Integrity 17. A nurse is caring for an African-American child recently admitted to the hospital. The nurse should be aware of which broad cultural characteristics for this child when planning care (Select all that apply)? a. Silence may indicate a lack of trust. b. Maintaining constant eye contact may be viewed as aggressive. c. Self-care and folk medicine do not play a role in health care. d. Illness may be seen as the “will of God.” e. No importance is attached to nonverbal behavior. , B, D A nurse should be aware of the African-American broad cultural characteristics, which include the following: initial eye contact shows respect; maintaining eye contact can be viewed as aggressive, silence may indicate a lack of trust, and illness may be seen as the “will of God.” Self-care and folk medicine are prevalent in this culture, and importance is placed on nonverbal behavior. Chapter 28: Developmental and Genetic Influences on Child Health Promotion MULTIPLE CHOICE 1. The head-to-tail direction of growth is referred to as: a. Cephalocaudal. c. Mass to specific. b. Proximodistal. d. Sequential. The first pattern of development is the head-to-tail, or cephalocaudal, direction. The head end of the organism develops first and is large and complex, whereas the lower end is smaller and simpler, and development takes place at a later time. Proximodistal, or near-to-far, is the second pattern of development. Limb buds develop before fingers and toes. Postnatally the child has control of the shoulder before achieving mastery of the hands. Mass to specific is not a specific pattern of development. In all dimensions of growth, a definite, sequential pattern is followed. PTS: 1 DIF: Cognitive Level: Comprehension REF: 751 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance 2. Which term refers to those times in an individual’s life when he or she is more susceptible to positive or negative influences? a. Sensitive period c. Terminal points b. Sequential period d. Differentiation points Sensitive periods are limited times during the process of growth when the organism will interact with a particular environment in a specific manner. These times make the organism more susceptible to positive or negative influences. The sequential period, terminal points, and differentiation points are developmental times that do not make the organism more susceptible to environmental interaction. PTS: 1 DIF: Cognitive Level: Comprehension REF: 752 OBJ: Nursing Process: Planning MSC: Client Needs: Health Promotion and Maintenance 3. An infant who weighs 7 pounds at birth would be expected to weigh how many pounds at age 1 year? a. 14 c. 18 b. 16 d. 21 In general birth, weight triples by the end of the first year of life. For an infant who was 7 pounds at birth, 21 pounds would be the anticipated weight at the first birthday. Weights of 14, 16, and 18 pounds are less what would be expected for an infant with a birth weight of 7 pounds. PTS: 1 DIF: Cognitive Level: Comprehension REF: 753 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance 4. By what age does birth length usually double? a. 1 year c. 4 years b. 2 years d. 6 years Linear growth or height occurs almost entirely as a result of skeletal growth and is considered a stable measurement of general growth. On average most children have doubled their birth length at age 4 years. One year and 2 years are too young for doubling of length. PTS: 1 DIF: Cognitive Level: Comprehension REF: 753 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance 5. How does the onset of the pubertal growth spurt compare in girls and boys? a. It occurs earlier in boys. b. It occurs earlier in girls. c. It is about the same in both boys and girls. d. In both boys and girls it depends on their growth in infancy. Usually, the pubertal growth spurt begins earlier in girls. It typically occurs between the ages of 10 and 14 years for girls and 11 and 16 years for boys. The average earliest age at onset is 1 year earlier for girls. There does not appear to be a relation to growth during infancy. PTS: 1 DIF: Cognitive Level: Comprehension REF: 753 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance 6. A 13-year-old girl asks the nurse how much taller she will become. She has been growing about 2 inches per year but grew 4 inches this past year. Menarche recently occurred. The nurse should base her response on knowing that: a. Growth cannot be predicted. b. The pubertal growth spurt lasts about 1 year. c. Mature height is achieved when menarche occurs. d. Approximately 95% of mature height is achieved when menarche occurs. Although growth cannot be definitely predicted, at the time of the beginning of menstruation or the skeletal age of 13 years, most girls have grown to about 95% of their adult height. They may have some additional growth (5%) until the epiphyseal plates are closed. Responding that the pubertal growth spurt last about 1 year does not address the girl’s question. Young women usually will grow approximately 5% more after the onset of menstruation. PTS: 1 DIF: Cognitive Level: Comprehension REF: 753 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance 7. A child’s skeletal age is best determined by: a. Assessment of dentition. c. Facial bone development. b. Assessment of height over time. d. Radiographs of the hand and wrist. The most accurate measure of skeletal age is radiologic examination of the growth plates. These are the epiphyseal cartilage plates. Radiographs of the hand and wrist provide the most useful screening to determine skeletal age. Age of tooth eruption varies considerably in children. It would not be a good determinant of skeletal age. Assessment of height over time will provide a record of the child’s height, not skeletal age. Facial bone development does not reflect the child’s skeletal age, which is determined by radiographic assessment. PTS: 1 DIF: Cognitive Level: Knowledge REF: 754 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance 8. Trauma to which site can result in a growth problem for children’s long bones? a. Matrix c. Calcified cartilage b. Connective tissue d. Epiphyseal cartilage plate The epiphyseal cartilage plate is the area of active growth. Bone injury at the epiphyseal plate can significantly affect subsequent growth and development. Trauma or infection can result in deformity. The matrix, connective tissue, and calcified cartilage are not areas of active growth. Trauma in these sites will not result in growth problems for the long bones. PTS: 1 DIF: Cognitive Level: Knowledge REF: 753 OBJ: Nursing Process: Diagnosis MSC: Client Needs: Health Promotion and Maintenance 9. Lymphoid tissues such as lymph nodes are: a. Adult size by age 1 year. b. Adult size by age 13 years. c. Half their adult size by age 5 years. d. Twice their adult size by age 10 to 12 years. Lymph nodes increase rapidly and reach adult size at approximately age 6 years. They continue growing until they reach maximal development at age 10 to 12 years, which is twice their adult size. A rapid decline in size occurs until they reach adult size by the end of adolescence. PTS: 1 DIF: Cognitive Level: Knowledge REF: 754 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance 10. Which statement is true about the basal metabolic rate (BMR) in children? a. It is reduced by fever. b. It is slightly higher in boys than in girls at all ages. c. It increases with the age of child. d. It decreases as proportion of surface area to body mass increases. The BMR is the rate of metabolism when the body is at rest. At all ages the rate is slightly higher in boys than in girls. The rate is increased by fever. The BMR is highest in infancy and then closely relates to the proportion of surface area to body mass. As the child grows, the proportion decreases progressively to maturity. PTS: 1 DIF: Cognitive Level: Comprehension REF: 754 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance 11. A mother reports that her 6-year-old child is highly active and irritable and that she has irregular habits and adapts slowly to new routines, people, or situations. According to Chess and Thomas, which category of temperament best describes this child? a. Easy child c. Slow-to-warm-up child b. Difficult child d. Fast-to-warm-up child This is a description of difficult children, who compose about 10% of the population. Negative withdrawal responses are typical of this type of child, who requires a more structured environment. Mood expressions are usually intense and primarily negative. These children exhibit frequent periods of crying and often violent tantrums. Easy children are even tempered, regular, and predictable in their habits. They are open and adaptable to change. Approximately 40% of children fit this description. Slow-to-warm-up children typically react negatively and with mild intensity to new stimuli and adapt slowly with repeated contact. Approximately 10% of children fit this description. Fast-to-warm-up children is not one of the categories identified by Chess and Thomas. PTS: 1 DIF: Cognitive Level: Comprehension REF: 755 OBJ: Nursing Process: Diagnosis MSC: Client Needs: Health Promotion and Maintenance 12. By the time children reach their twelfth birthday, they should have learned to trust others and should have developed a sense of: a. Identity. c. Integrity. b. Industry. d. Intimacy. Industry is the developmental task of school-age children. By age 12 years, children engage in tasks that they can carry through to completion. They learn to compete and cooperate with others, and they learn rules. Identity versus role confusion is the developmental task of adolescence. Integrity and intimacy are not developmental tasks of childhood. PTS: 1 DIF: Cognitive Level: Knowledge REF: 758 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance 13. The predominant characteristic of the intellectual development of the child ages 2 to 7 years is egocentricity. What best describes this concept? a. Selfishness c. Preferring to play alone b. Self-centeredness d. Inability to put self in another’s place According to Piaget, this age child is in the preoperational stage of development. Children interpret objects and events not in terms of their general properties but in terms of their relationships or their use to them. This egocentrism does not allow children of this age to put themselves in another’s place. Selfishness, self-centeredness, and preferring to play alone do not describe the concept of egocentricity. PTS: 1 DIF: Cognitive Level: Knowledge REF: 758 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance 14. The nurse is observing parents playing with their 10-month-old daughter. What should the nurse recognize as evidence that the child is developing object permanence? a. She looks for the toy the parents hide under the blanket. b. She returns the blocks to the same spot on the table. c. She recognizes that a ball of clay is the same when flattened out. d. She bangs two cubes held in her hands. Object permanence is the realization that items that leave the visual field still exist. When the infant searches for the toy under the blanket, it is an indication that object permanence has developed. Returning blocks to the same spot on a table is not an example of object permanence. Recognizing a ball of clay is the same when flat is an example of conservation, which occurs during the concrete operations stage from 7 to 11 years. Banging cubes together is a simple repetitive activity characteristic of developing a sense of cause and effect. PTS: 1 DIF: Cognitive Level: Knowledge REF: 758 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance 15. What is characteristic of the preoperational stage of cognitive development? a. Thinking is logical. c. Reasoning is inductive. b. Thinking is concrete. d. Generalizations can be made. Preoperational thinking is concrete and tangible. Children in this age group cannot reason beyond the observable, and they lack the ability to make deductions or generalizations. Increasingly logical thought, inductive reasoning, and the ability to make generalizations are characteristic of the concrete operations stage of development, ages 7 to 11 years. PTS: 1 DIF: Cognitive Level: Comprehension REF: 758 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance 16. Which behavior is most characteristic of the concrete operations stage of cognitive development? a. Progression from reflex activity to imitative behavior b. Inability to put oneself in another’s place c. Increasingly logical and coherent thought processes d. Ability to think in abstract terms and draw logical conclusions During the concrete operations stage of development, which occurs approximately between ages 7 and 11 years, increasingly logical and coherent thought processes occur. This is characterized by the child’s ability to classify, sort, order, and organize facts to use in problem solving. The progression from reflex activity to imitative behavior is characteristic of the sensorimotor stage of development. The inability to put oneself in another’s place is characteristic of the preoperational stage of development. The ability to think in abstract terms and draw logical conclusions is characteristic of the formal operations stage of development. PTS: 1 DIF: Cognitive Level: Comprehension REF: 758 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance 17. According to Kohlberg, children develop moral reasoning as they mature. What is most characteristic of a preschooler’s stage of moral development? a. Obeying the rules of correct behavior is important. b. Showing respect for authority is important behavior. c. Behavior that pleases others is considered good. d. Actions are determined as good or bad in terms of their consequences. Preschoolers are most likely to exhibit characteristics of Kohlberg’s preconventional level of moral development. During this stage they are culturally oriented to labels of good or bad, right or wrong. Children integrate these concepts based on the physical or pleasurable consequences of their actions. Obeying rules of correct behavior, showing respect for authority, and knowing that behavior that pleases others is considered good are characteristic of Kohlberg’s conventional level of moral development. PTS: 1 DIF: Cognitive Level: Comprehension REF: 759 OBJ: Nursing Process: Planning MSC: Client Needs: Health Promotion and Maintenance 18. At what age do children tend to imitate the religious gestures and behaviors of others without understanding their significance? a. Toddlerhood c. Older school-age period b. Young school-age period d. Adolescence Toddlerhood is a time of imitative behavior. Children will copy the behavior of others without comprehending any significance or meaning to the activities. During the school-age period most children develop a strong interest in religion. The existence of a deity is accepted, and petitions to an omnipotent being are important. Although adolescents become more skeptical and uncertain about religious beliefs, they do understand the significance of religious rituals. PTS: 1 DIF: Cognitive Level: Comprehension REF: 759 OBJ: Nursing Process: Planning MSC: Client Needs: Health Promotion and Maintenance 19. A toddler playing with sand and water would be participating in _____ play. a. Skill c. Social-affective b. Dramatic d. Sense-pleasure The toddler playing with sand and water is engaging in sense-pleasure play. This is characterized by nonsocial situations in which the child is stimulated by objects in the environment. Infants engage in skill play when they persistently demonstrate and exercise newly acquired abilities. Dramatic play is the predominant form of play in the preschool period. Children pretend and fantasize. Social-affective play is one of the first types of play in which infants engage. The infant responds to interactions with people. PTS: 1 DIF: Cognitive Level: Comprehension REF: 761 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance 20. In what type of play are children engaged in similar or identical activity without organization, division of labor, or mutual goal? a. Solitary c. Associative b. Parallel d. Cooperative In associative play no group goal is present. Each child acts according to his or her own wishes. Although the children may be involved in similar activities, no organization, division of labor, leadership assignment, or mutual goal exists. Solitary play describes children playing alone with toys different from those used by other children in the same area. Parallel play describes children playing independently but being among other children. Cooperative play is organized. Children play in a group with other children who play activities for a common goal. PTS: 1 DIF: Cognitive Level: Comprehension REF: 762 OBJ: Nursing Process: Implementation MSC: Client Needs: Health Promotion and Maintenance 21. The nurse observes some children in the playroom. Which play situation exhibits the characteristics of parallel play? a. Kimberly and Amanda sharing clay to each make things b. Brian playing with his truck next to Kristina playing with her truck c. Adam playing a board game with Kyle, Steven, and Erich d. Danielle playing with a music box on her mother’s lap An example of parallel play is when both children are engaged in similar activities in proximity to each other; however, they are each engaged in their own play, such as Brian and Kristina playing with their own trucks side by side. Sharing clay is characteristic of associative play. A group of children playing a board game is characteristic of cooperative play. Playing alone on the mother’s lap is an example of solitary play. PTS: 1 DIF: Cognitive Level: Analysis REF: 762 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance 22. Three children playing a board game would be an example of: a. Solitary play c. Associative play b. Parallel play d. Cooperative play Using a board game requires cooperative play. The children must be able to play in a group and carry out the formal game. In solitary, parallel, and associative play, children do not play in a group with a common goal. PTS: 1 DIF: Cognitive Level: Comprehension REF: 762 OBJ: Nursing Process: Planning MSC: Client Needs: Health Promotion and Maintenance 23. Which function of play is a major component of play at all ages? a. Creativity c. Intellectual development b. Socialization d. Sensorimotor activity Sensorimotor activity is a major component of play at all ages. Active play is essential for muscle development and allows the release of surplus energy. Through sensorimotor play, children explore their physical world by using tactile, auditory, visual, and kinesthetic stimulation. Creativity, socialization, and intellectual development are each functions of play that are major components at different ages. PTS: 1 DIF: Cognitive Level: Comprehension REF: 762 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance 