*NURSING > QUESTIONS & ANSWERS > Chamberlain College of Nursing - NR 509Chest Pain SOAP Note/Exam. All Filled and Graded A (All)
Chamberlain College of Nursing - NR 509Chest Pain SOAP Note/Exam. All Filled and Graded A
Document Content and Description Below
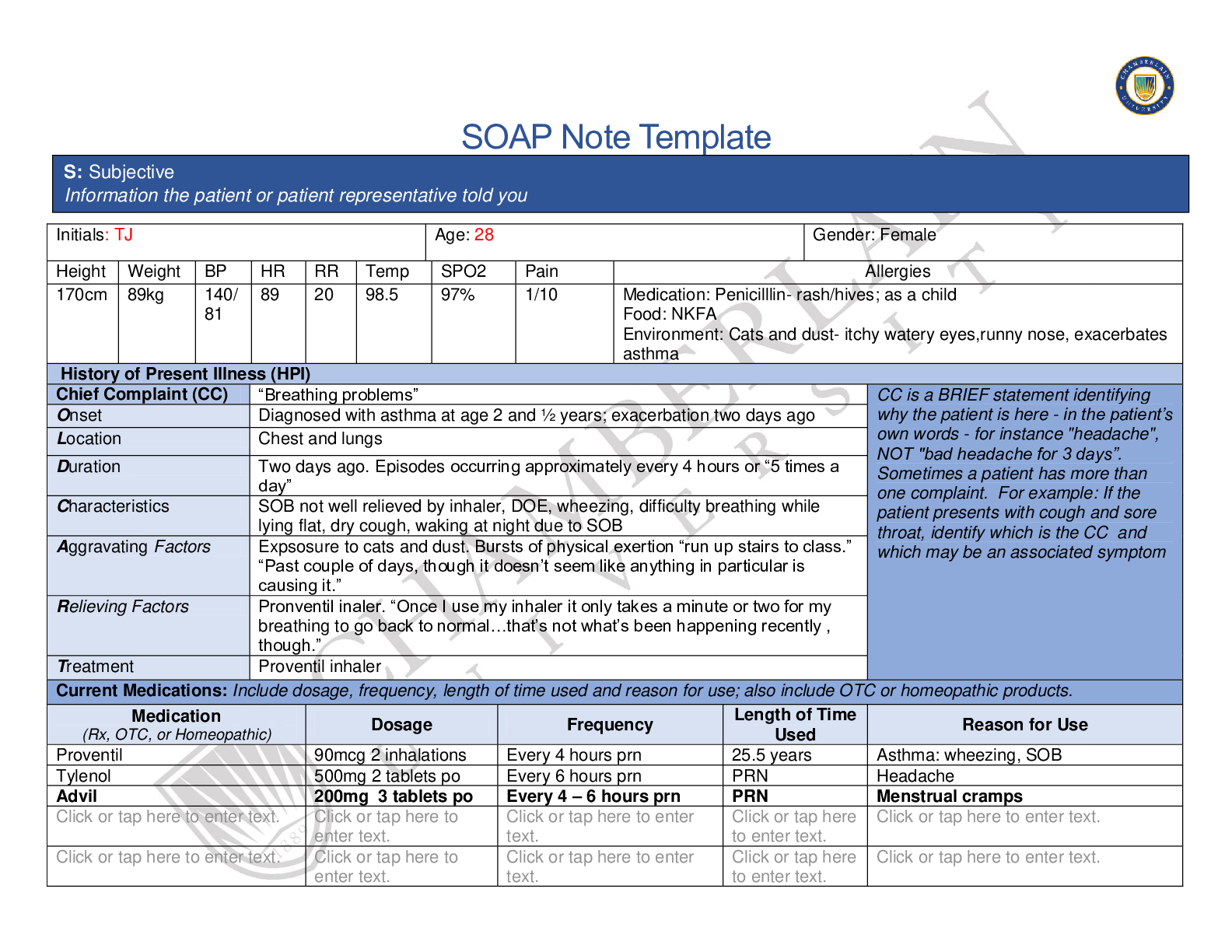
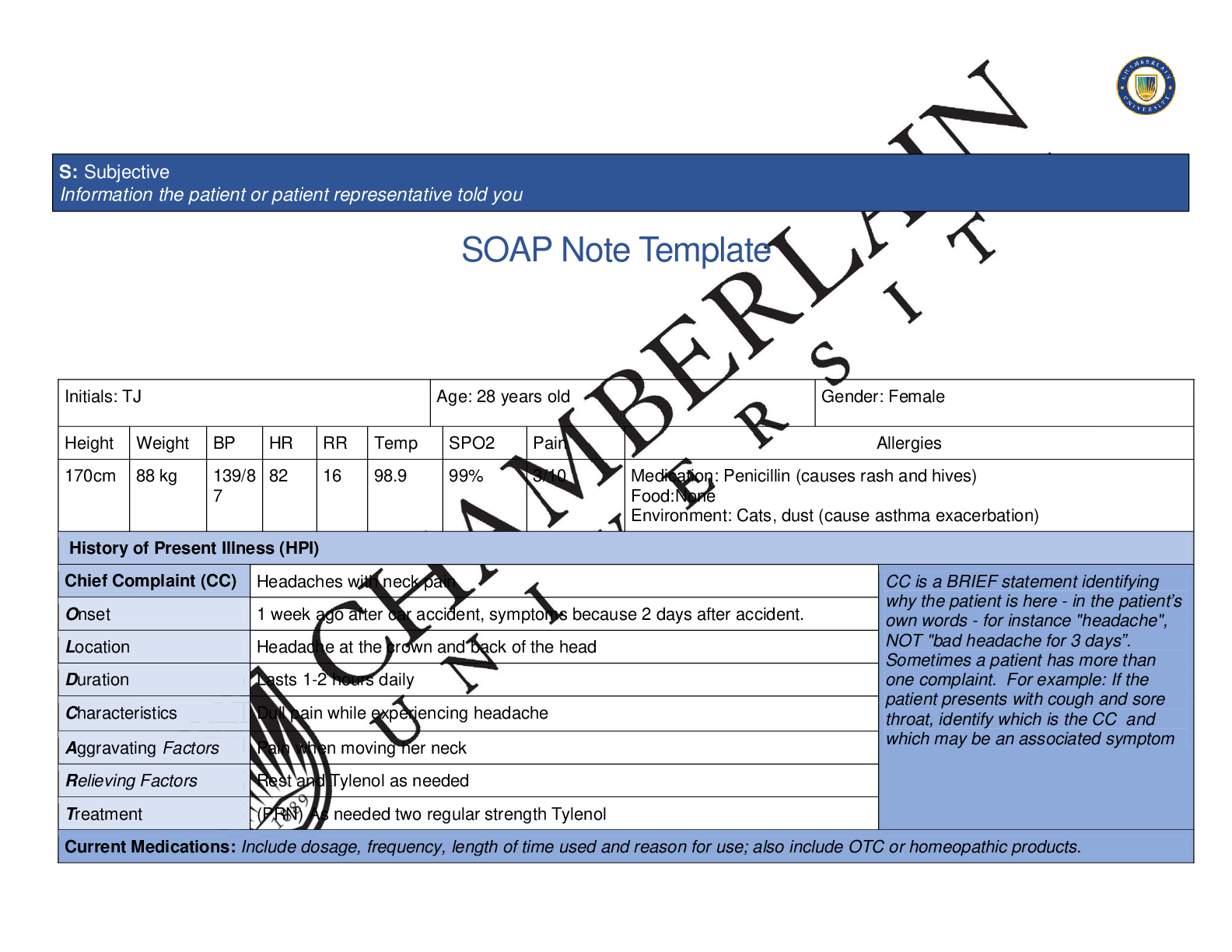
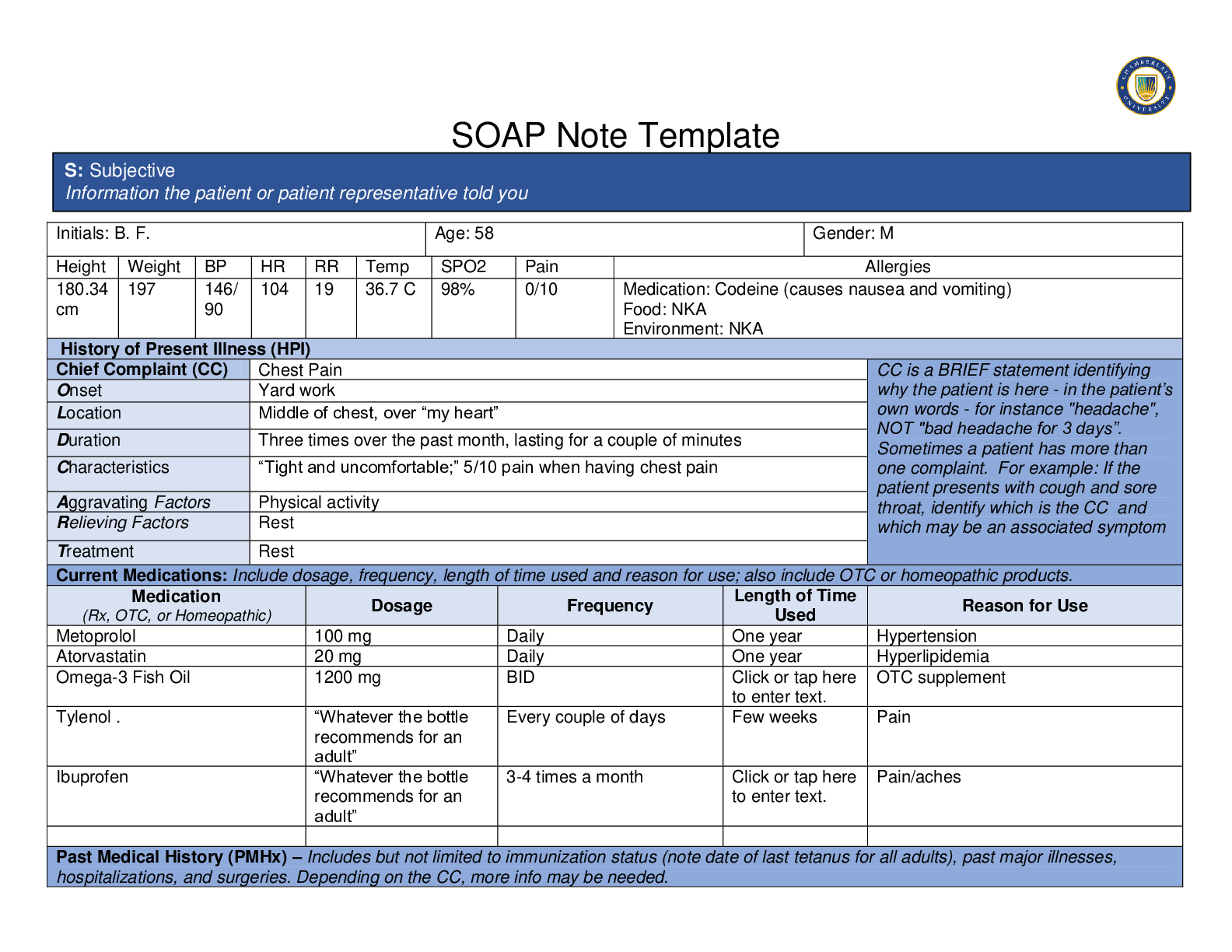
SOAP Note Template Initials: B. F. Age: 58 Gender: M Height Weight BP HR RR Temp SPO2 Pain Allergies 180.34 cm 197 146/ 90 104 19 36.7 C 98% 0/10 Medication: Codeine (causes nausea and vomiting... ) Food: NKA Environment: NKA History of Present Illness (HPI) Chief Complaint (CC) Chest Pain CC is a BRIEF statement identifying why the patient is here - in the patient’s own words - for instance "headache", NOT "bad headache for 3 days”. Sometimes a patient has more than one complaint. For example: If the patient presents with cough and sore throat, identify which is the CC and which may be an associated symptom Onset Yard work Location Middle of chest, over “my heart” Duration Three times over the past month, lasting for a couple of minutes Characteristics “Tight and uncomfortable;” 5/10 pain when having chest pain Aggravating Factors Physical activity Relieving Factors Rest Treatment Rest Current Medications: Include dosage, frequency, length of time used and reason for use; also include OTC or homeopathic products. Medication (Rx, OTC, or Homeopathic) Dosage Frequency Length of Time Used Reason for Use Metoprolol 100 mg Daily One year Hypertension Atorvastatin 20 mg Daily One year Hyperlipidemia Omega-3 Fish Oil 1200 mg BID Click or tap here OTC supplement Tylenol . “Whatever the bottle recommends for an adult” Every couple of days Few weeks Pain Ibuprofen “Whatever the bottle recommends for an adult” 3-4 times a month Click or tap here Pain/aches Past Medical History (PMHx) – Includes but not limited to immunization status (note date of last tetanus for all adults), past major illnesses, hospitalizations, and surgeries. Depending on the CC, more info may be needed. S: Subjective Information the patient or patient representative told youHypertension, Stage II - diagnosed 2018 Hyperlipidemia - diagnosed 2018 No hospitalizations No surgical history Immunizations up-to-date Influenza vaccine 2018 Social History (Soc Hx) - Includes but not limited to occupation and major hobbies, family status, tobacco and alcohol use, and any other pertinent data. Include health promotion such as use seat belts all the time or working smoke detectors in the house. Civil engineer