24. Which statement is true about toy safety? a. Adults should be the only ones who select toys. b. Adults should be alert to notices of recalls by manufacturers. c. Government agencies inspect all toys on the market. d. Evaluation of toy safety is a joint effort between children and adults. Adults should be involved in the selection of toys for children to ensure that they are safe and age appropriate. Once the child is using a toy, the adult should be alert to manufacturer recalls. The child and adult should be involved in the joint process of toy selection. Government agencies do not inspect all toys for sale. The U.S. Consumer Products Safety Commission does keep track of potentially dangerous and recalled toys. Children do not have the ability to determine the safety of a toy. It is the adult’s responsibility. PTS: 1 DIF: Cognitive Level: Comprehension REF: 763 OBJ: Nursing Process: Implementation MSC: Client Needs: Health Promotion and Maintenance 25. What is probably the single most important influence on growth at all stages of development? a. Nutrition c. Culture b. Heredity d. Environment Nutrition is the single most important influence on growth. Dietary factors regulate growth at all stages of development, and their effects are exerted in numerous and complex ways. Adequate nutrition is closely related to good health throughout life. Heredity, culture, and environment all contribute to the child’s growth and development; however, good nutrition is essential throughout the life span for optimal health. PTS: 1 DIF: Cognitive Level: Application REF: 755 OBJ: Nursing Process: Planning MSC: Client Needs: Health Promotion and Maintenance 26. Which strategy would be the least appropriate for a child to use to cope? a. Learning problem solving c. Having parents solve problems b. Listening to music d. Using relaxation techniques Children respond to everyday stress by trying to change the circumstances or adjust to the circumstances the way they are. Strategies that provide relaxation and other stress-reduction techniques should be used. An inappropriate response would be for the parents to solve the problems. Some children develop socially unacceptable strategies such as lying, stealing, or cheating. Learning problem solving, listening to music, and using relaxation techniques are positive approaches for coping in children. PTS: 1 DIF: Cognitive Level: Application REF: 768 OBJ: Nursing Process: Implementation MSC: Client Needs: Psychosocial Integrity 27. The intrauterine environment can have a profound and permanent effect on the developing fetus with or without chromosome or gene abnormalities. Most adverse intrauterine effects are the result of teratogens. The nurse is cognizant that this group of agents does not include: a. Accutane c. Amniotic bands b. Rubella d. Alcohol Amniotic bands are a congenital anomaly known as a “disruption” that occurs with the breakdown of previously normal tissue. Congenital amputations caused by amniotic bands are not the result of a teratogen. Other agents include Dilantin, warfarin, cytomegalovirus, radiation, and maternal PKU. PTS: 1 DIF: Cognitive Level: Comprehension REF: 765 OBJ: Nursing Process: Diagnosis MSC: Client Needs: Physiologic Integrity 28. The karyotype of a person is 47, XY, +21. This person is a: a. Normal male. c. Normal female. b. Male with Down syndrome. d. Female with Turner syndrome. This person is male because his sex chromosomes are XY. He has one extra copy of chromosome 21 (for a total of 47 instead of 46), resulting in Down syndrome. A normal male would have 46 chromosomes. A normal female would have 46 chromosomes and XX for the sex chromosomes. A female with Turner syndrome would have 45 chromosomes; the sex chromosomes would have just one X. PTS: 1 DIF: Cognitive Level: Comprehension REF: 766 OBJ: Nursing Process: Assessment MSC: Client Needs: Physiologic Integrity 29. Frequent developmental assessments are important for which reason? a. Stable developmental periods during infancy provide an opportunity to identify any delays or deficits. b. Infants need stimulation specific to the stage of development. c. Critical periods of development occur during childhood. d. Child development is unpredictable and needs monitoring. Critical periods are blocks of time during which children are ready to master specific developmental tasks. The earlier that delays in development are discovered and intervention initiated, the less dramatic their effect will be. Infancy is a dynamic time of development that requires frequent evaluations to assess appropriate developmental progress. Infants in a nurturing environment will develop appropriately and will not necessarily need stimulation specific to their developmental stage. Normal growth and development are orderly and proceed in a predictable pattern on the basis of each individual’s abilities and potentials. PTS: 1 DIF: Cognitive Level: Comprehension REF: 757 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance 30. The theorist who viewed developmental progression as a lifelong series of conflicts that need resolution is: a. Erikson. c. Kohlberg. b. Freud. d. Piaget. Erik Erikson viewed development as a series of conflicts affected by social and cultural factors. Each conflict must be resolved for the child to progress emotionally, with unsuccessful resolution leaving the child emotionally disabled. Sigmund Freud proposed a psychosexual theory of development. He proposed that certain parts of the body assume psychological significance as foci of sexual energy. The foci shift as the individual moves through the different stages (oral, anal, phallic, latency, and genital) of development. Lawrence Kohlberg described moral development as having three levels (preconventional, conventional, and postconventional). His theory closely parallels Piaget’s. Jean Piaget’s cognitive theory interprets how children learn and think and how this thinking progresses and differs from adult thinking. Stages of his theory include sensorimotor, preoperations, concrete operations, and formal operations. PTS: 1 DIF: Cognitive Level: Comprehension REF: 757 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance 31. Which “expected outcome” would be developmentally appropriate for a hospitalized 4-year-old child? a. The child will be dressed and fed by the parents. b. The child will independently ask for play materials or other personal needs. c. The child will be able to verbalize an understanding of the reason for the hospitalization. d. The child will have a parent stay in the room at all times. Erikson identifies initiative as a developmental task for the preschool child. Initiating play activities and asking for play materials or assistance with personal needs demonstrate developmental appropriateness. Parents need to foster appropriate developmental behavior in the 4-year-old child. Dressing and feeding the child do not encourage independent behavior. A 4-year-old child cannot be expected to cognitively understand the reason for hospitalization. Expecting the child to verbalize an understanding for hospitalization is an inappropriate outcome. Parents staying with the child throughout a hospitalization is an inappropriate outcome. Although children benefit from parental involvement, parents may not have the support structure to stay in the room with the child at all times. PTS: 1 DIF: Cognitive Level: Application REF: 757 OBJ: Nursing Process: Planning MSC: Client Needs: Health Promotion and Maintenance MULTIPLE RESPONSE 32. Play serves many purposes. In teaching parents about appropriate activities, the nurse should inform them that play serves the following function (Select all that apply): a. Intellectual development b. Physical development c. Self-awareness d. Creativity e. Temperament development , C, D A common statement is that play is the work of childhood. Intellectual development is enhanced through the manipulation and exploration of objects. Self-awareness is the process of developing a self-identity. This process is facilitated through play. In addition, creativity is developed through the experimentation characteristic of imaginative play. Physical development depends on many factors; play is not one of them. Temperament refers to behavioral tendencies that are observable from the time of birth. The actual behaviors but not the child’s temperament attributes may be modified through play. PTS: 1 DIF: Cognitive Level: Comprehension REF: 763 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance 33. A nurse is preparing to administer a Denver II. Which statement(s) about the Denver II test is (are) accurate (Select all that apply)? a. All items intersected by the age line should be administered. b. There is no correction for a child born prematurely. c. The tool is an intelligence test. d. Toddlers and preschoolers should be prepared by presenting the test as a game. e. Presentation of the toys from the kit should be done one at a time. , D, E To identify “cautions,” all items intersected by the age line are administered. Toddlers and preschoolers should be tested by presenting the Denver II as a game. Because children are easily distracted, perform each item quickly and present only one toy from the kit at a time. Before beginning the screening, ask whether the child was born preterm and correctly calculate the adjusted age. Up to 24 months of age, allowances are made for preterm infants by subtracting the number of weeks of missed gestation from their present age and testing them at the adjusted age. Explain to the parents and child, if appropriate, that the screenings are not intelligence tests but rather are a method of showing what the child can do at a particular age. PTS: 1 DIF: Cognitive Level: Comprehension REF: 764 OBJ: Nursing Process: Implementation MSC: Client Needs: Health Promotion and Maintenance 34. What factors indicate that parents should seek genetic counseling for their child (Select all that apply)? a. Abnormal newborn screen b. Family history of a hereditary disease c. History of hypertension in the family d. Severe colic as an infant e. Metabolic disorder , B, E Factors indicating that parents should seek genetic counseling for their child include an abnormal newborn screen, family history of a hereditary disease, and a metabolic disorder. A history of hypertension or severe colic as an infant is not an indicator of a genetic disease. PTS: 1 DIF: Cognitive Level: Comprehension REF: 768 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance MATCHING Match the sequence of cephalocaudal development that the nurse expects to find in the normal infant with the appropriate step numbers. Begin with the first development expected, sequencing to the final. a. Crawl d. Gain complete head control b. Sit unsupported e. Walk c. Lift head when prone 35. Step 1 36. Step 2 37. Step 3 38. Step 4 39. Step 5 35. PTS: 1 DIF: Cognitive Level: Application REF: 751 OBJ: Nursing Process: Implementation MSC: Client Needs: Health Promotion and Maintenance NOT: Cephalocaudal development is from head to tail. Infants achieve structural control of the head before they have control of their trunks and extremities, they lift their head while prone, obtain complete head control, sit unsupported, crawl, and walk sequentially. 36. PTS: 1 DIF: Cognitive Level: Application REF: 751 OBJ: Nursing Process: Implementation MSC: Client Needs: Health Promotion and Maintenance NOT: Cephalocaudal development is from head to tail. Infants achieve structural control of the head before they have control of their trunks and extremities, they lift their head while prone, obtain complete head control, sit unsupported, crawl, and walk sequentially. 37. PTS: 1 DIF: Cognitive Level: Application REF: 751 OBJ: Nursing Process: Implementation MSC: Client Needs: Health Promotion and Maintenance NOT: Cephalocaudal development is from head to tail. Infants achieve structural control of the head before they have control of their trunks and extremities, they lift their head while prone, obtain complete head control, sit unsupported, crawl, and walk sequentially. 38. PTS: 1 DIF: Cognitive Level: Application REF: 751 OBJ: Nursing Process: Implementation MSC: Client Needs: Health Promotion and Maintenance NOT: Cephalocaudal development is from head to tail. Infants achieve structural control of the head before they have control of their trunks and extremities, they lift their head while prone, obtain complete head control, sit unsupported, crawl, and walk sequentially. 39. ANS: E PTS: 1 DIF: Cognitive Level: Application REF: 751 OBJ: Nursing Process: Implementation MSC: Client Needs: Health Promotion and Maintenance NOT: Cephalocaudal development is from head to tail. Infants achieve structural control of the head before they have control of their trunks and extremities, they lift their head while prone, obtain complete head control, sit unsupported, crawl, and walk sequentially. Chapter 26: 21st Century Pediatric Nursing MULTIPLE CHOICE 1. From a worldwide perspective, infant mortality in the United States: a. Is the highest of the other developed nations. b. Lags behind five other developed nations. c. Is the lowest infant death rate of developed nations. d. Lags behind most other developed nations. Although the death rate has decreased, the United States still ranks last among nations with the lowest infant death rates. The United States has the highest infant death rate of developed nations. PTS: 1 DIF: Cognitive Level: Knowledge REF: 723 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance 2. The major cause of death for children older than 1 year is: a. Cancer. c. Unintentional injuries. b. Infection. d. Congenital abnormalities. Unintentional injuries (accidents) are the leading cause of death after age 1 year through adolescence. Congenital anomalies are the leading cause of death in those younger than 1 year and are less significant in this age group. There have been major declines in deaths attributed infection as a result of improved therapies. Cancer is the second leading cause of death in this age group. PTS: 1 DIF: Cognitive Level: Comprehension REF: 723 OBJ: Nursing Process: Planning MSC: Client Needs: Health Promotion and Maintenance 3. In addition to injuries, the leading causes of death in adolescents ages 15 to 19 years are: a. Suicide, cancer. c. Homicide, heart disease. b. Homicide, suicide d. Drowning, cancer. In this age group the leading cause of death is accidents, followed by homicide and suicide. Other causes of death include cancer and heart disease. PTS: 1 DIF: Cognitive Level: Knowledge REF: 723 OBJ: Nursing Process: Planning MSC: Client Needs: Health Promotion and Maintenance 4. The leading cause of death from unintentional injuries in children is: a. Poisoning. c. Motor vehicle–related fatalities. b. Drowning. d. Fire- and burn-related fatalities. Motor vehicle–related fatalities comprise the leading cause of death in children, as either passengers or pedestrians. Poisoning is the ninth leading cause of death. Drowning is the second leading cause of death. Fire- and burn-related fatalities are the third leading cause of death. PTS: 1 DIF: Cognitive Level: Knowledge REF: 719 OBJ: Nursing Process: Planning MSC: Client Needs: Health Promotion and Maintenance 5. Which of the following is descriptive of deaths caused by unintentional injuries? a. More deaths occur in males. b. More deaths occur in females. c. The pattern of deaths varies widely in Western societies. d. The pattern of deaths does not vary according to age and sex. Most deaths from unintentional injuries occur in males. The pattern of death caused by unintentional injuries is consistent in Western societies. Causes of unintentional deaths vary with age and gender. PTS: 1 DIF: Cognitive Level: Comprehension REF: 720 OBJ: Nursing Process: Planning MSC: Client Needs: Health Promotion and Maintenance 6. The type of injury a child is especially susceptible to at a specific age is most closely related to: a. Physical health of the child. b. Developmental level of the child. c. Educational level of the child. d. Number of responsible adults in the home. The child’s developmental stage determines the type of injury that is likely to occur. The child’s physical health may facilitate his or her recovery from an injury. Educational level is related to developmental level, but it is not as important as the child’s developmental level in determining the type of injury. The number of responsible adults in the home may affect the number of unintentional injuries, but the type of injury is related to the child’s developmental stage. PTS: 1 DIF: Cognitive Level: Comprehension REF: 721 OBJ: Nursing Process: Planning MSC: Client Needs: Health Promotion and Maintenance 7. Which statement regarding childhood morbidity is the most accurate? a. Morbidity does not vary with age. b. Morbidity is not distributed randomly. c. Little can be done to improve morbidity. d. Unintentional injuries do not have an effect on morbidity. Morbidity is not distributed randomly in children. Increased morbidity is associated with certain groups of children, including children living in poverty and those who were low birth weight. Morbidity does vary with age. The types of illnesses in children are different for each age group. Morbidity can be decreased with interventions focused on groups with high morbidity and on decreasing unintentional injuries, which also affect morbidity. PTS: 1 DIF: Cognitive Level: Comprehension REF: 724 OBJ: Nursing Process: Planning MSC: Client Needs: Health Promotion and Maintenance 8. Which statement is most descriptive of pediatric family-centered care? a. It reduces the effect of cultural diversity on the family. b. It encourages family dependence on the health care system. c. It recognizes that the family is the constant in a child’s life. d. It avoids expecting families to be part of the decision-making process. The key components of family-centered care are for the nurse to support, respect, encourage, and embrace the family’s strength by developing a partnership with the child’s parents. Family-centered care recognizes the family as the constant in the child’s life. The nurse should support the cultural diversity of the family, not reduce its effect. The family should be enabled and empowered to work with the health care system and to be part of the decision-making process. PTS: 1 DIF: Cognitive Level: Comprehension REF: 725 OBJ: Nursing Process: Implementation MSC: Client Needs: Health Promotion and Maintenance 9. The nurse is preparing staff in-service education about atraumatic care for pediatric patients. Which intervention should the nurse include? a. Prepare the child for separation from parents during hospitalization by reviewing a video. b. Prepare the child before any unfamiliar treatment or procedure by demonstrating on a stuffed animal. c. Help the child accept the loss of control associated with hospitalization. d. Help the child accept pain that is connected with a treatment or procedure. Preparing the child for any unfamiliar treatments, controlling pain, allowing privacy, providing play activities for expression of fear and aggression, providing choices, and respecting cultural differences are components of atraumatic care. In providing atraumatic care, the separation of child from parents during hospitalization is minimized. The nurse should promote a sense of control for the child. Preventing and minimizing bodily injury and pain are major components of atraumatic care. PTS: 1 DIF: Cognitive Level: Application REF: 724 OBJ: Nursing Process: Implementation MSC: Client Needs: Health Promotion and Maintenance 10. Which statement best describes the process of critical thinking? a. It is a simple developmental process. b. It is purposeful and goal directed. c. It is based on deliberate and irrational thought. d. It assists individuals in guessing what is most appropriate. Critical thinking is a complex, developmental process based on rational and deliberate thought. When thinking is clear, precise, accurate, relevant, consistent, and fair, a logical connection develops between the elements of thought and the problem at hand. PTS: 1 DIF: Cognitive Level: Comprehension REF: 727 OBJ: Nursing Process: Planning MSC: Client Needs: Safe and Effective Care Environment 11. A clinic nurse is planning a teaching session about childhood obesity prevention for parents of school-age children. The nurse should include which associated risk of obesity in the teaching plan? a. Type I diabetes c. Celiac disease b. Respiratory disease d. Type II diabetes Childhood obesity has been associated with the rise of type II diabetes in children. Type I diabetes is not associated with obesity and has a genetic component. Respiratory disease is not associated with obesity, and celiac disease is the inability to metabolize gluten in foods and is not associated with obesity. PTS: 1 DIF: Cognitive Level: Application REF: 719 OBJ: Nursing Process: Planning MSC: Client Needs: Health Promotion and Maintenance 12. Which is now referred to as the “new morbidity”? a. Limitations in the major activities of daily living b. Unintentional injuries that cause chronic health problems c. Discoveries of new therapies to treat health problems d. Behavioral, social, and educational problems that alter health The new morbidity reflects the behavioral, social, and educational problems that interfere with the child’s social and academic development. It is also referred to a “‘pediatric social illness’.” Limitations in major activities of daily living and unintentional injuries that result in chronic health problems are included in morbidity data. Discovery of new therapies would be reflected in changes in morbidity data over time. PTS: 1 DIF: Cognitive Level: Knowledge REF: 719 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance 13. Which action by the nurse demonstrates use of evidence-based practice (EBP)? a. Gathering equipment for a procedure b. Documenting changes in a patient’s status c. Questioning the use of daily central line dressing changes d. Clarifying a physician’s prescription for morphine The nurse who questions the daily central line dressing change is ascertaining whether clinical interventions result in positive outcomes for patients. This demonstrates evidence-based practice (EBP), which implies questioning why something is effective and whether a better approach exists. Gathering equipment for a procedure and documenting changes in a patient’s status are practices that follow established guidelines. Clarifying a physician’s prescription for morphine constitutes safe nursing care. PTS: 1 DIF: Cognitive Level: Application REF: 727 OBJ: Nursing Process: Evaluation MSC: Client Needs: Safe and Effective Care Environment: Management of Care 14. A nurse is planning a class on accident prevention for parents of toddlers. Which safety topic is the priority for this class? a. Appropriate use of car seat restraints b. Safety crossing the street c. Helmet use when riding a bicycle d. Poison control numbers Motor vehicle accidents (MVAs) continue to be the most common cause of death in children older than 1 year; therefore, the priority topic is appropriate use of car seat restraints. Safety crossing the street and bicycle helmet use are topics that should be included for preschool parents but are not priorities for parents of toddlers. Information about poison control is important for parents of toddlers and would be a safety topic to include but is not the priority over the appropriate use of car seat restraints. PTS: 1 DIF: Cognitive Level: Application REF: 719 OBJ: Nursing Process: Planning MSC: Client Needs: Health Promotion and Maintenance MULTIPLE RESPONSE 15. The nursing process is a method of problem identification and problem solving that describes what the nurse actually does. The five steps include (Select all that apply): a. Assessment. b. Diagnosis. c. Planning. d. Documentation e. Implementation. f. Evaluation , B, C, E, F The accepted model is assessment, diagnosis, planning, implementation, and evaluation. The diagnosis phase is separated into two steps: nursing diagnosis and outcome identification. Although documentation is not one of the five steps of the nursing process, it is essential for evaluation. The nurse can assess, diagnose and identify problems, plan, and implement without documentation; however evaluation is best performed with written evidence of progress toward outcomes. PTS: 1 DIF: Cognitive Level: Knowledge REF: 728-729 OBJ: Nursing Process: Assessment, Diagnosis, Planning, Implementation, Evaluation MSC: Client Needs: Health Promotion and Maintenance 16. Which behaviors by the nurse indicate a therapeutic relationship with children and families? (Select all that apply.) a. Spending off-duty time with children and families b. Asking questions if families are not participating in the care c. Clarifying information for families d. Buying toys for a hospitalized child e. Learning about the family’s religious preferences , C, E Asking questions if families are not participating in the care, clarifying information for families, and learning about the family’s religious preferences are positive actions and foster therapeutic relationships with children and families. Spending off-duty time with children and families and buying toys for a hospitalized child are negative actions and indicate overinvolvement with children and families that is nontherapeutic. Chapter 31: The Infant and Family MULTIPLE CHOICE 1. Which statement best describes the infant’s physical development? a. Anterior fontanel closes by age 6 to 10 months. b. Binocularity is well established by age 8 months. c. Birth weight doubles by age 5 months and triples by age 1 year. d. Maternal iron stores persist during the first 12 months of life. Growth is very rapid during the first year of life. The birth weight approximately doubles by age 5 to 6 months and triples by age 1 year. The anterior fontanel closes at age 12 to 18 months. Binocularity is not established until age 15 months. Maternal iron stores are usually depleted by age 6 months. PTS: 1 DIF: Cognitive Level: Analysis REF: 866 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance 2. The nurse is assessing a 6-month-old healthy infant who weighed 7 pounds at birth. The nurse should expect the infant to now weigh approximately: a. 10 pounds. c. 20 pounds. b. 15 pounds. d. 25 pounds. Birth weight doubles at about age 5 to 6 months. At 6 months, an infant who weighed 7 pounds at birth would weigh approximately 15 pounds. Ten pounds is too little; the infant would have gone from the 50th percentile at birth to below the 5th percentile. Twenty pounds or more is too much; the infant would have tripled the birth weight at 6 months. PTS: 1 DIF: Cognitive Level: Analysis REF: 866 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance 3. The nurse is doing a routine assessment on a 14-month-old infant and notes that the anterior fontanel is closed. This should be interpreted as: a. A normal finding. b. A questionable finding—the infant should be rechecked in 1 month. c. An abnormal finding—indicates the need for immediate referral to a practitioner. d. An abnormal finding—indicates the need for developmental assessment. Because the anterior fontanel normally closes between ages 12 and 18 months, this is a normal finding, and no further intervention is required. PTS: 1 DIF: Cognitive Level: Analysis REF: 869 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance 4. By what age does the posterior fontanel usually close? a. 6 to 8 weeks c. 4 to 6 months b. 10 to 12 weeks d. 8 to 10 months The bones surrounding the posterior fontanel fuse and close by age 6 to 8 weeks. Ten weeks or longer is too late. PTS: 1 DIF: Cognitive Level: Knowledge REF: 864 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance 5. The parents of a 9-month-old infant tell the nurse that they have noticed foods such as peas and corn are not completely digested and can be seen in their infant’s stool. The nurse bases her explanation on knowing that: a. Children should not be given fibrous foods until the digestive tract matures at age 4 years. b. The infant should not be given any solid foods until this digestive problem is resolved. c. This is abnormal and requires further investigation. d. This is normal because of the immaturity of digestive processes at this age. The immaturity of the digestive tract is evident in the appearance of the stools. Solid foods are passed incompletely broken down in the feces. An excess quantity of fiber predisposes the child to large, bulky stools. This is a normal part of the maturational process, and no further investigation is necessary. PTS: 1 DIF: Cognitive Level: Application REF: 870 OBJ: Nursing Process: Implementation MSC: Client Needs: Health Promotion and Maintenance 6. A 3-month-old infant, born at 38 weeks of gestation, will hold a rattle if it is put in her hands; however, she will not voluntarily grasp it. The nurse should interpret this as: a. Normal development. b. Significant developmental lag. c. Slightly delayed development caused by prematurity. d. Suggestive of a neurologic disorder such as cerebral palsy. This indicates normal development. Reflexive grasping occurs during the first 2 to 3 months and then gradually becomes voluntary. No evidence of developmental lag, delayed development, or neurologic dysfunction is present. PTS: 1 DIF: Cognitive Level: Application REF: 871 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance 7. In terms of fine motor development, the infant of 7 months should be able to: a. Transfer objects from one hand to the other. b. Use thumb and index finger in a crude pincer grasp. c. Hold a crayon and make a mark on paper. d. Release cubes into a cup. By age 7 months, infants can transfer objects from one hand to the other, crossing the midline. The crude pincer grasp is apparent at about age 9 months. The infant can scribble spontaneously at age 15 months. At age 12 months, the infant can release cubes into a cup. PTS: 1 DIF: Cognitive Level: Comprehension REF: 871 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance 8. In terms of gross motor development, what would the nurse expect a 5-month-old infant to do? a. Roll from abdomen to back. c. Sit erect without support. b. Roll from back to abdomen. d. Move from prone to sitting position. Rolling from abdomen to back is developmentally appropriate for a 5-month-old infant. The ability to roll from back to abdomen usually occurs at 6 months old. Sitting erect without support is a developmental milestone usually achieved by 8 months. The 10-month-old infant can usually move from a prone to a sitting position. PTS: 1 DIF: Cognitive Level: Comprehension REF: 872 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance 9. At which age can most infants sit steadily unsupported? a. 4 months c. 8 months b. 6 months d. 10 months Sitting erect without support is a developmental milestone usually achieved by 8 months. At age 4 months, an infant can sit with support. At age 6 months, the infant will maintain a sitting position if propped. By 10 months, the infant can maneuver from a prone to a sitting position. PTS: 1 DIF: Cognitive Level: Comprehension REF: 872 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance 10. By what age should the nurse expect that an infant will be able to pull to a standing position? a. 6 months c. 9 months b. 8 months d. 11 to 12 months Most infants can pull themselves to a standing position at age 9 months. Any infant who cannot pull to a standing position by age 11 to 12 months should be referred for further evaluation for developmental dysplasia of the hip. At 6 months, the infant has just obtained coordination of arms and legs. By age 8 months, infants can bear full weight on their legs. PTS: 1 DIF: Cognitive Level: Comprehension REF: 872 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance 11. According to Piaget, the 6-month-old infant would be in what stage of the sensorimotor phase? a. Use of reflexes c. Secondary circular reactions b. Primary circular reactions d. Coordination of secondary schemata Infants are usually in the secondary circular reaction stage from age 4 months to 8 months. This stage is characterized by a continuation of the primary circular reaction for the response that results. For example, shaking of a rattle is performed to hear the noise of the rattle, not just for shaking. The use of reflexes is primarily during the first month of life. The primary circular reaction stage marks the replacement of reflexes with voluntary acts. The infant is in this stage from age 1 month to 4 months. The fourth sensorimotor stage is coordination of secondary schemata. This is a transitional stage in which increasing motor skills enable greater exploration of the environment. PTS: 1 DIF: Cognitive Level: Comprehension REF: 875 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance 12. Which behavior indicates that an infant has developed object permanence? a. Recognizes familiar face such as the mother b. Recognizes familiar object such as a bottle c. Actively searches for a hidden object d. Secures objects by pulling on a string During the first 6 months of life, infants believe that objects exist only as long as they can see them. When infants search for an object that is out of sight, this signals the attainment of object permanence, whereby an infant knows that an object exists even when it is not visible. Between ages 8 and 12 weeks, infants begin to respond differentially to their mothers. They cry, smile, vocalize, and show distinct preference for their mothers. This preference is one of the stages that influence the attachment process, but it is too early for object permanence. Recognizing familiar objects is an important transition for the infant, but it does not signal object permanence. The ability to understand cause and effect, such as pulling on a string to secure an object, is part of secondary schema development. PTS: 1 DIF: Cognitive Level: Analysis REF: 875 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance 13. A parent asks the nurse “At what age do most babies begin to fear strangers?” The nurse responds that most infants begin to fear strangers at age: a. 2 months. c. 6 months. b. 4 months. d. 12 months. Between ages 6 and 8 months, fear of strangers and stranger anxiety become prominent and are related to the infant’s ability to discriminate between familiar and nonfamiliar people. At age 2 months, the infant is just beginning to respond differentially to the mother. At age 4 months, the infant is beginning the process of separation individuation when the infant begins to recognize self and mother as separate beings. Twelve months is too late and requires referral for evaluation if the infant does not fear strangers at this age. PTS: 1 DIF: Cognitive Level: Comprehension REF: 877 OBJ: Nursing Process: Diagnosis MSC: Client Needs: Health Promotion and Maintenance 14. The nurse is interviewing the father of 10-month-old Megan. She is playing on the floor when she notices an electrical outlet and reaches up to touch it. Her father says “No” firmly and removes her from near the outlet. The nurse should use this opportunity to teach the father that Megan: a. Is old enough to understand the word “No.” b. Is too young to understand the word “No.” c. Should already know that electrical outlets are dangerous. d. Will learn safety issues better if she is spanked. By age 10 months, children are able to associate meaning with words. The child should be old enough to understand the word “No.” The 10-month-old is too young to understand the purpose of an electrical outlet. The father is using both verbal and physical cues to teach safety measures and alert the child to dangerous situations. Physical discipline should be avoided. PTS: 1 DIF: Cognitive Level: Analysis REF: 905 OBJ: Nursing Process: Implementation MSC: Client Needs: Health Promotion and Maintenance 15. Sara, age 4 months, was born at 35 weeks’ gestation. She seems to be developing normally, but her parents are concerned because she is a “more difficult” baby than their other child, who was term. The nurse should explain that: a. Infants’ temperaments are part of their unique characteristics. b. Infants become less difficult if they are not kept on scheduled feedings and structured routines. c. Sara’s behavior is suggestive of failure to bond completely with her parents. d. Sara’s difficult temperament is the result of painful experiences in the neonatal period. Infant temperament has a strong biologic component. Together with interactions with the environment, primarily the family, the biologic component contributes to the infant’s unique temperament. Children perceived as difficult may respond better to scheduled feedings and structured caregiving routines than to demand feedings and frequent changes in routines. Sara’s temperament has been created by both biologic and environmental factors. The nurse should provide guidance in parenting techniques that are best suited to Sara’s temperament. PTS: 1 DIF: Cognitive Level: Comprehension REF: 878 OBJ: Nursing Process: Implementation MSC: Client Needs: Health Promotion and Maintenance 16. Which information could be given to the parents of a 12-month-old child regarding appropriate play activities for this age? a. Give large push-pull toys for kinesthetic stimulation. b. Place cradle gym across crib to facilitate fine motor skills. c. Provide child with finger paints to enhance fine motor skills. d. Provide stick horse to develop gross motor coordination. The 12-month-old child is able to pull to a stand and walk holding on or independently. Appropriate toys for a child of