Married for 27 years with two children: son 26 year old and daughter 19 year old hobbies - fish, sports, and small electronics repair Does not smoke or vape Exposure to secondhand smoke - almost never Alcohol - beer; 2 or 3 beers on the weekends, bourbon occasionally No illicit drug use Blood pressure check- only during checkups Stressors - concern about this chest pain; other than that, low stress Exercise - used to bicycle until it got stolen a couple of years ago. Have not had much regular exercise since Nutrition - Breakfast: Instant breakfast or granola bar; on weekends, eggs, pancakes, bacon, hash browns Lunch: Turkey or Italian sub or salad if “feeling healthy or guilty” Dinner: Grilled meats and veggies Salt intake - Does not pay attention to it Water intake - At least four glasses, probably more a day Caffeine - one to two cups of coffee almost daily Soda - “Once in a blue moon; avoiding it 99% of the time” Family History (Fam Hx) - Includes but not limited to illnesses with possible genetic predisposition, contagious or chronic illnesses. Reason for death of any deceased first degree relatives should be included. Include parents, grandparents, siblings, and children. Include grandchildren if pertinent. Mother - Type II diabetes and hypertension Father - Obesity, hypertension, and hyperlipidemia; Decease at 75 years old of colon cancer Brother - Died at age 24 in motor vehicle accident Sister - Type II diabetes and hypertension Son - None Daughter - asthma, diagnosed at age 19 Maternal grandmother - died of breast cancer at the age of 65 Maternal grandfather - died of heart attack at the age of 54 Paternal grandmother - died of pneumonia at age 78 Paternal grandfather - died of “old age” at age 85Review of Systems (ROS): Address all body systems that may help rule in or out a differential diagnosis Check the box next to each positive symptom and provide additional details. Constitutional Skin HEENT ☐Fatigue - denies ☐Weakness - denies ☐Fever/Chills - denies ☐Weight Gain - denies ☐Weight Loss - denies ☐Trouble Sleeping - denies ☐Night Sweats - denies ☐Other: Click or tap here to enter text. ☐Itching - denies ☐Rashes - denies ☐Nail Changes - denies ☐Skin Color Changes - denies ☐Other: Click or tap here to enter text. ☐Diplopia - denies ☐Eye Pain - denies ☐Eye redness - denies ☐Vision changes - denies ☐Photophobia - denies ☐Eye discharge - denies ☐Earache - denies ☐Tinnitus - denies ☐Epistaxis - denies ☐Vertigo - denies ☐Hearing Changes - denies ☐Hoarseness - denies ☐Oral Ulcers - denies ☐Sore Throat - denies ☐Congestion - denies ☐Rhinorrhea - denies ☐Other: . Respiratory Neuro Cardiovascular ☐Cough - denies ☐Hemoptysis - denies ☐Dyspnea - denies ☐Wheezing - denies ☐Pain on Inspiration - denies ☐Sputum Production ☐Other: . ☐Syncope or Lightheadedness - denies ☐Headache - denies ☐Numbness - denies ☐Tingling - denies ☐Sensation Changes - denies ☐Speech Deficits - denies ☐Other: Click or tap here to enter text. ☐Chest pain - Middle of chest, over “my heart.” Started while doing yard work. Three times over the past month, lasting for a couple of minutes. “Tight and uncomfortable;” 5/10 pain. Worse with physical activity. ☐SOB - denies ☐Exercise Intolerance - chest pain worsens with activity ☐Orthopnea - denies ☐Edema - denies. ☐Murmurs - denies ☐Palpitations - denies ☐Faintness - denies ☐OC Changes - denies ☐Claudications - denies ☐PND - denies ☐Other: Click or tap here to enter text. MSK GI GU PSYCH ☐Pain - denies ☐Stiffness - denies ☐Crepitus - denies ☐Swelling - denies ☐Limited ROM - denies ☐Nausea/Vomiting - denies ☐Dysphasia - denies ☐Diarrhea - denies ☐Appetite Change - denies ☐Heartburn - denies ☐Urgency - denies ☐Dysuria - denies ☐Burning - denies ☐Hematuria - denies ☐Polyuria - denies ☐Stress - denies ☐Anxiety - feeling anxious not knowing what’s going on with his chest ☐Depression - denies☐Redness - denies ☐Misalignment - denies ☐Other: Click or tap here to enter text. ☐Blood in Stool - denies ☐Abdominal Pain - denies ☐Excessive Flatus - denies ☐Food Intolerance - denies ☐Rectal Bleeding - denies ☐Other: . ☐Nocturia - denies ☐Incontinence - denies ☐Other: Click or tap here to enter text. ☐Suicidal/Homicidal Ideation - denies ☐Memory Deficits - denies ☐Mood Changes - denies ☐Trouble Concentrating - denies ☐Other: Click or tap here to enter text. GYN ☐Rash - denies ☐Discharge - N/A ☐Itching - denies ☐Irregular Menses - N/A/ ☐Dysmenorrhea - N/A ☐Foul Odor - denies ☐Amenorrhea - N/A ☐LMP - N/A ☐Contraception - denies ☐Other:. Body System Positive Findings Negative Findings General . Alert and oriented. Dressed appropriately. Not in distress Skin . No signs of pallor, cyanosis, jaundice, rashes, or mottling of the skin. No visible abnormal findings in bilateral hands No visible abnormal lower extremities No tenting HEENT . No visible abnormal findings on the face Jugular vein distention - 4 cm or less above the sternal angle Respiratory Fine crackles present in posterior right lower lobe and posterior left lower lobe Chest symmetrical No visible abnormal findings on the chest Breath sounds present in all areas O: Objective Information gathered during the physical