this age include large push-pull toys for kinesthetic stimulation. A cradle gym should not be placed across the crib. Finger paints are appropriate for older children. A 12-month-old child does not have the stability to use a stick horse. PTS: 1 DIF: Cognitive Level: Analysis REF: 878 OBJ: Nursing Process: Planning MSC: Client Needs: Health Promotion and Maintenance 17. An appropriate play activity for a 7-month-old infant to encourage visual stimulation is: a. Playing peek-a-boo. c. Imitating animal sounds. b. Playing pat-a-cake. d. Showing how to clap hands. Because object permanence is a new achievement, peek-a-boo is an excellent activity to practice this new skill for visual stimulation. Playing pat-a-cake and showing how to clap hands will help with kinesthetic stimulation. Imitating animal sounds will help with auditory stimulation. PTS: 1 DIF: Cognitive Level: Analysis REF: 878 OBJ: Nursing Process: Planning MSC: Client Needs: Health Promotion and Maintenance 18. The best play activity to provide tactile stimulation for a 6-month-old infant is to: a. Allow to splash in bath. c. Play music box, tapes, or CDs. b. Give various colored blocks. d. Use infant swing or stroller. The feel of the water while the infant is splashing provides tactile stimulation. Various colored blocks provide visual stimulation for a 4- to 6-month-old infant. A music box, tapes, and CDs provide auditory stimulation. Swings and strollers provide kinesthetic stimulation. PTS: 1 DIF: Cognitive Level: Analysis REF: 875 OBJ: Nursing Process: Planning MSC: Client Needs: Health Promotion and Maintenance 19. At what age should the nurse expect an infant to begin smiling in response to pleasurable stimuli? a. 1 month c. 3 months b. 2 months d. 4 months At age 2 months, the infant has a social, responsive smile. A reflex smile is usually present at age 1 month. The 3-month-old can recognize familiar faces. At age 4 months, the infant can enjoy social interactions. PTS: 1 DIF: Cognitive Level: Comprehension REF: 876 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance 20. Latasha is a breastfed infant being seen in the clinic for her 6-month checkup. Her mother tells the nurse that Latasha recently began to suck her thumb. The best nursing intervention is to: a. Recommend that the mother substitute a pacifier for Latasha’s thumb. b. Assess Latasha for other signs of sensory deprivation. c. Reassure the mother that this is very normal at this age. d. Suggest that the mother breastfeed Latasha more often to satisfy sucking needs. Sucking is an infant’s chief pleasure, and she may not be satisfied by bottle-feeding or breastfeeding alone. During infancy and early childhood, there is no need to restrict nonnutritive sucking. Dental damage does not appear to occur unless the use of the pacifier or finger persists after age 4 to 6 years. The nurse should explore with the mother her feelings about pacifier vs. thumb. This is a normal behavior to meet nonnutritive sucking needs. No data support that Latasha has sensory deprivation. PTS: 1 DIF: Cognitive Level: Application REF: 880 OBJ: Nursing Process: Implementation MSC: Client Needs: Health Promotion and Maintenance 21. Austin, age 6 months, has six teeth. The nurse should recognize that this is: a. Normal tooth eruption. c. Unusual and dangerous. b. Delayed tooth eruption. d. Earlier-than-normal tooth eruption. This is earlier than expected. Most infants at age 6 months have two teeth. Six teeth at 6 months is not delayed; it is early tooth eruption. Although unusual, it is not dangerous. PTS: 1 DIF: Cognitive Level: Comprehension REF: 881 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance 22. The nurse notices that a 10-month-old infant being seen in the clinic is wearing expensive, inflexible, high-top shoes. The nurse should explain that: a. Soft and flexible shoes are generally better. b. High-top shoes are necessary for support. c. Inflexible shoes are necessary to prevent in-toeing and out-toeing. d. This type of shoe will encourage the infant to walk sooner. The main purpose of the shoe is protection. Soft, well-constructed, athletic-type shoes are best for infants and children. High-top shoes are not necessary for support but may be helpful keeping the child’s foot in the shoe. Inflexible shoes can delay walking, aggravate in-toeing and out-toeing, and impede development of the supportive foot muscles. PTS: 1 DIF: Cognitive Level: Analysis REF: 901 OBJ: Nursing Process: Implementation MSC: Client Needs: Health Promotion and Maintenance 23. A mother tells the nurse that she is discontinuing breastfeeding her 5-month-old infant. The nurse should recommend that the infant be given: a. Skim milk. c. Commercial iron-fortified formula. b. Whole cow’s milk. d. Commercial formula without iron. For children younger than 1 year, the American Academy of Pediatrics recommends the use of breast milk. If breastfeeding has been discontinued, iron-fortified commercial formula should be used. Cow’s milk should not be used in children younger than 12 months. Maternal iron stores are almost depleted by this age; the iron-fortified formula will help prevent the development of iron deficiency anemia. PTS: 1 DIF: Cognitive Level: Comprehension REF: 882 OBJ: Nursing Process: Implementation MSC: Client Needs: Health Promotion and Maintenance 24. When is the best age for solid food to be introduced into the infant’s diet? a. 2 to 3 months c. When birth weight has tripled b. 4 to 6 months d. When tooth eruption has started Physiologically and developmentally, the 4- to 6-month-old is in a transition period. The extrusion reflex has disappeared, and swallowing is a more coordinated process. In addition, the gastrointestinal tract has matured sufficiently to handle more complex nutrients and is less sensitive to potentially allergenic food. Infants of this age will try to help during feeding. Two to 3 months is too young. The extrusion reflex is strong, and the infant will push food out with the tongue. No research base indicates that the addition of solid food to bottle-feeding has any benefit. Tooth eruption can facilitate biting and chewing; most infant foods do not require this ability. PTS: 1 DIF: Cognitive Level: Comprehension REF: 882 OBJ: Nursing Process: Planning MSC: Client Needs: Health Promotion and Maintenance 25. The parents of a 4-month-old infant tell the nurse that they are getting a microwave oven and will be able to heat the baby’s formula faster. The nurse should recommend: a. Never heating a bottle in a microwave oven. b. Heating only 10 ounces or more. c. Always leaving the bottle top uncovered to allow heat to escape. d. Shaking the bottle vigorously for at least 30 seconds after heating. Neither infant formula nor breast milk should be warmed in a microwave oven as this may cause oral burns as a result of uneven heating in the container. The bottle may remain cool while hot spots develop in the milk. Warming expressed milk in a microwave decreases the availability of antiinfective properties and causes separation of the fat content. Milk should be warmed in a lukewarm water bath. PTS: 1 DIF: Cognitive Level: Analysis REF: 883 OBJ: Nursing Process: Implementation MSC: Client Needs: Health Promotion and Maintenance 26. Parents tell the nurse that their 1-year-old son often sleeps with them. They seem unconcerned about this. The nurse’s response should be based on the knowledge that: a. Children should not sleep with their parents. b. Separation from parents should be completed by this age. c. Daytime attention should be increased. d. This is a common and accepted practice, especially in some cultural groups. Co-sleeping or sharing the family bed, in which the parents allow the children to sleep with them, is a common and accepted practice in many cultures. Parents should evaluate the options available and avoid conditions that place the infant at risk. Population-based studies are currently underway; no evidence at this time supports or abandons the practice for safety reasons. This is the age at which children are just beginning to individuate. Increased daytime activity may help decrease sleep problems in general, but co-sleeping is a culturally determined phenomenon. PTS: 1 DIF: Cognitive Level: Comprehension REF: 911 OBJ: Nursing Process: Planning MSC: Client Needs: Health Promotion and Maintenance 27. The parent of 2-week-old Sarah asks the nurse if Sarah needs fluoride supplements because she is exclusively breastfed. The nurse’s best response is: a. “She needs to begin taking them now.” b. “They are not needed if you drink fluoridated water.” c. “She may need to begin taking them at age 6 months.” d. “She can have infant cereal mixed with fluoridated water instead of supplements.” Fluoride supplementation is recommended by the American Academy of Pediatrics beginning at age 6 months if the child is not drinking adequate amounts of fluoridated water. The recommendation is to begin supplementation at 6 months, not at 2 weeks. The amount of water that is ingested and the amount of fluoride in the water are evaluated when supplementation is being considered. PTS: 1 DIF: Cognitive Level: Comprehension REF: 883 OBJ: Nursing Process: Planning MSC: Client Needs: Health Promotion and Maintenance 28. A mother tells the nurse that she doesn’t want her infant immunized because of the discomfort associated with injections. The nurse should explain that: a. This cannot be prevented. b. Infants do not feel pain as adults do. c. This is not a good reason for refusing immunizations. d. A topical anesthetic, eutectic mixture of local anesthetic (EMLA), can be applied before injections are given. Several topical anesthetic agents can be used to minimize the discomfort associated with immunization injections. These include EMLA and vapor coolant sprays. Pain associated with many procedures can be prevented or minimized by using the principles of atraumatic care. With preparation, the injection site can be properly anesthetized to decrease the amount of pain felt by the infant. Infants have the neural pathways to sense pain. Numerous research studies have indicated that infants perceive and react to pain in the same manner as do children and adults. The mother should be allowed to discuss her concerns and the alternatives available. This is part of the informed consent process. PTS: 1 DIF: Cognitive Level: Analysis REF: 895 OBJ: Nursing Process: Implementation MSC: Client Needs: Health Promotion and Maintenance 29. The parents of a 12-month-old child ask the nurse if the child can eat hot dogs. The nurse’s reply should be based on knowing that: a. The child is too young to digest hot dogs. b. The child is too young to eat hot dogs safely. c. Hot dogs must be sliced into sections to prevent aspiration. d. Hot dogs must be cut into small, irregular pieces to prevent aspiration. Hot dogs are of a consistency, diameter, and round shape that may cause complete obstruction of the child’s airway. If given to young children, the hot dog should be cut into small irregular pieces rather than served whole or in slices. The child’s digestive system is mature enough to digest hot dogs. To eat the hot dog safely, the child should be sitting down, and the hot dog should be appropriately cut into irregularly shaped pieces. PTS: 1 DIF: Cognitive Level: Comprehension REF: 900 OBJ: Nursing Process: Implementation MSC: Client Needs: Health Promotion and Maintenance 30. The clinic is lending a federally approved car seat to an infant’s family. The nurse should explain that the safest place to put the car seat is: a. Front facing in back seat. b. Rear facing in back seat. c. Front facing in front seat if an air bag is on the passenger side. d. Rear facing in front seat if an air bag is on the passenger side. The rear-facing car seat provides the best protection for an infant’s disproportionately heavy head and weak neck. Infants should face the rear from birth to 20 pounds and as close to 1 year of age as possible. The middle of the back seat provides the safest position. Severe injuries and deaths in children have occurred from air bags deploying on impact in the front passenger seat. PTS: 1 DIF: Cognitive Level: Comprehension REF: 900 OBJ: Nursing Process: Planning MSC: Client Needs: Health Promotion and Maintenance 31. A nurse is teaching parents about prevention and treatment of colic. Which should the nurse include in the teaching plan? a. Avoid use of pacifiers. b. Eliminate all secondhand smoke contact. c. Lay infant flat after feeding. d. Avoid swaddling the infant. To prevent and treat colic, teach parents that if household members smoke, they should avoid smoking near the infant; smoking activity should preferably be confined to outside of the home. A pacifier can be introduced for added sucking. The infant should be swaddled tightly with a soft, stretchy blanket and placed in an upright seat after feedings. PTS: 1 DIF: Cognitive Level: Application REF: 905 OBJ: Nursing Process: Implementation MSC: Client Needs: Physiologic Integrity 32. A parent of an infant with colic tells the nurse, “All this baby does is scream at me; it is a constant worry.” The nurse’s best action is: a. Encourage parent to verbalize feelings. b. Encourage parent not to worry so much. c. Assess parent for other signs of inadequate parenting. d. Reassure parent that colic rarely lasts past age 9 months. Colic is multifactorial, and no single treatment is effective for all infants. The parent is verbalizing concern and worry. The nurse should allow the parent to put these feelings into words. An empathic, gentle, and reassuring attitude, in addition to suggestions about remedies, will help alleviate the parent’s anxieties. The nurse should reassure the parent that he or she is not doing anything wrong. The infant with colic is experiencing spasmodic pain that is manifested by loud crying, in some cases up to 3 hours each day. Telling the parent that it will eventually go away does not help him or her through the current situation. PTS: 1 DIF: Cognitive Level: Application REF: 906 OBJ: Nursing Process: Implementation MSC: Client Needs: Psychosocial Integrity 33. Parent guidelines for relieving colic in an infant include: a. Avoiding touching the abdomen. b. Avoiding using a pacifier. c. Changing the infant’s position frequently. d. Placing the infant where the family cannot hear the crying. Changing the infant’s position frequently may be beneficial. The parent can walk holding the infant face down and with the infant’s chest across the parent’s arm. The parent’s hand can support the infant’s abdomen, applying gentle pressure. Gently massaging the abdomen is effective in some infants. Pacifiers can be used for meeting additional sucking needs. The infant should not be placed where monitoring cannot be done. The infant can be placed in the crib and allowed to cry. Periodically, the infant should be picked up and comforted. PTS: 1 DIF: Cognitive Level: Application REF: 907 OBJ: Nursing Process: Implementation MSC: Client Needs: Physiologic Integrity 34. Clinical manifestations of failure to thrive caused by behavioral problems resulting in inadequate intake of calories include: a. Avoidance of eye contact. b. An associated malabsorption defect. c. Weight that falls below the 15th percentile. d. Normal achievement of developmental landmarks. One of the clinical manifestations of nonorganic failure to thrive is the child’s avoidance of eye contact with the health professional. A malabsorption defect would result in a physiologic problem, not behavioral. Weight (but not height) below the 5th percentile is indicative of failure to thrive. Developmental delays, including social, motor, adaptive, and language, exist. PTS: 1 DIF: Cognitive Level: Comprehension REF: 909 OBJ: Nursing Process: Assessment MSC: Client Needs: Physiologic Integrity 35. Which is an important nursing consideration when caring for an infant with failure to thrive? a. Establish a structured routine and follow it consistently. b. Maintain a nondistracting environment by not speaking to the infant during feeding. c. Place the infant in an infant seat during feedings to prevent overstimulation. d. Limit sensory stimulation and play activities to alleviate fatigue. The infant with failure to thrive should have a structured routine that is followed consistently. Disruptions in other activities of daily living can have a great impact on feeding behaviors. Bathing, sleeping, dressing, playing, and feeding are structured. The nurse should talk to the infant by giving directions about eating. This will help the infant maintain focus. Young children should be held while being fed, and older children can sit at a feeding table. The infant should be fed in the same manner at each meal. The infant can engage in sensory and play activities at times other than mealtime. PTS: 1 DIF: Cognitive Level: Application REF: 910 OBJ: Nursing Process: Implementation MSC: Client Needs: Physiologic Integrity 36. An important nursing responsibility when dealing with a family experiencing the loss of an infant from sudden infant death syndrome (SIDS) is to: a. Explain how SIDS could have been predicted and prevented. b. Interview parents in depth concerning the circumstances surrounding the infant’s death. c. Discourage parents from making a last visit with the infant. d. Make a follow-up home visit to parents as soon as possible after the infant’s death. A competent, qualified professional should visit the family at home as soon as possible after the death and provide the family with printed information about SIDS. An explanation of how SIDS could have been predicted and prevented is inappropriate. SIDS cannot be prevented or predicted. Discussions about the cause will only increase parental guilt. The parents should be asked only factual questions to determine the cause of death. Parents should be allowed and encouraged to make a last visit with their infant. PTS: 1 DIF: Cognitive Level: Application REF: 910 OBJ: Nursing Process: Implementation MSC: Client Needs: Psychosocial Integrity 37. Which is the most appropriate action when an infant becomes apneic? a. Shake vigorously. b. Roll head side to side. c. Hold by feet upside down with head supported. d. Gently stimulate trunk by patting or rubbing. If the infant is apneic, the infant’s trunk should be gently stimulated by patting or rubbing. If the infant is prone, turn onto the back. The infant should not be shaken vigorously, have the head rolled side to side, or be held by the feet upside down with the head supported. These actions can cause injury. PTS: 1 DIF: Cognitive Level: Application REF: 916 OBJ: Nursing Process: Implementation MSC: Client Needs: Physiologic Integrity 38. With the goal of preventing plagiocephaly, the nurse should teach new parents to: a. Place the infant prone for 30 to 60 minutes per day. b. Buy a soft mattress. c. Allow the infant to nap