examination by inspection, palpation, auscultation, and palpation. If unable to assess a body system, write “Unable to assess”. Document pertinent positive and negative assessment findings.Neuro . . Cardiovascular Bruit in right carotid artery S3 audible Gallops present on auscultation Thrill present on palpation in right carotid artery with an amplitude of 3+ (increased) PMI displaced laterally, less than 3 cm, and brisk and tapping in amplitude Amplitude 1+ in bilateral popliteal arteries Amplitude 1+ in bilateral tibial arteries Amplitude 1+ in bilateral dorsalis pedis arteries Jugular vein distention - 4 cm or less above the sternal angle No visible abnormal findings in nail changes of bilateral hands No visible abnormal findings in nail changes in bilateral feet No edema in bilateral lower extremities Capillary refill time is less than 3 seconds in fingers and toes No bruit in left carotid arteries S1 and S2 audible No bruit on auscultation in abdominal aorta No bruit on auscultation in bilateral renal arteries No bruit on auscultation in bilateral iliac arteries No bruit on auscultation in bilateral femoral arteries No thrill present on palpation in left carotid artery ; amplitude of 2+ (expected) No thrill and 2+ on palpation in bilateral branchial arteries No thrill and 2+ on palpation in bilateral radial arteries No thrill and 2+ on palpation in bilateral femoral arteries No thrill present on palpation in bilateral popliteal arteries No thrill present on palpation in bilateral tibial arteries No thrill present on palpation in bilateral dorsalis pedis arteries EKG - sinus rhythm and no ST elevation Musculoskeletal . . Gastrointestinal Rounded abdomen Abdomen symmetrical and no visible abnormal findings Bowel sounds present and normoactive in all four quadrants No tenderness or other additional observations on light palpation No palpable mass on deep palpation Liver palpable and no friction rub Spleen not palpable, no friction rub, and tympany on percussion All areas of abdomen generally tympanic Liver span between 6-12 cm Genitourinary . Bilateral kidneys not palpable Psychiatric . . Gynecological . . Problem List 1. Chest pain. 6 Activity intolerance 11 . 2 Hyperlipidemia 7 Anxiety 12 . 3 Hypertension 8 Displaced PMI 13 . 4 Hepatomegaly 9 . 14 . 5 Obesity 10 . 15 . Diagnosis ICD-10 Code Pertinent Findings Stable angina I20.9 Chest pain that is relieved by rest Carotid stenosis I65.29 Bruit in right carotid artery Systolic congestive heart failure I50.2 Fine crackles present in posterior right lower lobe and posterior left lower lobe. S3. Displaced PMI. Diagnostics: List tests you will order this visit Test Rationale/Citation Troponin and Ck-MB Cardiac markers are used in the diagnosis and risk stratification of patients with chest pain and suspected acute coronary syndrome (Adamson et al., 2018). A: Assessment Medical Diagnoses. Provide 3 differential diagnoses which may provide an etiology for the CC. The first diagnosis (presumptive diagnosis) is the diagnosis with the highest priority. Provide the ICD-10 code and pertinent findings to support each diagnosis.Chest x-ray Chest x-ray is the first line procedure to assess for pulmonary congestion (Cardinale, Priola, Moretti, & Volpicelli, 2014). BNP A useful diagnostic test for heart failure (Yoo, 2014). Lipid panel A high level of triglycerides in the blood is also associated with an increased risk of developing cardiovascular disease (Ryan, Heath, & Cook, 2018). TEE (transesophageal echocardiography) It can be used to diagnose coronary heart disease, heart attack, cardiomyopathy, carotid stenosis, and any injury to the heart or aorta (Maxwell, Konoske, & Mark, 2016). Medications: List medications/treatments including OTC drugs you will order and “continue previous meds” if pertinent. Drug Dosage Length of Treatment Rationale/Citation Aspirin 81 mg Continuous Low-dose aspirin reduces major cardiac events by up to 30% (Wee, Burns, and Bett, 2015). Lisinopril 5 mg 2 weeks Individuals with stable angina who have hypertension should be treated with an ACE inhibitor (Alyani & Uzokov, 2017). Since I am also prescribing lasix, I will start lisinopril at 5 mg (Epocrates, 2019). Lasix 10 mg 2 weeks Loop diuretics remain the drug choice for treatments patients with heart failure (Casu & Merella, 2015). Nitroglycerin 0.3 mg SL q5 min; max - 3 doses within 15 min 2 weeks Nitrates are used to treat acute episodes of angina (Boden, Padal, Cabral, Buschmann, & Sidhu, 2015). Continue previous meds . . . Referral/Consults: Cardiology Rationale/Citation A cardiologist has special training and skill in finding, treating and preventing diseases of the heart and blood vessels (Marques et al., 2014). Their skills and training are required for decisions involving cardiac catheterization or balloon angioplasty. Education:Associated symptoms of severe angina or heart attack Diet and exercise Nitroglycerin usage Rationale/Citation Aside from chest pain, individual with severe angina or heart attack may have other symptoms such as shortness of breath, nausea, vomiting, palpitations, dizziness, tingling sensation in either arm or vague