in the car safety seat. d. Have the infant sleep with the parents. Prevention of positional plagiocephaly may begin shortly after birth by implementing prone positioning or “tummy time” for approximately 30 to 60 minutes per day when the infant is awake. Soft mattresses or sleeping with parents (co-sleeping) are not recommended because they put the infant at a higher risk for a sudden infant death incident. To prevent plagiocephaly, prolonged placement in car safety seats should be avoided. PTS: 1 DIF: Cognitive Level: Application REF: 912 OBJ: Nursing Process: Implementation MSC: Client Needs: Physiologic Integrity 39. An infant has been pronounced dead from sudden infant death syndrome (SIDS) in the emergency department. Which is an appropriate question to ask the parents? a. “Did you hear the infant cry out?” b. “Why didn’t you check on the infant earlier?” c. “What time did you find the infant?” d. “Was the head buried in a blanket?” During a SIDS incident, if the infant is not pronounced dead at the scene, he or she may be transported to the emergency department to be pronounced dead by a physician. While they are in the emergency department, the parents are asked only factual questions, such as when they found the infant, how he or she looked, and whom they called for help. The nurse avoids any remarks that may suggest responsibility, such as “Why didn’t you go in earlier?” “Didn’t you hear the infant cry out?” or “Was the head buried in a blanket?” PTS: 1 DIF: Cognitive Level: Application REF: 912 OBJ: Nursing Process: Implementation MSC: Client Needs: Psychosocial Integrity 40. An infant experienced an apparent life-threatening event and is being placed on home apnea monitoring. The parents have understood the instructions for use of a home apnea monitor when they state: a. “We can adjust the monitor to eliminate false alarms.” b. “We should sleep in the same bed as our monitored infant.” c. “We will check the monitor several times a day to be sure the alarm is working.” d. “We will place the monitor in the crib with our infant.” The parents should check the monitor several times a day to be sure the alarm is working and that it can be heard from room to room. The parents should not adjust the monitor to eliminate false alarms. Adjustments could compromise the monitor’s effectiveness. The monitor should be placed on a firm surface away from the crib and drapes. The parents should not sleep in the same bed as the monitored infant. PTS: 1 DIF: Cognitive Level: Application REF: 912 OBJ: Nursing Process: Implementation MSC: Client Needs: Physiologic Integrity 41. The parents of a 3-month-old infant report that their infant sleeps supine (face up) but is often prone (face down) while awake. The nurse’s response should be based on knowledge that this is: a. Unacceptable because of the risk of sudden infant death syndrome (SIDS). b. Unacceptable because it does not encourage achievement of developmental milestones. c. Unacceptable to encourage fine motor development. d. Acceptable to encourage head control and turning over. These parents are implementing the guidelines to reduce the risk of SIDS. Infants should sleep on their backs and then be placed on their abdomens when awake to enhance development of milestones such as head control. The face-down position while awake and positioning on the back for sleep are acceptable because they reduce risk of SIDS and allow achievement of developmental milestones. These position changes encourage gross motor, not fine motor, development. PTS: 1 DIF: Cognitive Level: Analysis REF: 871 OBJ: Nursing Process: Implementation MSC: Client Needs: Health Promotion and Maintenance 42. The nurse should teach parents that which age is safe to give infants whole milk instead of commercial infant formula? a. 6 months c. 12 months b. 9 months d. 18 months The American Academy of Pediatrics does not recommend the use of cow’s milk for children younger than 12 months. At 6 and 9 months, the infant should be receiving commercial infant formula or breast milk. At age 18 months, milk and formula are supplemented with solid foods, water, and some fruit juices. PTS: 1 DIF: Cognitive Level: Comprehension REF: 883 OBJ: Nursing Process: Implementation MSC: Client Needs: Health Promotion and Maintenance 43. A parent asks the nurse whether her infant is susceptible to pertussis. The nurse’s response should be based on which statement concerning susceptibility to pertussis? a. Neonates will be immune the first few months. b. If the mother has had the disease, the infant will receive passive immunity. c. Children younger than 1 year seldom contract this disease. d. Most children are highly susceptible from birth. The acellular pertussis vaccine is recommended by the American Academy of Pediatrics beginning at age 6 weeks. Infants are at greater risk for complications of pertussis. The vaccine is not given after age 7 years, when the risks of the vaccine become greater than those of pertussis. The infant is highly susceptible to pertussis, which can be a life-threatening illness in this age-group. PTS: 1 DIF: Cognitive Level: Application REF: 890 OBJ: Nursing Process: Implementation MSC: Client Needs: Health Promotion and Maintenance MULTIPLE RESPONSE 44. Pacifiers can be extremely dangerous because of the frequency of use and the intensity of the infant’s suck. In teaching parents about appropriate pacifier selection, the nurse should explain that a pacifier should have which characteristics (select all that apply)? a. Easily grasped handle b. One-piece construction c. Ribbon or string to secure to clothing d. Soft, pliable material e. Sturdy, flexible material , B, E A good pacifier should be easily grasped by the infant. One-piece construction is necessary to avoid having the nipple and guard separate. The material should be sturdy and flexible. An attached ribbon or string and soft, pliable material are not characteristics of a good pacifier. PTS: 1 DIF: Cognitive Level: Comprehension REF: 900 OBJ: Nursing Process: Planning MSC: Client Needs: Safe and Effective Care Environment 45. In terms of gross motor development, what would the nurse expect a 5-month-old infant to do (select all that apply)? a. Roll from abdomen to back. b. Put feet in mouth when supine. c. Roll from back to abdomen. d. Sit erect without support. e. Move from prone to sitting position. , B Rolling from abdomen to back and placing the feet in the mouth when supine are developmentally appropriate for a 5-month-old infant. Rolling from back to abdomen is developmentally appropriate for a 6-month-old infant. An 8-month-old infant should be able to sit erect without support. A 10-month-old infant can usually move from a prone to a sitting position. PTS: 1 DIF: Cognitive Level: Application REF: 872 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance 46. A nurse is conducting education classes for parents of infants. The nurse plans to discuss sudden infant death syndrome (SIDS). Which risk factors should the nurse include as increasing an infant’s risk of a SIDS incident(select all that apply)? a. Breastfeeding b. Low Apgar scores c. Male sex d. Birth weight in the 50th or higher percentile e. Recent viral illness , C, E Certain groups of infants are at increased risk for SIDS: those with low birth weight, low Apgar scores, or recent viral illness, and those of male sex. Breastfed infants and infants of average or above-average weight are not at higher risk for SIDS. PTS: 1 DIF: Cognitive Level: Comprehension REF: 911 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance 47. Which interventions should the nurse implement when caring for a family of a sudden infant death syndrome (SIDS) infant (select all that apply)? a. Allow parents to say goodbye to their infant. b. Once parents leave the hospital, no further follow-up is required. c. Arrange for someone to take the parents home from the hospital. d. Avoid requesting an autopsy of the deceased infant. e. Conduct a debriefing session with the parents before they leave the hospital. , C, E An important aspect of compassionate care for parents experiencing a SIDS incident is allowing them to say good-bye to their infant. These are the parents’ last moments with their infant, and they should be as quiet, meaningful, peaceful, and undisturbed as possible. Because the parents leave the hospital without their infant, it is helpful to accompany them to the car or arrange for someone else to take them home. A debriefing session may help health care workers who dealt with the family and deceased infant to cope with emotions that are often engendered when a SIDS victim is brought into the acute care facility. An autopsy may clear up possible misconceptions regarding the death. When the parents return home, a competent, qualified professional should visit them after the death as soon as possible. PTS: 1 DIF: Cognitive Level: Comprehension REF: 913 OBJ: Nursing Process: Implementation MSC: Client Needs: Psychosocial Integrity 48. A nurse is preparing to administer routine immunizations to a 4-month-old infant. The infant is currently up to date on all previously recommended immunizations. Which immunizations will the nurse prepare to administer (select all that apply)? a. Measles, mumps, and rubella (MMR) b. Rotavirus (RV) c. Diphtheria, tetanus, and acellular pertussis (DTaP) d. Varicella e. Haemophilus influenzae type b (HIB) f. Inactivated poliovirus (IPV) , C, E, F The recommended immunization schedule for a 4-month-old, up to date on immunizations, would be to administer the RV, DTaP, HIB, and IPV vaccinations. The MMR and varicella vaccinations would not be administered until the child is at least 1 year of age. PTS: 1 DIF: Cognitive Level: Application REF: 886 OBJ: Nursing Process: Implementation MSC: Client Needs: Health Promotion and Maintenance 49. A nurse has completed a teaching session for parents about “baby-proofing” the home. Which statements made by the parents indicate an understanding of the teaching (select all that apply)? a. “We will put plastic fillers in all electrical plugs.” b. “We will place poisonous substances in a high cupboard.” c. “We will place a gate at the top and bottom of stairways.” d. “We will keep our household hot water heater at 130 degrees.” e. “We will remove front knobs from the stove.” , C, E By the time babies reach 6 months of age, they begin to become much more active, curious, and mobile. Putting plastic fillers on all electrical plugs can prevent an electrical shock. Putting gates at the top and bottom of stairways will prevent falls. Removing front knobs from the stove can prevent burns. Poisonous substances should be stored in a locked cabinet, not in a cabinet that children can reach when they begin to climb. The household hot water heater should be turned down to 120 degrees or less. PTS: 1 DIF: Cognitive Level: Analysis REF: 905 OBJ: Nursing Process: Evaluation MSC: Client Needs: Health Promotion and Maintenance MATCHING Place in order the expected sequence of fine motor developmental milestones for an infant, beginning with the first milestone achieved and ending with the last milestone achieved. a. Voluntary palmar grasp d. Neat pincer grasp b. Reflex palmar grasp e. Builds a tower of two blocks c. Puts objects into a container 50. First 51. Second 52. Third 53. Fourth 54. Fifth 50. PTS: 1 DIF: Cognitive Level: Analysis REF: 868 OBJ: Nursing Process: Evaluation MSC: Client Needs: Health Promotion and Maintenance NOT: Grasping occurs during the first 2 to 3 months as a reflex and gradually becomes voluntary. By 5 months, infants are able to voluntarily grasp objects. Gradually, the palmar grasp (using the whole hand) is replaced by a pincer grasp (using the thumb and index finger). By 8 to 10 months of age, infants use a crude pincer grasp, and by 11 months, they have progressed to a neat pincer grasp. By 11 months, they put objects into containers and like to remove them. By age 1 year, infants try to build towers of two blocks. 51. PTS: 1 DIF: Cognitive Level: Analysis REF: 868 OBJ: Nursing Process: Evaluation MSC: Client Needs: Health Promotion and Maintenance NOT: Grasping occurs during the first 2 to 3 months as a reflex and gradually becomes voluntary. By 5 months, infants are able to voluntarily grasp objects. Gradually, the palmar grasp (using the whole hand) is replaced by a pincer grasp (using the thumb and index finger). By 8 to 10 months of age, infants use a crude pincer grasp, and by 11 months, they have progressed to a neat pincer grasp. By 11 months, they put objects into containers and like to remove them. By age 1 year, infants try to build towers of two blocks. 52. PTS: 1 DIF: Cognitive Level: Analysis REF: 868 OBJ: Nursing Process: Evaluation MSC: Client Needs: Health Promotion and Maintenance NOT: Grasping occurs during the first 2 to 3 months as a reflex and gradually becomes voluntary. By 5 months, infants are able to voluntarily grasp objects. Gradually, the palmar grasp (using the whole hand) is replaced by a pincer grasp (using the thumb and index finger). By 8 to 10 months of age, infants use a crude pincer grasp, and by 11 months, they have progressed to a neat pincer grasp. By 11 months, they put objects into containers and like to remove them. By age 1 year, infants try to build towers of two blocks. 53. PTS: 1 DIF: Cognitive Level: Analysis REF: 868 OBJ: Nursing Process: Evaluation MSC: Client Needs: Health Promotion and Maintenance NOT: Grasping occurs during the first 2 to 3 months as a reflex and gradually becomes voluntary. By 5 months, infants are able to voluntarily grasp objects. Gradually, the palmar grasp (using the whole hand) is replaced by a pincer grasp (using the thumb and index finger). By 8 to 10 months of age, infants use a crude pincer grasp, and by 11 months, they have progressed to a neat pincer grasp. By 11 months, they put objects into containers and like to remove them. By age 1 year, infants try to build towers of two blocks. 54. ANS: E PTS: 1 DIF: Cognitive Level: Analysis REF: 868 OBJ: Nursing Process: Evaluation MSC: Client Needs: Health Promotion and Maintenance NOT: Grasping occurs during the first 2 to 3 months as a reflex and gradually becomes voluntary. By 5 months, infants are able to voluntarily grasp objects. Gradually, the palmar grasp (using the whole hand) is replaced by a pincer grasp (using the thumb and index finger). By 8 to 10 months of age, infants use a crude pincer grasp, and by 11 months, they have progressed to a neat pincer grasp. By 11 months, they put objects into containers and like to remove them. By age 1 year, infants try to build towers of two blocks. Chapter 32: The Toddler and Family MULTIPLE CHOICE 1. Which factor is most important in predisposing toddlers to frequent infections such as otitis media, tonsillitis, and upper respiratory tract infections? a. Respirations are abdominal. b. Pulse and respiratory rates are slower than those in infancy. c. Defense mechanisms are less efficient than those during infancy. d. Short, straight internal ear/throat structures and large tonsil/adenoid lymph tissue are present. Toddlers continue to have the short, straight internal ear canal of infants. The lymphoid tissue of the tonsils and adenoids continues to be relatively large. These two anatomic conditions combine to predispose the toddler to frequent infections. The abdominal respirations and lowered pulse and respiratory rate of toddlers do not affect their susceptibility to infection. The defense mechanisms are more efficient compared with those of infancy. PTS: 1 DIF: Cognitive Level: Analysis REF: 923 OBJ: Nursing Process: Assessment MSC: Client Needs: Physiologic Integrity 2. The psychosocial developmental tasks of toddlerhood include: a. Development of a conscience. b. Recognition of sex differences. c. Ability to get along with age mates. d. Ability to withstand delayed gratification. If the need for basic trust has been satisfied, toddlers can give up dependence for control, independence, and autonomy. One of the tasks that the toddler is concerned with is the ability to withstand delayed gratification. Development of a conscience occurs during the preschool years. The recognition of sex differences occurs during the preschool years. The ability to get along with age mates develops during the preschool and school-age years. PTS: 1 DIF: Cognitive Level: Comprehension REF: 924 OBJ: Nursing Process: Assessment MSC: Client Needs: Psychosocial Integrity 3. A parent of an 18-month-old boy tells the nurse that he says “no” to everything and has rapid mood swings. If he is scolded, he shows anger and then immediately wants to be held. The nurse’s best interpretation of this behavior is that: a. This is normal behavior for his age. b. This is unusual behavior for his age. c. He is not effectively coping with stress. d. He is showing he needs more attention. Toddlers use distinct behaviors in the quest for autonomy. They express their will with continued negativity and the use of the word “no.” Children at this age also have rapid mood swings. The nurse should reassure the parents that their child is engaged in expected behavior for an 18-month-old. PTS: 1 DIF: Cognitive Level: Comprehension REF: 933 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance 4. The nurse is planning care for a 17-month-old child. According to Piaget, in what stage would the nurse expect the child to be? a. Trust c. Secondary circular reaction b. Preoperations d. Tertiary circular reaction The 17-month-old is in the fifth stage of the sensorimotor phase: tertiary circular reactions. The child uses active experimentation to achieve previously unattainable goals. Trust is Erikson’s first stage. Preoperations is the stage of cognitive development, usually present in older toddlers and preschoolers. Secondary circular reactions last from about ages 4 to 8 months. PTS: 1 DIF: Cognitive Level: Comprehension REF: 924 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance 5. What describes a toddler’s cognitive development at age 20 months? a. Searches for an object only if he or she sees it being hidden b. Realizes that “out of sight” is not out of reach c. Puts objects into a container but cannot take them out d. Understands the passage of time such as “just a minute” and “in an hour” At this age the child is in the final sensorimotor stage. Children will now search for an object in several potential places, even though they saw only the original hiding place. Children have a more developed sense of objective permanence. They will search for objects even if they have not seen them hidden. Putting an object in a container but being unable to take it out indicates tertiary circular reactions. An embryonic sense of time exists; although toddlers may behave appropriately to time-oriented phrases, their sense of timing is exaggerated. PTS: 1 DIF: Cognitive Level: Comprehension REF: 924 