abdominal discomfort (Aroesty & Kannam, 2019). It is important for individuals to be knowledgeable that there are other symptoms of angina and heart attack than the classical presentation of chest pain. Diet and exercise are an important part of one’s heart health. A lowsaturated fat, high-fiber, high plant food diet and limiting salt can reduce the risk of developing heart disease (Centers for Disease Control and Prevention, 2015). Physical activity can lower blood pressure and cholesterol and help maintain a healthy weight. Nitroglycerin is a small pill that is placed under the tongue, which will dissolve, if chest pain occurs. While the nitroglycerin is dissolving and being absorbed by the body, the individual should sit down because the medication may make you dizzy or lightheaded (Aroesty & Kannam, 2019). Follow Up: Indicate when patient should return to clinic and provide detailed instructions indicating if the patient should return sooner than scheduled or seek attention elsewhere. Follow up appointment in two weeks. If chest pain continues, go to the Rationale/Citation Follow up appointment to reER. Also if new symptoms develop such as shortness of breath, nausea, vomiting, palpitations, dizziness, tingling sensation in either arm or vague abdominal discomfort, the individual should go to the ER right away. assess chest pain and new medications. Individual with severe angina or heart attack may have other symptoms such as shortness of breath, nausea, vomiting, palpitations, dizziness, tingling sensation in either arm or vague abdominal discomfort (Aroesty & Kannam, 2019). References Include at least one evidence-based peer-reviewed journal article which relates to this case. Use the correct APA 6th edition formatting. Adamson, P. D., Hunter, A., Madsen, D. M., Shah, A., McAllister, D. A., Pawade, T. A., Williams, M. C., Berry, C., Boon, N. A., Flather, M., Forbes, J., McLean, S., Roditi, G., Timmis, A. D., van Beek, E., Dweck, M. R., Mickley, H., Mills, N. L., and Newby, D. E. (2018). High-sensitivity cardiac tropinin I and the diagnosis of coronary artery disease in patients with suspected angina pectoris. Circulation: Cardiovascular Quality and Outcomes, 2018(11). https://doi.org/10.1161/CIRCOUTCOMES.117.004227 Alyavi, A., & Uzokov, J. (2017). Treatment of stable angina pectoris: Focus on the role of calcium antagonists and ACE inhibitors. e-Journal of Cardiology Practice, 15(9). Aroesty, J. M., & Kannam, J. P. (2019). Patient education: Chest pain (Beyond the basics). In B. J. Gersh (Ed.), UpToDate. Retrieved from https://www.uptodate.com/contents/chest-pain-beyond-the-basics Boden, W. E., Padala, S. K., Cabral, K. P., Buschmann, I. R., & Sidhu, M. S. (2015). Role of short-acting nitroglycerin in the management of ischemic heart disease. Drug design, development and therapy, 9, 4793–4805. doi:10.2147/DDDT.S79116 Cardinale, L., Priola, A. M., Moretti, F., & Volpicelli, G. (2014). Effectiveness of chest radiography, lung ultrasound and thoracic computed tomography in the diagnosis of congestive heart failure. World journal of radiology, 6(6), 230–237. doi:10.4329/wjr.v6.i6.230 Casu, G., & Merella, P. (2015). Diuretic Therapy in Heart Failure - Current Approaches. European cardiology, 10(1), 42–47. doi:10.15420/ecr.2015.10.01.42 Centers for Disease Control and Prevention. (2015). Preventing heart disease: Healthy living habits. Retrieved from https://www.cdc.gov/heartdisease/healthy_living.htm Lisinopril (2019). In Epocrates Essentials for Apple iOS (Version 19.6) [Mobile application software]. Retrieved from http://www.epocrates.com/mobile/iphone/essentials Marques, A. C., Calderaro, D., Yu, P. C., Gualandro, D. M., Carmo, G. A., Azevedo, F. R., Pastana, A. F., Limo, E. M. O., Monachini, M., & Caramelli, B. (2014). Impact of cardiology referral: clinical outcomes and factors associated with physicians' adherence to recommendations. Clinics (Sao Paulo, Brazil), 69(10), 666–671. doi:10.6061/clinics/2014(10)03Maxwell, C., Konoske, R., & Mark, J. (2016). Emerging Concepts in Transesophageal Echocardiography. F1000Research, 5, F1000 Faculty Rev-340. doi:10.12688/f1000research.7169.1 Ryan, A., Heath, S., & Cook, S. (2018). Dyslipidaemia and cardiovascular risk. Boston Medical Journal, 2018(360. https://doi.org/10.1136/bmj.k835 Wee, Y., Burns, K., & Bett, N. (2015). Medical management of chronic stable angina. Australian prescriber, 38(4), 131–136. doi:10.18773/austprescr.2015.042 Yoo B. S. (2014). Clinical Significance of B-type Natriuretic Peptide in Heart Failure. Journal of lifestyle medicine, 4(1), 34–38. doi:10.15280/jlm.2014.4.1.34 [Show More]
Last updated: 2 years ago
Preview 1 out of 10 pages
Buy this document to get the full access instantly
Instant Download Access after purchase
Buy NowInstant download
We Accept:

Reviews( 0 )
$18.00
Can't find what you want? Try our AI powered Search
Document information
Connected school, study & course
About the document
Uploaded On
Jun 07, 2020
Number of pages
10
Written in

Additional information
This document has been written for:
Uploaded
Jun 07, 2020
Downloads
0
Views
116
.png)
.png)
.png)
.png)
.png)
.png)
.png)