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance 6. Although a 14-month-old girl received a shock from an electrical outlet recently, her parents find her about to place a paper clip in another outlet. The best interpretation of this behavior is that: a. Her cognitive development is delayed. b. This is typical behavior because toddlers are not very developed. c. This is typical behavior because of inability to transfer knowledge to new situations. d. This is not typical behavior because toddlers should know better than to repeat an act that caused pain. During the tertiary circular reactions stage, children have only a rudimentary sense of the classification of objects. The appearance of an object denotes its function for these children. The slot of an outlet is for putting things into. Her cognitive development is appropriate for her age and represents typical behavior for a toddler. Only some awareness exists of a causal relation between events. PTS: 1 DIF: Cognitive Level: Comprehension REF: 924 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance 7. Two toddlers are playing in a sandbox when one child suddenly grabs a toy from the other child. The best interpretation of this behavior is that: a. This is typical behavior because toddlers are aggressive. b. This is typical behavior because toddlers are egocentric. c. Toddlers should know that sharing toys is expected of them. d. Toddlers should have the cognitive ability to know right from wrong. Play develops from the solitary play of infancy to the parallel play of toddlers. The toddler plays alongside other children, not with them. This typical behavior of the toddler is not intentionally aggressive. Shared play is not within their cognitive development. Toddlers do not conceptualize shared play. Because the toddler cannot view the situation from the perspective of the other child, it is okay to take the toy. Therefore, no right or wrong is associated with taking a toy. PTS: 1 DIF: Cognitive Level: Comprehension REF: 928 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance 8. Which statement about toilet training is correct? a. Bladder training is usually accomplished before bowel training. b. Wanting to please the parent helps motivate the child to use the toilet. c. Watching older siblings use the toilet confuses the child. d. Children must be forced to sit on the toilet when first learning. Voluntary control of the anal and urethral sphincters is achieved sometime after the child is walking. The child must be able to recognize the urge to let go and to hold on. The child must want to please the parent by holding on rather than pleasing self by letting go. Bowel training precedes bladder training. Watching older siblings provides role modeling and facilitates imitation for the toddler. The child should be introduced to the potty chair or toilet in a nonthreatening manner. PTS: 1 DIF: Cognitive Level: Comprehension REF: 930 OBJ: Nursing Process: Implementation MSC: Client Needs: Health Promotion and Maintenance 9. Which characteristic best describes the gross motor skills of a 24-month-old child? a. Skips c. Broad jumps b. Rides tricycle d. Walks up and down stairs The 24-month-old child can go up and down stairs alone with two feet on each step. Skipping and the ability to broad jump are skills acquired at age 3. Tricycle riding is achieved at age 4. PTS: 1 DIF: Cognitive Level: Comprehension REF: 929 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance 10. In the clinic waiting room, a nurse observes a parent showing an 18-month-old child how to make a tower out of blocks. In this situation the nurse should recognize that: a. Blocks at this age are used primarily for throwing. b. Toddlers are too young to imitate the behavior of others. c. Toddlers are capable of building a tower of blocks. d. Toddlers are too young to build a tower of blocks. This is a good parent-child interaction. The 18-month-old is capable of building a tower of 3 or 4 blocks. The ability to build towers of blocks usually begins at age 15 months. With ongoing development, the child is able to build taller towers. At this age, children imitate others around them and no longer throw blocks. PTS: 1 DIF: Cognitive Level: Comprehension REF: 929 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance 11. The parents of a newborn say that their toddler “hates the baby . . . he suggested that we put him in the trash can so the trash truck could take him away.” The nurse’s best reply is: a. “Let’s see if we can figure out why he hates the new baby.” b. “That’s a strong statement to come from such a small boy.” c. “Let’s refer him to counseling to work this hatred out. It’s not a normal response.” d. “That is a normal response to the birth of a sibling. Let’s look at ways to deal with this.” The arrival of a new infant represents a crisis for even the best-prepared toddler. Toddlers have their entire schedule and routines disrupted because of the new family member. The nurse should work with parents on ways to involve the toddler in the newborn’s care and help focus attention on the toddler. The toddler does not hate the infant. This is an expected response to the changes in routines and attention that affect the toddler. This is a normal response. The toddler can be provided with a doll to tend to its needs when the parent is performing similar care for the newborn. PTS: 1 DIF: Cognitive Level: Comprehension REF: 932 OBJ: Nursing Process: Planning MSC: Client Needs: Psychosocial Integrity 12. A toddler’s parent asks the nurse for suggestions on dealing with temper tantrums. The most appropriate recommendation is to: a. Punish the child. b. Leave the child alone until the tantrum is over. c. Ignore the behavior, provided that it is not injurious. d. Explain to child that this is wrong. The parent should be told that the best way to deal with temper tantrums is to ignore the behaviors, provided that the actions are not dangerous to the child. Tantrums are common during this age-group as the child becomes more independent and increasingly complex tasks overwhelm him or her. The parents and caregivers need to have consistent and developmentally appropriate expectations. Punishment and explanations will not be beneficial. PTS: 1 DIF: Cognitive Level: Comprehension REF: 932 OBJ: Nursing Process: Implementation MSC: Client Needs: Psychosocial Integrity 13. A parent asks the nurse about how to respond to negativism in toddlers. The most appropriate recommendation is to: a. Punish the child. b. Provide more attention. c. Ask child not always to say “no.” d. Reduce the opportunities for a “no” answer. The nurse should suggest to the parent that questions should be phrased with realistic choices rather than “yes” or “no” answers. This provides a sense of control for the toddler and reduces the opportunity for negativism. Negativism is not an indication of stubbornness or insolence and should not be punished. The negativism is not a function of attention; the child is testing limits to gain an understanding of the world. The toddler is too young to be asked to not always say “no.” PTS: 1 DIF: Cognitive Level: Analysis REF: 933 OBJ: Nursing Process: Planning MSC: Client Needs: Health Promotion and Maintenance 14. The parents of a 2-year-old tell the nurse that they are concerned because the toddler has started to use “baby talk” since the arrival of their new baby. The nurse should recommend that the parents: a. Ignore the “baby talk.” b. Explain to the toddler that “baby talk” is for babies. c. Tell the toddler frequently, “You are a big kid now.” d. Encourage the toddler to practice more advanced patterns of speech. The baby talk is a sign of regression in the toddler. It should be ignored, while praising the child for developmentally appropriate behaviors. Regression is children’s way of saying that they are expressing stress. The parents should not introduce new expectations and should allow the child to master the developmental tasks without criticism. PTS: 1 DIF: Cognitive Level: Application REF: 932 OBJ: Nursing Process: Planning MSC: Client Needs: Health Promotion and Maintenance 15. Parents tell the nurse that their toddler daughter eats little at mealtimes, only sits at the table with the family briefly, and wants snacks “all the time.” The nurse should recommend that the parents: a. Give her planned, frequent, and nutritious snacks. b. Offer rewards for eating at mealtimes. c. Avoid snacks so she is hungry at mealtimes. d. Explain to her in a firm manner what is expected of her. Most toddlers exhibit a physiologic anorexia in response to the decreased nutritional requirement associated with the slower growth rate. Parents should assist the child to develop healthy eating habits. The toddler is often unable to sit through a meal. Frequent nutritious snacks are a good way to ensure proper nutrition. To help with developing healthy eating habits, food should not be used as positive or negative reinforcement for behavior. The child may develop habits of overeating or eat nonnutritious foods in response. PTS: 1 DIF: Cognitive Level: Application REF: 934 OBJ: Nursing Process: Planning MSC: Client Needs: Health Promotion and Maintenance 16. A father tells the nurse that his daughter wants the same plate and cup used at every meal, even if they go to a restaurant. The nurse should explain that this is: a. A sign that the child is spoiled. c. Regression, common at this age. b. A way to exert unhealthy control. d. Ritualism, common at this age. The child is exhibiting the ritualism that is characteristic at this age. Ritualism is the need to maintain sameness and reliability. It provides a sense of comfort to the toddler. It will dictate certain principles in feeding practices, including rejecting a favorite food because it is served in a different container. This does not indicate a child who has unreasonable expectations or a need to exert control, but rather normal development. Toddlers use ritualistic behaviors to maintain necessary structure in their lives. This is not regression, which is a retreat from a present pattern of functioning. PTS: 1 DIF: Cognitive Level: Analysis REF: 934 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance 17. Developmentally, most children at age 12 months: a. Use a spoon adeptly. b. Relinquish the bottle voluntarily. c. Eat the same food as the rest of the family. d. Reject all solid food in preference to the bottle. By age 12 months, most children are eating the same food that is prepared for the rest of the family. Using a spoon usually is not mastered until age 18 months. The parents should be engaged in weaning a child from a bottle if that is the source of liquid. Toddlers should be encouraged to drink from a cup at the first birthday and weaned totally by 14 months. The child should be weaned from a milk/formula-based diet to a balanced diet that includes iron-rich sources of food. PTS: 1 DIF: Cognitive Level: Comprehension REF: 934 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance 18. The most effective way to clean a toddler’s teeth is for the: a. Child to brush regularly with toothpaste of his or her choice. b. Parent to stabilize the chin with one hand and brush with the other. c. Parent to brush the mandibular occlusive surfaces, leaving the rest for the child. d. Parent to brush the front labial surfaces, leaving the rest for the child. For young children, the most effective cleaning of teeth is done by the parents. Different positions can be used if the child’s back is to the adult. The adult should use one hand to stabilize the chin and the other to brush the child’s teeth. The child can participate in brushing, but for a thorough cleaning adult intervention is necessary. PTS: 1 DIF: Cognitive Level: Comprehension REF: 939 OBJ: Nursing Process: Implementation MSC: Client Needs: Health Promotion and Maintenance 19. The nurse is discussing with a parent group the importance of fluoride for healthy teeth. The nurse should recommend that the parents: a. Use fluoridated mouth rinses in children older than 1 year. b. Have children brush teeth with fluoridated toothpaste unless fluoride content of water supply is adequate. c. Give fluoride supplements to breastfed infants beginning at age 1 month. d. Determine whether water supply is fluoridated. The decision about fluoride supplementation cannot be made until it is known whether the water supply contains fluoride and the amount. It is difficult to teach this age-group to spit out the mouthwash. Swallowing fluoridated mouthwashes can contribute to fluorosis. Fluoridated toothpaste is still indicated, but very small amounts are used. Fluoride supplementation is not recommended until after age 6 months. PTS: 1 DIF: Cognitive Level: Analysis REF: 940 OBJ: Nursing Process: Implementation MSC: Client Needs: Health Promotion and Maintenance 20. An appropriate recommendation in preventing tooth decay in young children is to: a. Substitute raisins for candy. b. Serve sweets after a meal. c. Use honey or molasses instead of refined sugar. d. Serve sweets between meals. Sweets should be consumed with meals so the teeth can be cleaned afterward. This decreases the amount of time that the sugar is in contact with the teeth. Raisins, honey, and molasses are highly cariogenic and should be avoided. PTS: 1 DIF: Cognitive Level: Analysis REF: 940 OBJ: Nursing Process: Planning MSC: Client Needs: Health Promotion and Maintenance 21. The leading cause of death during the toddler period is: a. Injuries. c. Congenital disorders. b. Infectious diseases. d. Childhood diseases. Injuries are the single most common cause of death in children ages 1 through 4 years. It is the period of highest death rate from injuries of any childhood age-group except adolescence. Infectious and childhood diseases are less common cause of deaths in this age-group. Congenital disorders are the second leading cause of death in this age-group. PTS: 1 DIF: Cognitive Level: Comprehension REF: 941 OBJ: Nursing Process: Planning MSC: Client Needs: Health Promotion and Maintenance 22. The nurse recommends to parents that peanuts are not a good snack food for toddlers. The nurse’s rationale for this action is that: a. They are low in nutritive value. c. They cannot be entirely digested. b. They are very high in sodium. d. They can be easily aspirated. Foreign-body aspiration is common during the second year of life. Although they chew well, children at this age may have difficulty with large pieces of food such as meat and whole hot dogs and with hard foods such as nuts or dried beans. Peanuts have many beneficial nutrients but should be avoided because of the risk of aspiration in this age-group. The sodium level may be a concern, but the risk of aspiration is more important. Many foods pass through the gastrointestinal tract incompletely digested. This is not necessarily detrimental to the child. PTS: 1 DIF: Cognitive Level: Analysis REF: 948 OBJ: Nursing Process: Implementation MSC: Client Needs: Health Promotion and Maintenance 23. The parent of 16-month-old Chris asks, “What is the best way to keep Chris from getting into our medicines at home?” The nurse should advise that: a. “All medicines should be locked securely away.” b. “The medicines should be placed in high cabinets.” c. “Chris just needs to be taught not to touch medicines.” d. “Medicines should not be kept in the homes of small children.” The major reason for poisoning in the home is improper storage. Toddlers can climb, unlatch cabinets, and obtain access to high-security places. For medications, only a locked cabinet is safe. Toddlers can climb by using furniture. High places are not a deterrent to an exploring toddler. Toddlers are not able to generalize as dangerous all of the different forms of medications that may be available in the home. Teaching them not to touch medicines is not feasible. Many parents require medications for chronic illnesses. They must be taught safe storage for their home and when they visit other homes. PTS: 1 DIF: Cognitive Level: Application REF: 947 OBJ: Nursing Process: Implementation MSC: Client Needs: Health Promotion and Maintenance 24. The most fatal type of burn in the toddler age-group is: a. Flame burn from playing with matches. b. Scald burn from high-temperature tap water. c. Hot object burn from cigarettes or irons. d. Electric burn from electrical outlets. Flame burns from matches and lighters represent one of the most fatal types of burns in the toddler age-group. Scald burns from water, hot object burns from cigarettes or irons, and electric burns from outlets are all significant causes of burn injury. The child should be protected from these causes by reducing the temperature of the hot water in the home, keeping objects such as cigarettes and irons away from children, and placing protective guards over electrical outlets when not in use. PTS: 1 DIF: Cognitive Level: Comprehension REF: 946 OBJ: Nursing Process: Planning MSC: Client Needs: Health Promotion and Maintenance 25. The mother of a 14-month-old child is concerned because the child’s appetite has decreased. The best response for the nurse to make to the mother is: a. “It is important for your toddler to eat three meals a day and nothing in between.” b. “It is not unusual for toddlers to eat less.” c. “Be sure to increase your child’s milk consumption, which will improve nutrition.” d. “Giving your child a multivitamin supplement daily will increase your toddler’s appetite.” Toddlers need small, frequent meals. Nutritious selection throughout the day, rather than quantity, is more important with this age-group. Physiologically, growth slows and appetite decreases during the toddler period. Milk consumption should not exceed 16 to 24 oz daily. Juice should be limited to 4 to 6 oz per day. Increasing the amount of milk will only further decrease solid food intake. Supplemental vitamins are important for all children, but they do not increase appetite. PTS: 1 DIF: Cognitive Level: Application REF: 934 OBJ: Nursing Process: Implementation MSC: Client Needs: Physiologic Integrity 26. Which toy is the most developmentally appropriate for an 18- to 24-month-old child? a. A push-pull toy c. A bicycle with training wheels b. Nesting blocks d. A computer Push-pull toys encourage large muscle activity and are appropriate for toddlers. Nesting blocks are more appropriate for a 12- to 15-month-old child. A bicycle with training wheels is appropriate for a preschool or young school-age child. A computer can be appropriate as early as the preschool years. PTS: 1 DIF: Cognitive Level: Comprehension REF: 928 OBJ: Nursing Process: Teaching/Learning MSC: Client Needs: Health Promotion and Maintenance 27. What is the primary purpose of a transitional object? a. It helps the parents deal with the guilt they feel when they leave the child. b. It keeps the child quiet at bedtime. c. It is effective in decreasing anxiety in the toddler. d. It decreases negativism and tantrums in the toddler. Decreasing anxiety, particularly separation anxiety, is the function of a transitional object; it provides comfort to the toddler in stressful situations and helps make the transition from dependence to autonomy. A decrease in parental guilt (distress) is an indirect benefit of a transitional object. A transitional object may be part of a bedtime ritual, but it may not keep the child quiet at bedtime. A transitional object does not significantly affect negativity and tantrums, but it can comfort a child after tantrums. PTS: 1 DIF: Cognitive Level: Comprehension REF: 927 OBJ: Nursing Process: Implementation MSC: Client Needs: Health Promotion and Maintenance 28. Which comments indicate that the mother of a toddler needs further teaching about dental care? a. “We use well water so I give my toddler fluoride supplements.” b. “My toddler brushes his teeth with my help.” c. “My child will not need a dental checkup until his permanent teeth come in.” d. “I use a small nylon bristle brush for my toddler’s teeth.” Children should first see the dentist 6 months after the first primary tooth erupts and no later than age 30 months. Toddlers need fluoride supplements when they use a water supply that is not fluorinated. Toddlers also require supervision with dental care. The parent should finish brushing areas not reached by the child. A small nylon bristle brush works best for cleaning toddlers’ teeth. PTS: 1 DIF: Cognitive Level: Comprehension REF: 941 OBJ: Nursing Process: Evaluation MSC: Client Needs: Physiologic Integrity 29. What is helpful to tell a mother who is concerned about preventing sleep problems in her 2-year-old child? a. Have the child always sleep in a quiet, darkened room. b. Provide high-carbohydrate snacks before bedtime. c. Communicate with the child’s daytime caregiver about eliminating the afternoon nap. d. Use a night-light in the child’s room. The preschooler has a great imagination. Sounds and shadows can have a negative effect on sleeping behavior. Night-lights provide the child with the ability to visualize the environment and decrease the fear felt in a dark room. A dark, quiet room may be scary to a preschooler. High-carbohydrate snacks increase energy and do not promote relaxation. Most 2-year-olds take one nap each day. Many give up the habit by age 3. Insufficient rest during the day can lead to irritability and difficulty sleeping at night. PTS: 1 DIF: Cognitive Level: Application REF: 938 OBJ: Nursing Process: Implementation MSC: Client Needs: Physiologic Integrity 30. Steven, 16 months old, falls down a few stairs. He gets up and “scolds” the stairs as if they caused him to fall. This is an example of which of the following? a. Animism c. Irreversibility b. Ritualism d. Delayed cognitive development Animism is the attribution of lifelike qualities to inanimate objects. By scolding the stairs, the toddler is attributing human characteristics to them. Ritualism is the need to maintain sameness and reliability. It provides a sense of comfort to the toddler. Irreversibility is the inability to reverse or undo actions initiated physically. Steven is acting in an age-appropriate manner. PTS: 1 DIF: Cognitive Level: Comprehension REF: 926 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance 31. Which should the nurse expect for a toddler’s language development at age 18 months? a. Vocabulary of 25 words b. Increasing level of comprehension c. Use of phrases d. Approximately one third of speech understandable During the second year of life, level of comprehension and understanding of speech increases and is far greater than the child’s vocabulary. This is also true for bilingual children, who are able to achieve this linguistic milestone in both languages. The 18-month-old child has a vocabulary of 10 or more words. At this age, the child does not use one-word sentences or phrases. The child has a limited vocabulary of single words that are comprehensible. PTS: 1 DIF: Cognitive Level: Comprehension REF: 927 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance 32. Kimberly’s parents have been using a rearward-facing, convertible car seat since she was born. The parents should be taught that most car seats can be safely switched to the forward-facing position when the child reaches which age? a. 1 year c. 3 years b. 2 years d. 4 years It is now recommended that all infants and toddlers ride in rear-facing car safety seats until they reach the age of 2 years or the height or weight recommended by the car seat manufacturer. Children 2 years old and older who have outgrown the rear-facing height or weight limit for their car safety seat should use a forward-facing car safety seat with a harness up to the maximum height or weight recommended by the manufacturer. One year is too young to switch to a forward-facing position. PTS: 1 DIF: Cognitive Level: Application REF: 941 OBJ: Nursing Process: Implementation MSC: Client Needs: Safe and Effective Care Environment 33. Which play item should the nurse bring from the playroom to a hospitalized toddler in isolation? a. Small plastic Legos c. Brightly colored balloon b. Set of large plastic building blocks d. Coloring book and crayons Large plastic blocks are appropriate for a toddler in isolation. Play objects for toddlers must still be chosen with an awareness of danger from small parts. Large, sturdy toys without sharp edges or removable parts are safest. Small plastic toys such as Legos can cause choking or can be aspirated. Balloons can cause significant harm if swallowed or aspirated. Coloring book and crayons would be too advanced for a toddler. PTS: 1 DIF: Cognitive Level: Application REF: 948 OBJ: Nursing Process: Implementation MSC: Client Needs: Safe and Effective Care Environment 34. A nurse places some x-ray contrast the toddler is to drink in a small cup instead of a large cup. Which concept of a toddler’s preoperational thinking is the nurse using? a. Inability to conserve c. Centration b. Magical thinking d. Irreversibility The nurse is using the toddler’s inability to conserve. This is when the toddler is unable to understand the idea that a mass can be changed in size, shape, volume, or length without losing or adding to the original mass. Instead, toddlers judge what they see by the immediate perceptual clues given to them. A small glass means less amount of contrast. Magical thinking is believing that thoughts are all-powerful and can cause events. Centration is focusing on one aspect rather than considering all possible alternatives. Irreversibility is the inability to undo or reverse the actions initiated, such as being unable to stop doing an action when told. PTS: 1 DIF: Cognitive Level: Application REF: 926 OBJ: Nursing Process: Implementation MSC: Client Needs: Health Promotion and Maintenance 35. Parents need further teaching about the use of car safety seats if they make which statement? a. “Even if our toddler helps buckle the straps, we will double-check the fastenings.” b. “We won’t start the car until everyone is properly restrained.” c. “We won’t need to use the car seat on short trips to the store.” d. “We will anchor the car seat to the car’s anchoring system.” Parents need to be taught to always use the restraint even for short trips. Further teaching is needed if they make this statement. Parents have understood the teaching if they encourage the child to help attach buckles, straps, and shields but always double-check fastenings; do not start the car until everyone is properly restrained; and anchor the car safety seat securely to the car’s anchoring system and apply the harness snugly to the child. PTS: 1 DIF: Cognitive Level: Application REF: 941 OBJ: Nursing Process: Implementation MSC: Client Needs: Health Promotion and Maintenance MULTIPLE RESPONSE 36. Which are characteristic of the physical development of a 30-month-old child (select all that apply)? a. Birth weight has doubled. b. Primary dentition is complete. c. Sphincter control is achieved. d. Anterior fontanel is open. e. Length from birth is doubled. , C Usually by age 30 months, the primary dentition of 20 teeth is completed, and the child has sphincter control in preparation for bowel and bladder control. A doubling of birth weight, opening of the anterior fontanel, and doubling of length are not characteristic of the physical development of a 30-month-old child. PTS: 1 DIF: Cognitive Level: Application REF: 923 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance 37. Motor vehicle injuries are a significant threat to young children. Knowing this, the nurse plans a teaching session with a toddler’s parents on car safety. Which will she teach (select all that apply)? a. Secure in a rear-facing, upright, car safety seat. b. Place the car safety seat in the rear seat, behind the driver’s seat. c. Harness safety straps should be fit snugly. d. Place the car safety seat in the front passenger seat equipped with an air bag. e. After the age of 2 years, toddlers can be placed in a forward-facing car seat. , C, E Toddlers younger than 2 years should be secured in a rear-facing, upright, approved car safety seat. After the age of 2 years, a forward-facing car seat can be used. Harness straps should be adjusted to provide a snug fit. The car safety seat should be placed in the middle of the rear seat. Children younger than 13 years should not ride in a front passenger seat that is equipped with an air bag. PTS: 1 DIF: Cognitive Level: Comprehension REF: 944 OBJ: Nursing Process: Planning MSC: Client Needs: Health Promotion and Maintenance 38. The nurse is assessing parental knowledge of temper tantrums. Which are true statements regarding temper tantrums (select all that apply)? a. Temper tantrums are a common response to anger and frustration in toddlers. b. Temper tantrums often include screaming, kicking, throwing things, and head banging. c. Parents can effectively manage temper tantrums by giving in to the child’s demands. d. Children having temper tantrums should be safely isolated and ignored. e. Parents can learn to anticipate times when tantrums are more likely to occur. , B, D, E Temper tantrums are a common response to anger and frustration in toddlers. They occur more often when toddlers are tired, hungry, bored, or excessively stimulated. A nap prior to fatigue or a snack if mealtime is delayed will be helpful in alleviated the times when tantrums are most likely to occur. Tantrums may include screaming, kicking, throwing things, biting themselves, or banging their head. Effective management of tantrums includes safely isolating and ignoring the child. The child should learn that nothing is gained by having a temper tantrum. Giving in to the child’s demands only increases the behavior. PTS: 1 DIF: Cognitive Level: Comprehension REF: 933 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance 39. A nurse is planning care for a hospitalized toddler in the preoperational thinking stage. Which characteristics should the nurse expect in this stage (select all that apply)? a. Concrete thinking b. Egocentrism c. Animism d. Magical thinking e. Ability to reason , C, D The characteristics of preoperational thinking that occur for the toddler include egocentrism (views everything in relation to self), animism (believes that inert objects are alive), and magical thinking (believes that thinking something causes that event). Concrete thinking is seen in school-age children and ability to reason is seen with adolescents. PTS: 1 DIF: Cognitive Level: Application REF: 926 OBJ: Nursing Process: Planning MSC: Client Needs: Health Promotion and Maintenance 40. Which should the nurse teach to parents of toddlers about accidental poison prevention (select all that apply)? a. Keep toxic substances in the garage. b. Discard empty poison containers. c. Know the number of the nearest poison control center. d. Remove colorful labels from containers of toxic substances. e. Caution child against eating nonedible items, such as plants. , C, E To prevent accidental poisoning, parents should be taught to promptly discard empty poison containers, to know the number of the nearest poison control center, and to caution the child against eating nonedible items, such as plants. Parents should place all potentially toxic agents, including cosmetics, personal care items, cleaning products, pesticides, and medications, in a locked cabinet, not in the garage. Parents should be taught to never remove labels from containers of toxic substances. PTS: 1 DIF: Cognitive Level: Application REF: 942 OBJ: Nursing Process: Implementation MSC: Client Needs: Health Promotion and Maintenance 41. Which gross motor milestones should the nurse assess in an 18-month-old child (select all that apply)? a. Jumps in place with both feet b. Takes a few steps on tiptoe c. Throws ball overhand without falling d. Pulls and pushes toys e. Stands on one foot momentarily , C, D An 18-month-old child can jump in place with both feet, throw a ball overhand without falling, and pull and push toys. Taking a few steps on tiptoe and standing on one foot momentarily are not acquired until 30 months of age. Chapter 33: The Preschooler and Family MULTIPLE CHOICE 1. Which accomplishment would the nurse expect of a healthy 3-year-old child? a. Jump rope b. Ride a two-wheel bicycle c. Skip on alternate feet d. Balance on one foot for a few seconds Three-year-olds are able to accomplish the gross motor skill of balancing on one foot. Jumping rope, riding a two-wheel bike, and skipping on alternate feet are gross motor skills of 5-year-old children. PTS: 1 DIF: Cognitive Level: Comprehension REF: 953 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance 2. In terms of fine motor development, what could the 3-year-old child be expected to do? a. Tie shoelaces. b. Use scissors or a pencil very well. c. Draw a person with seven to nine parts. d. Copy (draw) a circle. Three-year-olds are able to accomplish the fine motor skill of drawing a circle. Tying shoelaces, using scissors or a pencil very well, and drawing a person with multiple parts are fine motor skills of 5-year-old children. PTS: 1 DIF: Cognitive Level: Comprehension REF: 958 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance 3. In terms of cognitive development, the 5-year-old child would be expected to: a. Use magical thinking. b. Think abstractly. c. Understand conservation of matter. d. Be able to comprehend another person’s perspective. Magical thinking is believing that thoughts can cause events. Abstract thought does not develop until school-age years. The concept of conservation is the cognitive task of school-age children ages 5 to 7 years. Five-year-olds cannot understand another’s perspective. PTS: 1 DIF: Cognitive Level: Comprehension REF: 953 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance 4. What is descriptive of the preschooler’s understanding of time? a. Has no understanding of time b. Associates time with events c. Can tell time on a clock d. Uses terms like “yesterday” appropriately In a preschooler’s understanding, time has a relation with events such as, “We’ll go outside after lunch.” Preschoolers develop an abstract sense of time at age 3 years. Children can tell time on a clock at age 7 years. Children do not fully understand use of time-oriented words until age 6 years. PTS: 1 DIF: Cognitive Level: Comprehension REF: 953 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance 5. The nurse is caring for a hospitalized 4-year-old boy, Ryan. His parents tell the nurse that they will be back to visit at 6 PM. When Ryan asks the nurse when his parents are coming, the nurse’s best response is: a. “They will be here soon.” b. “They will come after dinner.” c. “Let me show you on the clock when 6 PM is.” d. “I will tell you every time I see you how much longer it will be.” A 4-year-old understands time in relation to events such as meals. Children perceive “soon” as a very short time. The nurse may lose the child’s trust if his parents do not return in the time he perceives as “soon.” Children cannot read or use a clock for practical purposes until age 7 years. This answer assumes that the child understands the concept of hours and minutes, which is not developed until age 5 or 6 years. PTS: 1 DIF: Cognitive Level: Comprehension REF: 953 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance 6. A 4-year-old boy is hospitalized with a serious bacterial infection. He tells the nurse that he is sick because he was “bad.” The nurse’s best interpretation of this comment is that it is: a. A sign of stress. b. Common at this age. c. Suggestive of maladaptation. d. Suggestive of excessive discipline at home. Preschoolers cannot understand the cause and effect of illness. Their egocentrism makes them think that they are directly responsible for events, making them feel guilt for things outside of their control. Children of this age show stress by regressing developmentally or acting out. Maladaptation is unlikely. This comment does not imply excessive discipline at home. PTS: 1 DIF: Cognitive Level: Comprehension REF: 954 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance 7. In terms of language and cognitive development, a 4-year-old child would be expected to: a. Think in abstract terms. b. Follow simple commands. c. Understand conservation of matter. d. Comprehend another person’s perspective. Children ages 3 to 4 years can give and follow simple commands. Children cannot think abstractly at age 4 years. Conservation of matter is a developmental task of the school-age child. A 4-year-old child cannot comprehend another’s perspective. PTS: 1 DIF: Cognitive Level: Comprehension REF: 955 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance 8. Which type of play is most typical of the preschool period? a. Solitary c. Associative b. Parallel d. Team Associative play is group play in similar or identical activities but without rigid organization or rules. Solitary play is that of infants. Parallel play is that of toddlers. School-age children play in teams. PTS: 1 DIF: Cognitive Level: Comprehension REF: 956 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance 9. Imaginary playmates are beneficial to the preschool child because they: a. Take the place of social interactions. b. Take the place of pets and other toys. c. Become friends in times of loneliness. d. Accomplish what the child has already successfully accomplished. One purpose of an imaginary friend is to be a friend in time of loneliness. Imaginary friends do not take the place of social interactions but may encourage conversation. Imaginary friends do not take the place of pets or toys. They accomplish what the child is still attempting, not what has already been accomplished. PTS: 1 DIF: Cognitive Level: Analysis REF: 957 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance 10. Which characteristic best describes the language of a 3-year-old child? a. Asks meanings of words b. Follows directional commands c. Can describe an object according to its composition d. Talks incessantly, regardless of whether anyone is listening Because of the dramatic vocabulary increase at this age, 3-year-olds are known to talk incessantly, regardless of whether anyone is listening. A 4- to 5-year-old asks lots of questions and can follow simple directional commands. A 6-year-old can describe an object according to its composition. PTS: 1 DIF: Cognitive Level: Comprehension REF: 958 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance 11. By what age would the nurse expect that most children could understand prepositional phrases such as “under,” “on top of,” “beside,” and “in back of”? a. 18 months c. 3 years b. 24 months d. 4 years At 4 years, children can understand directional phrases. Children 18 to 24 months and 3 years of age are too young. PTS: 1 DIF: Cognitive Level: Comprehension REF: 955 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance 12. A useful skill that the nurse should expect a 5-year-old child to be able to master is to: a. Tie shoelaces. c. Hammer a nail. b. Use a knife to cut meat. d. Make change from a quarter. Tying shoelaces is a fine motor task typical of 5-year-olds. Using a knife to cut meat is a fine motor task of a 7-year-old. Hammering a nail and making change from a quarter are fine motor tasks of an 8- to 9-year-old. PTS: 1 DIF: Cognitive Level: Comprehension REF: 959 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance 13. The nurse is guiding parents in selecting a day care facility for their child. When making the selection, it is especially important to consider: a. Structured learning environment. b. Socioeconomic status of children. c. Cultural similarities of children. d. Teachers knowledgeable about development. A teacher knowledgeable about development will structure activities for learning. A structured learning environment is not necessary at this age. Socioeconomic status is not the most important factor in selecting a preschool. Preschool is about expanding experiences with others; cultural similarities are not necessary. PTS: 1 DIF: Cognitive Level: Comprehension REF: 957 OBJ: Nursing Process: Planning MSC: Client Needs: Health Promotion and Maintenance 14. The parent of a 4-year-old son tells the nurse that the child believes “monsters and the boogeyman” are in his bedroom at night. The nurse’s best suggestion for coping with this problem is to: a. Insist that the child sleep with his parents until the fearful phase passes. b. Suggest involving the child to find a practical solution such as a night-light. c. Help the child understand that these fears are illogical. d. Tell the child frequently that monsters and the boogeyman do not exist. A night-light shows a child that imaginary creatures do not lurk in the darkness. Letting the child sleep with parents or telling the child that these creatures do not exist will not get rid of the fears. A 4-year-old is in the preconceptual age and cannot understand logical thought. PTS: 1 DIF: Cognitive Level: Comprehension REF: 961 OBJ: Nursing Process: Planning MSC: Client Needs: Health Promotion and Maintenance 15. Preschoolers’ fears can best be dealt with by which intervention? a. Actively involving them in finding practical methods to deal with the frightening experience b. Forcing them to confront the frightening object or experience in the presence of their parents c. Using logical persuasion to explain away their fears and help them recognize how unrealistic the fears are d. Ridiculing their fears so they understand that there is no need to be afraid Actively involving the child in finding practical methods to deal with the frightening experience is the best way to deal with fears. Forcing a child to confront fears may make the child more afraid. Preconceptual thought prevents logical understanding. Ridiculing fears does not make them go away. PTS: 1 DIF: Cognitive Level: Comprehension REF: 961 OBJ: Nursing Process: Implementation MSC: Client Needs: Health Promotion and Maintenance 16. A normal characteristic of the language development of a preschool-age child is: a. Lisp. c. Echolalia. b. Stammering. d. Repetition without meaning. Stammering and stuttering are normal dysfluencies in preschool-age children. Lisps are not a normal characteristic of language development. Echolalia and repetition are traits of toddlers’ language. PTS: 1 DIF: Cognitive Level: Comprehension REF: 962 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance 17. During the preschool period, the emphasis of injury prevention should be placed on: a. Constant vigilance and protection. b. Punishment for unsafe behaviors. c. Education for safety and potential hazards. d. Limitation of physical activities. Education for safety and potential hazards is appropriate for preschoolers because they can begin to understand dangers. Constant vigilance and protection is not practical at this age since preschoolers are becoming more independent. Punishment may make children scared of trying new things. Limitation of physical activities is not appropriate. PTS: 1 DIF: Cognitive Level: Comprehension REF: 964 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance 18. Acyclovir (Zovirax) is given to children with chickenpox to: a. Minimize scarring. c. Prevent aplastic anemia. b. Decrease the number of lesions. d. Prevent spread of the disease. Acyclovir decreases the number of lesions, shortens duration of fever, and decreases itching, lethargy, and anorexia; however, it does not prevent scarring. Preventing aplastic anemia is not a function of acyclovir. Only quarantine of the infected child can prevent the spread of disease. PTS: 1 DIF: Cognitive Level: Comprehension REF: 973 OBJ: Nursing Process: Implementation MSC: Client Needs: Physiologic Integrity 19. Which medication may be given to high risk children after exposure to chickenpox to prevent varicella? a. Acyclovir b. Vitamin A c. Diphenhydramine hydrochloride d. Varicella zoster immune globulin (VZIG) VZIG is given to high risk children to help prevent the development of chickenpox. Immune globulin intravenous may also be recommended. Acyclovir is given to immunocompromised children to reduce the severity of symptoms. Vitamin A reduces morbidity and mortality associated with the measles. The antihistamine diphenhydramine is administered to reduce the itching associated with chickenpox. PTS: 1 DIF: Cognitive Level: Comprehension REF: 973 OBJ: Nursing Process: Implementation MSC: Client Needs: Physiologic Integrity 20. Vitamin A supplementation may be recommended for the young child who has: a. Mumps. c. Measles (rubeola). b. Rubella. d. Erythema infectiosum. Evidence shows that vitamin A decreases morbidity and mortality associated with measles. Vitamin A will not lessen the effects of mumps, rubella, or fifth disease. PTS: 1 DIF: Cognitive Level: Comprehension REF: 973 OBJ: Nursing Process: Implementation MSC: Client Needs: Physiologic Integrity 21. When is a child with chickenpox considered to be no longer contagious? a. When fever is absent c. 24 hours after lesions erupt b. When lesions are crusted d. 8 days after onset of illness When the lesions are crusted, the chickenpox is no longer contagious. This may be a week after onset of disease. The child is still contagious once the fever has subsided and after the lesions erupt, and may or may not be contagious any time after 6 days as long as all lesions are crusted over. PTS: 1 DIF: Cognitive Level: Comprehension REF: 965 OBJ: Nursing Process: Assessment MSC: Client Needs: Physiologic Integrity 22. The nurse is performing an assessment on a child and notes the presence of Koplik’s spots. In which communicable disease are Koplik’s spots present? a. Rubella c. Chickenpox (varicella) b. Measles (rubeola) d. Exanthema subitum (roseola) Koplik’s spots are small, irregular red spots with a minute, bluish white center found on the buccal mucosa 2 days before systemic rash. Koplik’s spots are not present with rubella, varicella, or roseola. PTS: 1 DIF: Cognitive Level: Application REF: 967 OBJ: Nursing Process: Assessment MSC: Client Needs: Physiologic Integrity 23. Which statement best describes a child who is abused by the parent(s)? a. Unintentionally contributes to the abusing situation b. Belongs to a low socioeconomic population c. Is healthier than the nonabused siblings d. Abuses siblings in the same way as child is abused by the parent(s) A child’s temperament, position in the family, additional physical needs, activity level, or degree of sensitivity to parental needs unintentionally contributes to the abusing situation. Socioeconomic status is an environmentalcharacteristic. This child is less likely to be abused than one who is premature, disabled, or very young. The abused child does not in turn abuse his or her siblings. PTS: 1 DIF: Cognitive Level: Comprehension REF: 980 OBJ: Nursing Process: Assessment MSC: Client Needs: Psychosocial Integrity 24. A common characteristic of those who sexually abuse children is that they: a. Pressure the victim into secrecy. b. Are usually unemployed and unmarried. c. Are unknown to victims and victims’ families. d. Have many victims that are each abused only once. Sex offenders may pressure the victim into secrecy, regarding the activity as a “secret between us” that other people may take away if they find out. Abusers are often employed upstanding members of the community. Most sexual abuse is committed by men and persons who are well known to the child. Abuse is often repeated with the same child over time. The relationship may start insidiously without the child realizing that sexual activity is part of the offer. PTS: 1 DIF: Cognitive Level: Comprehension REF: 980 OBJ: Nursing Process: Assessment MSC: Client Needs: Psychosocial Integrity 25. Which statement, made by a 4-year-old child’s father, is true about the care of the preschooler’s teeth? a. “Because the ‘baby teeth’ are not permanent, they are not important to the child.” b. “My son can be encouraged to brush his teeth after I have thoroughly cleaned his teeth.” c. “My son’s ‘permanent teeth’ will begin to come in at 4 to 5 years of age.” d. “Fluoride supplements can be discontinued when my son’s ‘permanent teeth’ erupt.” Toddlers and preschoolers lack the manual dexterity to remove plaque adequately, so parents must assume this responsibility. Deciduous teeth are important because they maintain spacing and play an important role in the growth and development of the jaws and face and in speech development. Secondary teeth erupt at about 6 years of age. If the family does not live in an area where fluoride is included in the water supply, fluoride supplements should be continued. PTS: 1 DIF: Cognitive Level: Application REF: 964 OBJ: Nursing Process: Evaluation MSC: Client Needs: Physiologic Integrity 26. In providing anticipatory guidance to parents whose child will soon be entering kindergarten, which is a critical factor in preparing a child for kindergarten entry? a. The child’s ability to sit still b. The child’s sense of learned helplessness c. The parent’s interactions and responsiveness to the child d. Attending a preschool program Interactions between the parent and child are an important factor in the development of academic competence. Parental encouragement and support maximize a child’s potential. The child’s ability to sit still is important to learning; however, parental responsiveness and involvement are more important factors. Learned helplessness is the result of a child feeling that he or she has no effect on the environment and that his or her actions do not matter. Parents who are actively involved in a supportive learning environment will demonstrate a more positive approach to learning. Preschool and day care programs can supplement the developmental opportunities provided by parents at home, but they are not critical in preparing a child for entering kindergarten. PTS: 1 DIF: Cognitive Level: Comprehension REF: 957 OBJ: Nursing Process: Planning MSC: Client Needs: Health Promotion and Maintenance 27. A 4-year-old child tells the nurse that she does not want another blood sample drawn because “I need all my insides, and I don’t want anyone taking them out.” Which is the nurse’s best interpretation of this? a. Child is being overly dramatic. b. Child has a disturbed body image. c. Preschoolers have poorly defined body boundaries. d. Preschoolers normally have a good understanding of their bodies. Preschoolers have little understanding of body boundaries, which leads to fears of mutilation. The child is not capable of being dramatic at 4 years of age. She truly has fear. Body image is just developing in the school-age child. Preschoolers do not have good understanding of their bodies. PTS: 1 DIF: Cognitive Level: Application REF: 961 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance 28. Parents tell the nurse that they found their 3-year-old daughter and a male cousin of the same age inspecting each other closely as they used the bathroom. Which is the most appropriate recommendation the nurse should make? a. Punish children so this behavior stops. b. Neither condone nor condemn the curiosity. c. Allow children unrestricted permission to satisfy this curiosity. d. Get counseling for this unusual and dangerous behavior. Three-year-olds become aware of anatomic differences and are concerned about how the other “works.” Such exploration should not be condoned or condemned. Children should not be punished for this normal exploration. Encouraging the children to ask questions of the parents and redirecting their activity are more appropriate than giving permission. Exploration is age-appropriate and not dangerous behavior. PTS: 1 DIF: Cognitive Level: Application REF: 961 OBJ: Nursing Process: Implementation MSC: Client Needs: Health Promotion and Maintenance 29. Which common childhood communicable disease may cause severe defects in the fetus when it occurs in its congenital form? a. Erythema infectiosum c. Rubeola b. Roseola d. Rubella Rubella causes teratogenic effects on the fetus. There is a low risk of fetal death to those in contact with children affected with fifth disease. Roseola and rubeola are not dangerous to the fetus. PTS: 1 DIF: Cognitive Level: Comprehension REF: 970 OBJ: Nursing Process: Assessment MSC: Client Needs: Physiologic Integrity 30. Which is the causative agent of scarlet fever? a. Enteroviruses b. Corynebacterium organisms c. Scarlet fever virus d. Group A b-hemolytic streptococci (GABHS) GABHS infection causes scarlet fever. Enteroviruses do not cause the same complications. Corynebacterium organisms cause diphtheria. Scarlet fever is not caused by a virus. PTS: 1 DIF: Cognitive Level: Knowledge REF: 971 OBJ: Nursing Process: Assessment MSC: Client Needs: Physiologic Integrity 31. Which is probably the most important criterion on which to base the decision to report suspected child abuse? a. Inappropriate parental concern for the degree of injury b. Absence of parents for questioning about child’s injuries c. Inappropriate response of child d. Incompatibility between the history and injury observed Conflicting stories about the “accident” are the most indicative red flags of abuse. Inappropriate response of caregiver or child may be present, but is subjective. Parents should be questioned at some point during the investigation. PTS: 1 DIF: Cognitive Level: Application REF: 977 OBJ: Nursing Process: Assessment MSC: Client Needs: Psychosocial Integrity MULTIPLE RESPONSE 32. Which play patterns does a 3-year-old child typically display (select all that apply)? a. Imaginary play b. Parallel play c. Cooperative play d. Structured play e. Associative play , B, C, E Children between ages 3 and 5 years enjoy parallel and associative play. Children learn to share and cooperate as they play in small groups. Play is often imitative, dramatic, and creative. Imaginary friends are common around age 3 years. Structured play is typical of school-age children. PTS: 1 DIF: Cognitive Level: Comprehension REF: 956-957 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance 33. Strict isolation is required for a child who is hospitalized with (select all that apply): a. Mumps. b. Chickenpox. c. Exanthema subitum (roseola). d. Erythema infectiosum (fifth disease). e. Parvovirus B19. , B, C, D Childhood communicable diseases requiring strict transmission-based precautions (Contact, Airborne, and Droplet Precautions) include diphtheria, chickenpox, measles, mumps, tuberculosis, adenovirus, Haemophilus influenzae type B, mumps, pertussis, plague, streptococcal pharyngitis, and scarlet fever. Strict isolation is not required for parvovirus B19. PTS: 1 DIF: Cognitive Level: Comprehension REF: 968 OBJ: Nursing Process: Implementation MSC: Client Needs: Safe and Effective Care Environment 34. In terms of language and cognitive development, a 4-year-old child would be expected to have which traits (select all that apply)? a. Think in abstract terms. b. Follow directional commands. c. Understand conservation of matter. d. Use sentences of eight words. e. Tell exaggerated stories. , E Children ages 3 to 4 years can give and follow simple commands and tell exaggerated stories. Children cannot think abstractly at age 4 years. Conservation of matter is a developmental task of the school-age child. Five-year-old children use sentences with eight words with all parts of speech. PTS: 1 DIF: Cognitive Level: Application REF: 955 OBJ: Nursing Process: Assessment MSC: Client Needs: Health Promotion and Maintenance 35. Which toys should a nurse provide to promote imaginative play for a 3-year-old hospitalized child (select all that apply)? a. Plastic telephone b. Hand puppets c. Jigsaw puzzle (100 pieces) d. Farm animals and equipment e. Jump rope , B, D To promote imaginative play for a 3-year-old child, the nurse should provide: dress-up clothes, dolls and dollhouses, housekeeping toys, play-store toys, telephones, farm animals and equipment, village sets, trains, trucks, cars, planes, hand puppets, and medical kits. A 100-piece jigsaw puzzle and a jump rope would be appropriate for a young, school-age child but not a 3-year-old child. [Show More]
Last updated: 2 years ago
Preview 1 out of 177 pages

Buy this document to get the full access instantly
Instant Download Access after purchase
Buy NowInstant download
We Accept:

Reviews( 0 )
$14.00
Can't find what you want? Try our AI powered Search
Document information
Connected school, study & course
About the document
Uploaded On
Feb 03, 2020
Number of pages
177
Written in

Additional information
This document has been written for:
Uploaded
Feb 03, 2020
Downloads
0
Views
157



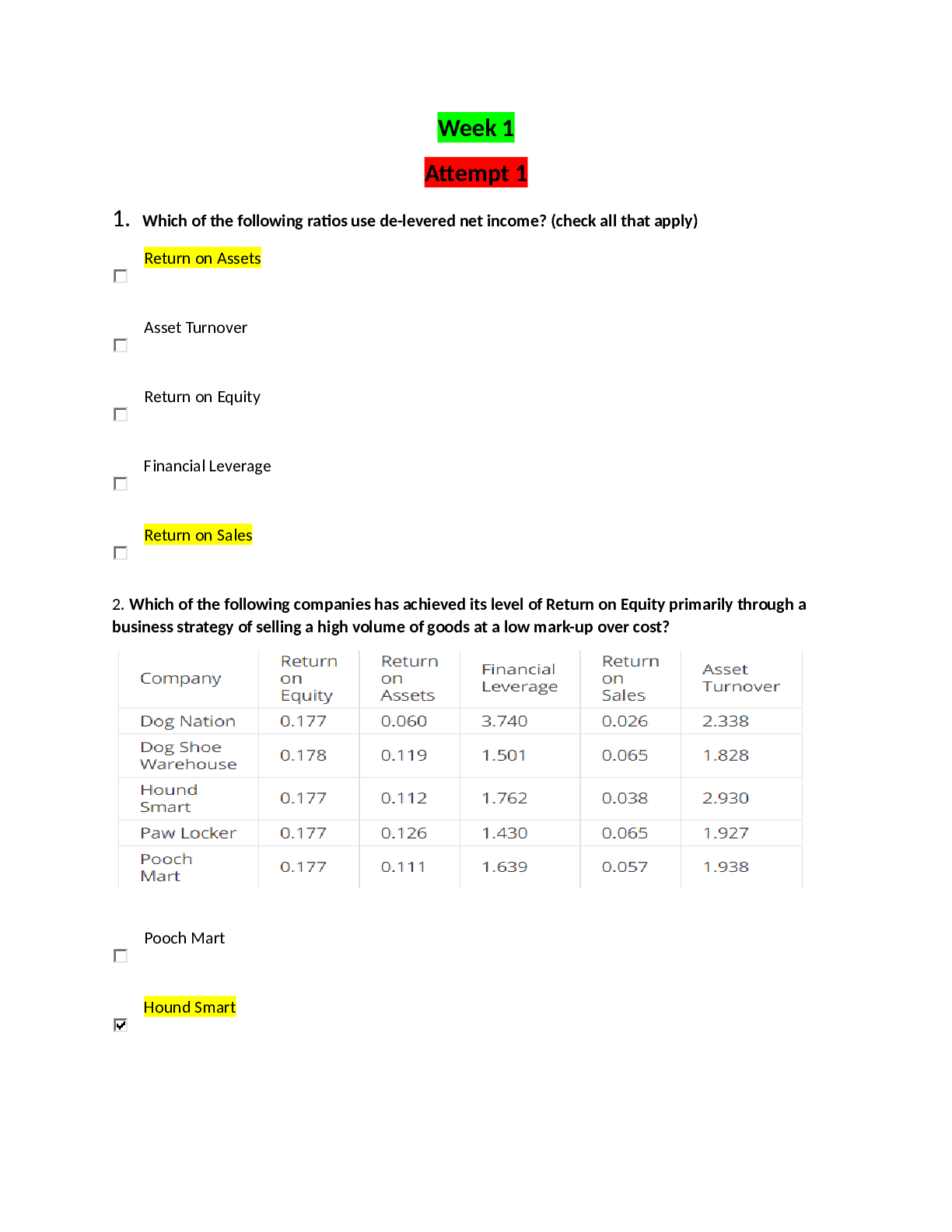
.png)
.png)
.png)
.png)
.png)
.png)
.png)